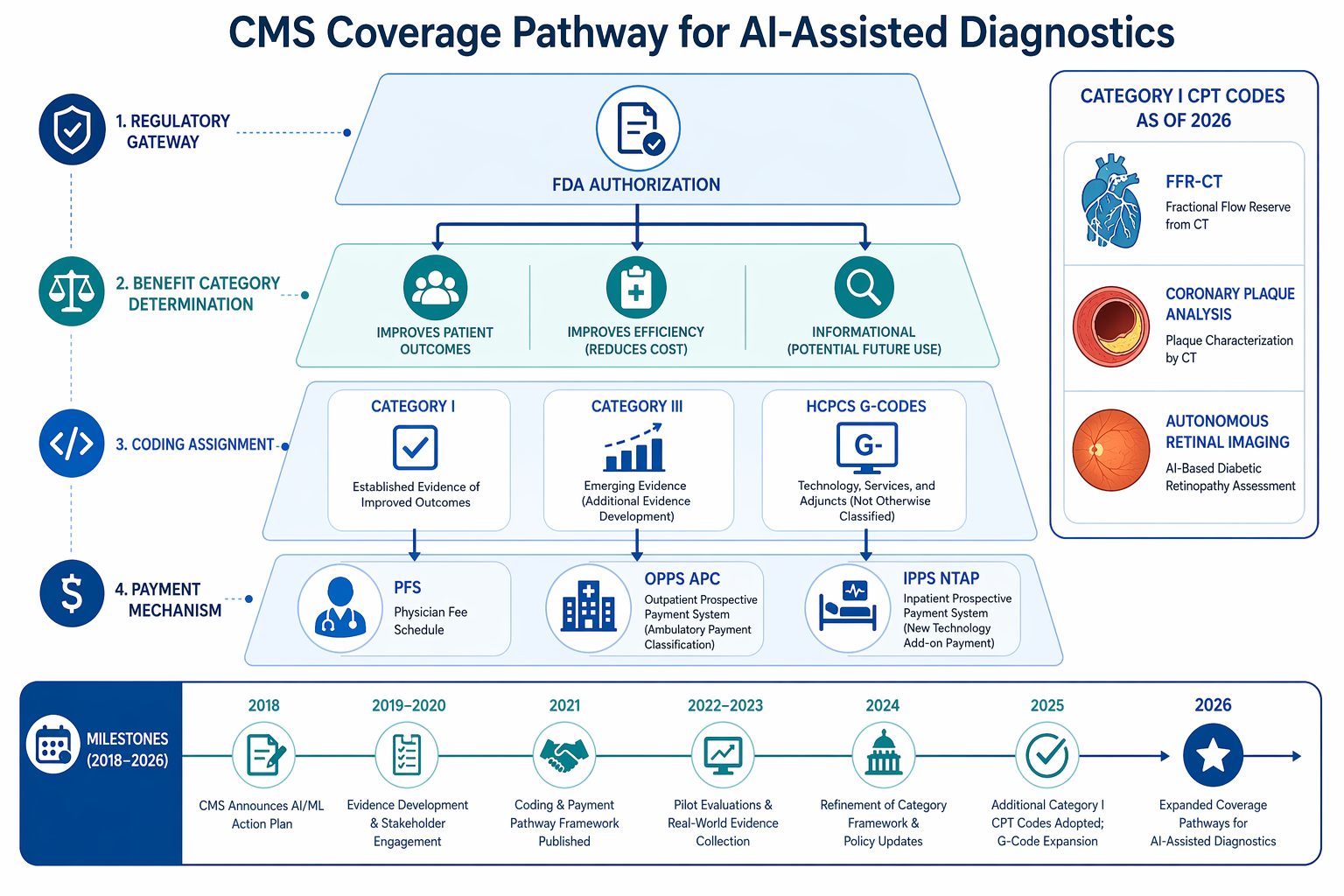
Why 2026 Is a Watershed Year for AI Diagnostics Coding
For years, providers who deployed AI-assisted diagnostic tools operated in a reimbursement gray zone. Category III CPT codes allowed data collection but offered no meaningful payment. Commercial payer coverage was inconsistent. Medicare had no dedicated infrastructure for algorithm-based services. That picture changed decisively in 2026.
