The Documentation Burden: Why NLP-Based Automation Is Under Pressure to Deliver
Clinical documentation consumes a disproportionate share of physician time. A PRISMA systematic review of 129 studies found that physicians spend 34–55% of their workday on clinical documentation, representing an estimated $90–140 billion in annual opportunity costs in the US. That figure captures time physicians are not seeing patients, not teaching, and not doing the clinical reasoning their training prepared them for.
The problem is not limited to physician time. Manual ICD coding carries error rates of up to 20%, and the US coding market is estimated at approximately $18.2 billion annually — a figure that reflects both the scale of the workflow and the cost of getting it wrong. Clinical documentation improvement (CDI) specialists spend significant effort querying physicians for clarifications on incomplete or ambiguous documentation, a process that is disruptive to clinical workflows and adds administrative overhead on both sides.
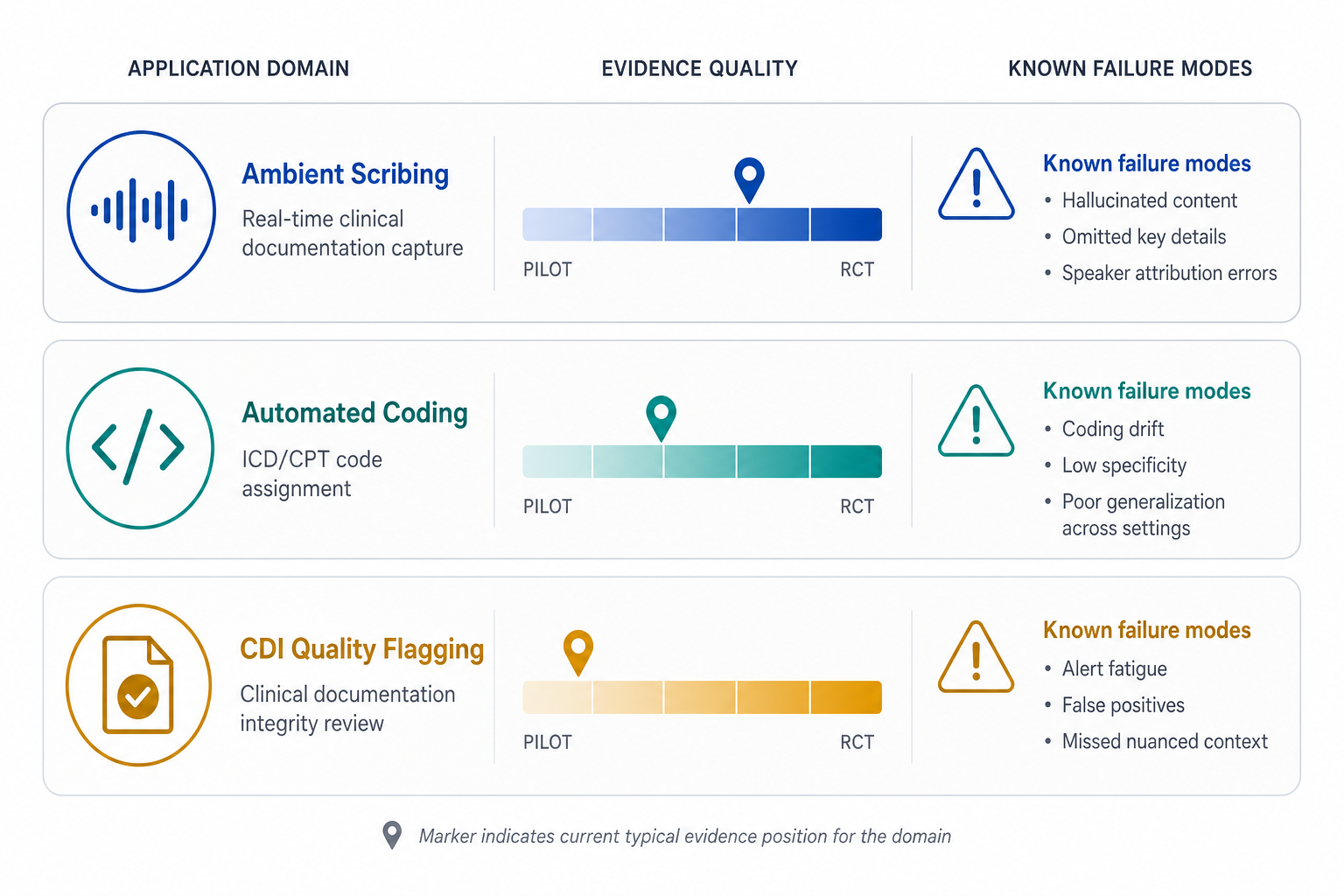
These three pressure points — physician documentation time, coding accuracy, and CDI query burden — have driven rapid commercial investment in NLP-based automation tools. The tools exist across three operationally distinct domains, each with a different NLP mechanism, a different evidence base, and a different set of deployment-stage risks. Understanding those differences is essential before evaluating vendor claims. Readers new to AI concepts more broadly may find the core AI and health concepts overview a useful starting point.