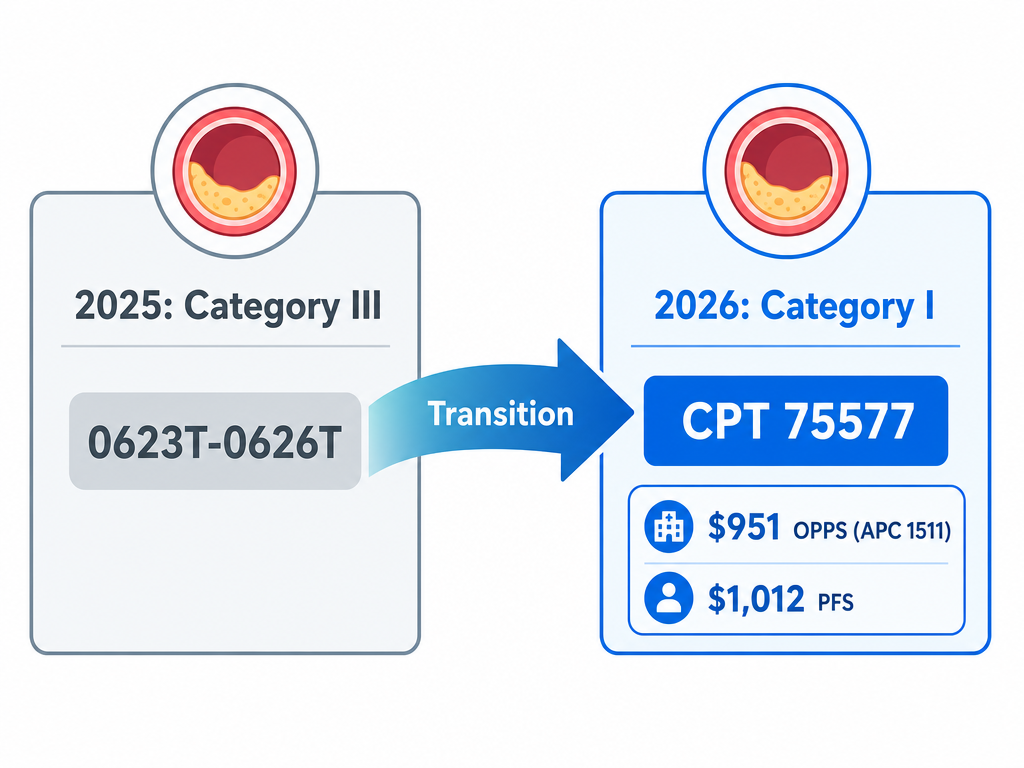
Three structural shifts define this inflection point. First, the American Medical Association's CPT Editorial Panel introduced 288 new codes across the 2026 code set, including 84 deletions and 46 revisions — the largest single-year update in recent memory. Among them, coronary plaque analysis graduated from Category III status (0623T–0626T) to a full Category I code (75577), carrying Medicare payment rates of approximately $951 under the Outpatient Prospective Payment System (APC 1511) and roughly $1,012 under the Physician Fee Schedule.
Second, CMS established HCPCS code G0680, effective April 1, 2026, for algorithmic analysis of coronary artery calcium (CAC) and aortic valve calcium (AVC) from routine chest CT. At roughly $15.50 per case under APC 1492, the code is modest in unit value but massive in addressable volume: the American Heart Association's 2025 Scientific Statement estimates that more than 17 million eligible individuals undergo chest CT annually in the United States.
Third, legislative and regulatory momentum is building. The Health Tech Investment Act (S. 1399), introduced in April 2025 by Senators Rounds and Heinrich, would create a distinct Medicare benefit category for algorithm-based healthcare services (ABHS), mandate placement into New Technology APCs, and guarantee at least five years of separate reimbursement. CMS also finalized its Transitional Coverage for Emerging Technologies (TCET) pathway in August 2024, accepting up to five candidates per year with a goal of issuing a National Coverage Determination within six months of FDA market authorization for Breakthrough Devices.