Ambient AI Scribing: What the Evidence Shows and Where It Stops
Ambient AI scribes use automatic speech recognition (ASR) combined with NLP or large language model (LLM) pipelines to convert real-time encounter audio into structured clinical notes, without requiring the physician to dictate or type. The commercial landscape includes tools such as Nuance DAX, Abridge, Nabla, and Suki — though none of these are systematically published in independent peer-reviewed literature.
A Cochrane-methods PRISMA systematic review identified only 8 eligible intervention studies evaluating AI scribes, most published between 2023 and 2024, with 75% conducted in the US. The most consistent finding across those studies was a reduction in documentation time per patient — for example, DAX users showed a decrease from 5.3 minutes to 4.54 minutes per encounter. Provider engagement scores also trended positively, with DAX users scoring 3.62 versus 3.37 for non-users on Press Ganey surveys.
The burnout evidence is weaker and should not be overstated. One study in the systematic review found no significant change in burnout scores (p=0.081), though the same study found that documentation time perception improved (p=0.005). These are different outcomes — feeling less burdened by documentation is not the same as scoring lower on a validated burnout instrument. The reviewers explicitly noted that a meta-analysis across studies was not feasible due to design heterogeneity.
A 2025 NEJM AI randomized controlled trial involving 238 outpatient physicians across 14 specialties reported significant improvements in both documentation time and burnout — the first large-scale RCT evidence for ambient scribing. This is a meaningful methodological step forward. However, a single RCT does not constitute a settled evidence base, and independent replication at scale has not yet been reported.
Real-world deployment data adds further complexity. A 2026 npj Digital Medicine analysis found substantial variation across health systems: Mass General Brigham observed a median total EHR time reduction of 5.6 minutes per appointment, while Permanente Medical Group's implementation showed only 18 seconds of savings per appointment compared to non-users, and Intermountain Health reported no statistically significant productivity gains. Consistent improvements were found in clinician well-being and patient interaction quality, but the productivity signal is far from uniform.
On note quality, the evidence is mixed. One study found that 62% of AI-generated neurology discharge summaries met standard of care — a figure that is encouraging but also means 38% did not. ChatGPT-4 showed substantial variability in errors, accuracy, and note quality, with particular difficulty on non-objective clinical data. These are not edge-case failures — they reflect systematic limitations of current LLM pipelines when applied to unstructured clinical audio.
| Finding | Effect / Result | Study / Source | Limitation |
|---|---|---|---|
| Documentation time per encounter | 5.3 min → 4.54 min (DAX users) | Systematic review (PMC12193156, 8 studies) | Small samples, heterogeneous designs |
| Provider engagement (Press Ganey) | 3.62 vs. 3.37 for non-users | Systematic review (PMC12193156) | Single survey instrument, not validated burnout scale |
| Burnout score change | p=0.081 (non-significant) | One study within systematic review | Single study, not replicated |
| After-hours EHR work | +4.69% increase for DAX users | Systematic review (PMC12193156) | Direction opposite to expected benefit |
| EHR time reduction — MGB | Median 5.6 min per appointment | npj Digital Medicine 2026 | Single health system, implementation-specific |
| EHR time reduction — PMG | 18 seconds per appointment | npj Digital Medicine 2026 | Minimal effect, different setting |
| Burnout and documentation time (RCT) | Significant improvement | NEJM AI RCT, 238 physicians, 14 specialties | Single RCT, replication pending |
| Neurology discharge summary quality | 62% met standard of care | PMC11605373 systematic review | 38% did not meet standard of care |

Computer-Assisted ICD/CPT Coding: Benchmark Promise Versus Real-World Performance
Automated coding tools use NLP concept extraction and classification to suggest ICD-10 or CPT codes from clinical documentation. The appeal is clear: manual coding has error rates up to 20% and costs approximately $18.2 billion annually in the US. Reducing those errors and costs through automation is a compelling value proposition — but the peer-reviewed evidence shows a significant gap between benchmark performance and real-world clinical note accuracy.