Taken together, these developments signal that CMS is building the scaffolding for scalable AI reimbursement. But the scaffolding has gaps. OPPS bundling, Multiple Procedure Payment Reduction (MPPR), and wide variation in Local Coverage Determinations (LCDs) across Medicare Administrative Contractor (MAC) jurisdictions mean that coding a service correctly is only half the battle. The other half is getting paid.
Coronary Plaque Analysis: From Category III (0623T–0626T) to Category I (CPT 75577)
The transition of coronary plaque analysis codes is the single most consequential reimbursement event for AI diagnostics in 2026. Effective January 1, 2026, CMS deleted Category III codes 0623T, 0624T, 0625T, and 0626T and replaced them with a single Category I code: 75577 (coronary atherosclerotic plaque assessment derived from augmentative software analysis of coronary computed tomography angiography).
Category I status is not merely a coding upgrade. It signals that the CPT Editorial Panel and CMS recognize AI-based plaque analysis as a clinically established, widely performed service with sufficient evidence to warrant permanent placement in the code set. Only two other AI diagnostic services have achieved Category I status: FFR-CT (computational fluid dynamics for coronary stenosis) and autonomous retinal imaging for diabetic retinopathy (CPT 9225X).
| Parameter | Category III (0623T–0626T) | Category I (75577) |
|---|---|---|
| Effective period | Prior to Jan 1, 2026 | Jan 1, 2026 onward |
| Medicare payment (OPPS) | None (data collection only) | ~$951 (APC 1511) |
| Medicare payment (PFS) | None | ~$1,012 (national average) |
| Billing requirements | Minimal | Structured LCD-compliant template required |
| Commercial payer coverage | Rare | Aetna, UHC, Cigna (~70% of insured) |
| Clinical documentation | Basic | H&P, symptoms, clinical indication for CCTA, AI analysis rationale |
CMS billing article A59813 specifies that AI-QCT/AI-CPA must be performed after the base CCTA has been completed and interpreted. The patient's medical record must document: history and physical exam, symptoms consistent with stable ischemic heart disease, clinical findings leading to CCTA, and the clinical indication for AI analysis. These documentation requirements are not optional — they are the primary reason initial denial rates for CPT 75577 run between 20% and 30%, according to data from Circle CVI.
Several AI plaque analysis tools are now FDA-cleared and commercially available, including products from Cleerly, Elucid, and HeartFlow. Readers seeking detailed device-level information — regulatory pathways, pivotal trial evidence, and real-world performance — should consult the FDA-cleared cardiology AI landscape article for a comprehensive subspecialty review.
HCPCS G0680: AI-Enabled CAC Analysis from Routine Chest CT
HCPCS code G0680, effective April 1, 2026, represents a fundamentally different reimbursement model from CPT 75577. Where 75577 pays for AI analysis of a dedicated cardiac study (CCTA), G0680 pays for opportunistic algorithmic analysis of coronary artery calcium and aortic valve calcium from chest CTs ordered for non-cardiac indications — lung cancer screening, pulmonary embolism rule-out, pre-operative evaluation, and others.
The unit economics are modest: G0680 is assigned to APC 1492 under OPPS with a national unadjusted rate of approximately $15.50 per case. But the volume opportunity is extraordinary. The AHA 2025 Scientific Statement estimates that more than 17 million eligible individuals undergo chest CT annually in the U.S., creating a massive addressable funnel for opportunistic cardiovascular screening that currently goes unrealized.
The clinical impact of acting on incidentally detected CAC is well documented. The NOTIFY-1 project demonstrated that AI-based CAC notification led to a statin prescription rate of 51.2% compared to 6.9% with usual care (Sandhu et al.). The downstream revenue implications are also significant: patients identified through G0680 screening may go on to receive CCTA (CPT 75574, ~$357) and AI plaque analysis (CPT 75577, ~$950–$1,000), creating a multi-code revenue cascade from a single $15.50 trigger.
| Code | Service | Payment (OPPS) | APC | Effective Date |
|---|---|---|---|---|
| G0680 | AI CAC/AVC analysis from chest CT | ~$15.50 | 1492 | April 1, 2026 |
| 75574 | CCTA (coronary CTA) | ~$357 | 1511 | Existing |
| 75577 | AI plaque analysis from CCTA | ~$951 | 1511 | Jan 1, 2026 |
The Hagopian et al. study published in NEJM AI (2025) validated AI-CAC algorithms across 98 VA centers, providing a multi-site evidence base that supports the clinical validity of opportunistic screening at scale. For radiology practices and health systems, G0680 represents a low-barrier entry point into AI-based cardiovascular reimbursement — the code requires no dedicated cardiac imaging, leverages existing chest CT volume, and creates a documented pathway for preventive cardiovascular care that can be tracked and measured.