A 2025 npj Health Systems study evaluated LLM fine-tuning for ICD-10 coding across two conditions: structured inputs and real-world clinical notes. Before fine-tuning, LLM exact code-matching was below 1–3%. After initial fine-tuning on 74,260 ICD-10 code-description pairs, exact matching improved to 97% on structured inputs. That figure sounds impressive — until the same model is applied to real-world MIMIC-IV discharge summaries, where exact match accuracy drops to 69.2% (category-level match: 87.2%). The gap between structured input performance and real-world note accuracy is not a minor calibration issue; it reflects how differently LLMs handle the ambiguity, abbreviation, and contextual reasoning embedded in actual clinical documentation.
A separate JMIR Formative Research pilot study evaluated a two-stage pipeline using RoBERTa for lead-term extraction and GPT-4 for code assignment. Fine-tuned RoBERTa achieved F1=0.80 for lead-term extraction — a promising result for human-in-the-loop workflows. However, the downstream GPT-4 code assignment yielded an explainability F1 of only 0.305, compared to a state-of-the-art benchmark of 0.633. GPT-4 out-of-the-box correctly associated only 47% of ICD codes to official descriptions. The study's conclusion was direct: AI automation, while promising, still underperforms compared to human accuracy and lacks the explainability needed for adoption in medical settings.
Error pattern analysis from real-world clinical notes identified four documented failure categories in the npj Health Systems study:
- Information absence (42%): The clinical note does not contain sufficient information to assign the correct code.
- Diagnostic criteria insufficiency (38%): The note references a condition but does not document the criteria required for a specific ICD code.
- Clinical context misinterpretation (8%): The model assigns a code that is plausible in isolation but incorrect given the clinical context.
- Coding rule violations (12%): The model violates ICD-10 coding conventions, such as sequencing rules or exclusion codes.
A PRISMA systematic review of AI-based automated ICD coding identified six structural challenges that constrain deployment at scale: the ICD-10-CM label space exceeds 70,000 diagnostic codes; label distribution is highly unbalanced (rare codes have minimal training examples); clinical documents are lengthy and multi-topic; coding decisions lack interpretability; ethical and social consequences of coding errors are significant; and transparency about model behavior is absent. A real-world validation at a Taiwanese hospital found an NLP-driven ICD-10-CM system achieved an F1-score of 0.621 on live hospital data — demonstrating feasibility but also confirming the continued need for human verification.
The role of fine-tuning and transfer learning in improving coding accuracy is an active research area. Readers evaluating technical approaches should consult the transfer learning and fine-tuning in clinical AI reference for definitions, strategies, and governance implications.
CDI Query Flagging: A Single Real-World Study and What It Can and Cannot Tell Us
Clinical documentation improvement tools use NLP and rule-based algorithms to analyze EHR data in real time, identifying documentation that is incomplete, ambiguous, or insufficiently specific for accurate coding and quality reporting. The appeal is substantial: CDI queries are disruptive, and reducing their frequency would benefit both physicians and CDI specialists.
The peer-reviewed evidence base for this application domain is thin. The only available real-world quantified study is a 2025 observational study published in Taylor & Francis, examining an NLP and rule-based AI clinical workflow tool across 43,597 patient encounters involving 25 hospitalists at a single 726-bed US academic medical center. The tool analyzed EHR data and presented draft assessment and plan sections with documentation specificity suggestions, which clinicians then transferred manually to the EMR.
The study found that overall CDI query rates decreased from 9.2% to 7.8% (a 14.8% relative reduction, p=0.02). For active tool users specifically, the reduction was from 10.1% to 8.1% — a 20.4% relative reduction (p=0.04). Non-users saw a non-significant increase in query rates over the same period.
Beyond the conflict of interest, the study has additional design limitations that constrain its generalizability:
- Single-site observational design: Results from one academic medical center cannot be assumed to generalize to community hospitals, multi-specialty systems, or different payer mixes.
- Five-month follow-up only: CDI query rates may fluctuate seasonally, by case mix, or with hospitalist turnover. Short follow-up limits confidence in the durability of the effect.
- No randomization: Active tool users self-selected or were assigned by workflow; uncontrolled confounders (e.g., more experienced hospitalists adopting the tool, or documentation culture differences) could explain part of the observed reduction.
- No control for confounders: Simultaneous CDI education, staffing changes, or payer policy shifts during the study period were not controlled.
This is the current state of the CDI NLP evidence base: one real-world study, with a conflict of interest, at a single site, over five months. Independent replication with a rigorous design — ideally a randomized stepped-wedge or cluster RCT — is needed before adoption decisions can be grounded in strong evidence.
Cross-Domain Evidence Limitations: What the Literature as a Whole Does Not Yet Show
Across all three application domains, the peer-reviewed evidence shares a consistent set of methodological weaknesses. These are not incidental gaps — they reflect the early stage of clinical validation for NLP documentation tools and the structural barriers to rigorous evaluation in commercial deployment environments.
- Small sample sizes: Most eligible studies in systematic reviews involve dozens to low hundreds of clinicians. The AI scribe systematic review found only 8 eligible intervention studies; the ICD coding systematic review identified 8 eligible studies from 12,641 initially identified records.
- Short follow-up durations: Most studies run for weeks to months. Long-term effects on documentation quality, coding accuracy, or CDI query rates are not established.
- Retrospective and single-center designs: The majority of evidence comes from single institutions, limiting generalizability across payer environments, patient populations, and EHR configurations.
- Absence of patient outcome data: No study in any of the three domains has demonstrated that NLP documentation tools improve patient outcomes. Efficiency gains have not been linked to clinical benefit.
- Proprietary model opacity: The most widely deployed commercial tools do not disclose their training data, validation datasets, or model architecture. This makes external bias and fairness analysis structurally impossible.
- Publication decline post-ChatGPT: A 46% decrease in peer-reviewed AI CDI publications per month was observed following ChatGPT's release in November 2022, coinciding with increased proprietary model development outside peer review. The commercial landscape has outpaced the evidence base.
A highly accurate end-to-end AI documentation assistant is not currently reported in peer-reviewed literature.
That finding, from the 129-study PRISMA systematic review, is the most important single statement in the current evidence base. It does not mean that useful tools do not exist — it means that the peer-reviewed record has not yet established one that meets the bar for broad clinical implementation without mandatory human oversight.
Failure Modes and Patient Safety Risks
Documented failure modes across all three application domains represent patient safety considerations, not merely quality issues. The distinction matters: an incorrect ICD code affects billing and resource allocation; an omitted clinical finding in an AI-generated note can affect downstream care decisions.
The following failure modes are documented in peer-reviewed literature or identified in governance-focused analyses of deployed tools:
- Hallucinations: LLM-generated notes may include clinical information that was not discussed during the encounter. This is not a hypothetical risk — it is documented in studies of ChatGPT-4 applied to clinical note generation and flagged in the JMIR Medical Informatics editorial review of ambient scribes.
- Omissions of clinically significant findings: AI-generated notes may fail to capture findings that were verbally expressed but not prominently structured in the audio stream. Relevant clinical details can be systematically underrepresented.
- Note bloat from AI verbosity: LLMs tend toward verbose output. AI-generated notes may be longer than clinically necessary, embedding relevant findings within padding that increases cognitive load for reviewing clinicians.
- Clinical context misinterpretation: Models may assign codes or generate note text that is locally plausible but contextually incorrect — for example, attributing a symptom to the wrong diagnosis or misreading clinical negation.
- Multi-speaker attribution failures: In busy clinical settings with interruptions, background conversations, or multiple speakers, ambient scribes may misattribute speech to the wrong participant or include extraneous content in the note.
- Background noise interference: ASR performance degrades in high-noise environments such as emergency departments, ICUs, or multi-bed examination areas. Most published evidence comes from quieter outpatient settings.
- Automation bias: Clinicians who routinely accept AI-generated notes without critical review may gradually reduce the depth of their own verification. This risk compounds over time and is identified in the JMIR editorial as a potential source of long-term 'cognitive debt.'
Clinician review of AI-generated documentation is a clinical necessity, not an optional oversight layer. This applies equally to ambient scribe output, AI-suggested codes, and CDI tool recommendations. Any deployment model that treats clinician sign-off as a formality rather than a substantive review step increases patient safety risk.
Regulatory Status and Governance Considerations
The regulatory status of ambient AI scribes and CDI tools reflects a deliberate commercial strategy as much as a regulatory determination. Most of these tools are marketed as administrative software — not clinical decision support — specifically to avoid classification as Software as a Medical Device (SaMD) under FDA frameworks. This positioning has regulatory consequences: tools that are not classified as SaMD are not subject to FDA premarket review, post-market surveillance requirements, or performance transparency mandates.
As of mid-2026, the FDA's SaMD framework and the EU Medical Device Regulation have not provided clear, harmonized guidance on classification and risk categorization for ambient documentation and CDI tools. The npj Digital Medicine 2026 perspective notes this regulatory gap explicitly, identifying it as a barrier to consistent governance across health systems and jurisdictions.
NHS England has provided emerging governance guidance for ambient AI scribes, representing one of the more structured national-level approaches. US health systems have largely developed their own internal governance frameworks in the absence of federal requirements.
- Most ambient AI scribes and CDI tools are not FDA-regulated as medical devices as of June 2026.
- The administrative tool classification exempts these products from premarket review and performance disclosure requirements.
- Proprietary model opacity means that bias and fairness analysis cannot be conducted by external evaluators — training data and validation sets are not disclosed.
- No harmonized international regulatory classification exists for ambient documentation AI as of mid-2026.
- Health systems deploying these tools carry institutional responsibility for governance, monitoring, and clinician oversight protocols.
Adoption Framework: Evaluating NLP Documentation Tools by Domain and Evidence Tier
Healthcare professionals and procurement teams evaluating NLP documentation tools need a structured way to map evidence quality to deployment decisions. The three application domains are at different stages of evidence maturity, and the minimum evidence threshold for responsible adoption differs accordingly.
| Application Domain | NLP Mechanism | Current Evidence Tier | Strongest Evidence Available | Key Evidence Gap | Deployment Stage |
|---|---|---|---|---|---|
| Ambient AI Scribing | ASR + NLP/LLM pipeline | Limited prospective evidence; one RCT | NEJM AI RCT (238 physicians, 14 specialties); systematic review of 8 studies | No patient outcome data; heterogeneous designs; proprietary model opacity | Broad commercial deployment; evidence base still maturing |
| Computer-Assisted ICD/CPT Coding | NLP concept extraction and classification | Retrospective benchmark studies; limited real-world validation | 69.2% exact match on MIMIC-IV with enhanced fine-tuning; F1=0.621 in Taiwanese hospital validation | No peer-reviewed evidence of broad real-world deployment at scale; explainability gaps | Pilot and limited deployment; human-in-the-loop required |
| CDI Query Flagging | NLP and rule-based EHR analysis | Single observational study with conflict of interest | 20.4% relative CDI query reduction for active users (n=43,597 encounters, single site, p=0.04) | Single site, 5-month follow-up, developer-funded, no randomization | Early commercial deployment; independent replication absent |
Minimum Evidence Standards for Procurement Decisions
The following represent minimum evidence standards that procurement teams should apply when evaluating vendors in each domain. These are not endorsements of any specific threshold — they are grounded in what the peer-reviewed literature shows is currently achievable and what gaps remain.
- Require site-specific or specialty-specific validation data. Performance figures from one health system or specialty do not transfer automatically. Request validation data from a setting comparable to your own.
- Require disclosure of test dataset composition. For coding tools, ask whether accuracy was measured on structured inputs or real-world clinical notes. The difference between 97% and 69.2% exact match is entirely explained by this distinction.
- Require conflict-of-interest disclosure for any study cited in vendor materials. Developer-funded studies with developer co-authors are not disqualifying, but they require independent corroboration before forming the basis of adoption decisions.
- Mandate clinician review workflows as a governance requirement. No current NLP documentation tool has demonstrated accuracy sufficient to eliminate clinician review. Any deployment model must treat review as substantive, not ceremonial.
- Establish a post-deployment monitoring protocol before go-live. Define how hallucinations, omissions, and coding errors will be identified, reported, and corrected. In the absence of regulatory requirements, this is an institutional responsibility.
- Ask for patient outcome data — and accept that vendors likely do not have it. No peer-reviewed study in any of the three domains has linked NLP documentation tools to improved patient outcomes. This is a known gap, not a vendor oversight. It should be part of any internal evaluation framework going forward.
Comments
Join the discussion with an anonymous comment.