Autonomous Retinal Imaging: The Precedent-Setting Category I Code (CPT 9225X)
Before coronary plaque analysis, before G0680, there was autonomous retinal imaging. CPT code 9225X was granted Category I status by the CPT Editorial Panel in May 2019, and CMS announced coverage effective January 1, 2021 — the first time Medicare reimbursed an autonomous AI system in any healthcare setting.
The system that earned this designation, LumineticsCore (formerly IDx-DR), received FDA De Novo authorization in 2018 as the first autonomous AI diagnostic system in any field of medicine. The CMS coverage decision in 2020 established a critical precedent: that an AI system operating without human interpretation of the primary image could qualify for Medicare payment under existing benefit categories, provided it met the statutory requirements for diagnostic tests.
For readers seeking the full clinical and regulatory background of the IDx-DR/LumineticsCore system — including the pivotal trial design, FDA review process, and post-market performance data — the IDx-DR clinical application profile provides a detailed evidence appraisal.
New Category III Codes in 2026: Perivascular Fat, Burn Imaging, and Cardiac Dysfunction
While Category I codes capture the headlines, Category III codes remain the primary pathway for emerging AI diagnostics to enter the Medicare coding system. The 2026 CPT update introduced several new Category III codes for AI-based services, each representing a distinct clinical use case and a potential future Category I candidate.
| Code | Service Description | Clinical Area | Reimbursement Status |
|---|---|---|---|
| 0992T | Perivascular fat analysis for cardiac risk (with concurrent CT) | Cardiology | Data collection only (Category III) |
| 0993T | Perivascular fat analysis for cardiac risk (without concurrent CT) | Cardiology | Data collection only (Category III) |
| 0972T | Multispectral imaging for burn wound assessment | Burn / Wound Care | Data collection only (Category III) |
| TBD | Detection of cardiac dysfunction via acoustic/ECG analysis | Cardiology | Data collection only (Category III) |
Category III codes serve a specific regulatory function: they allow CMS and the CPT Editorial Panel to track utilization, gather clinical data, and assess whether a service meets the threshold for Category I status. They do not, however, carry Medicare payment. Providers who perform these services must absorb the cost or bill patients directly, which limits adoption to research settings, grant-funded programs, and health systems with the financial capacity to invest in un-reimbursed innovation.
The trajectory from Category III to Category I is neither automatic nor predictable. Of the hundreds of Category III codes introduced over the past decade, only a handful have graduated. The coronary plaque analysis codes (0623T–0626T) spent approximately three years in Category III before transitioning — a relatively fast timeline driven by strong clinical evidence, multi-center validation, and commercial payer adoption. Perivascular fat analysis and AI-ECG cardiac dysfunction detection are at earlier stages of evidence generation and may follow a longer path.
For cardiology departments evaluating these tools, the existence of a Category III code is a necessary but insufficient condition for adoption. The AI in cardiology landscape article provides a broader view of FDA-cleared tools in echocardiography and ECG interpretation, many of which are still navigating the reimbursement pathway.
The AMA's CMAA Proposal and Legislative Efforts (Health Tech Investment Act)
The current coding framework — Category I, Category III, and HCPCS G-codes — was not designed for AI diagnostics. Category I codes assume a human-performed service. Category III codes assume data collection, not payment. HCPCS G-codes are temporary workarounds. None of these mechanisms adequately captures the unique characteristics of algorithm-based healthcare services: software that operates independently of the performing physician, that may be adjunctive to a primary procedure, and whose value lies in the computational analysis rather than the physician's time.
The AMA's proposed Clinical Algorithm-based Application (CMAA) classification would address this gap by creating a dedicated coding category for algorithm-based services. Under the CMAA framework, AI diagnostics would be classified separately from physician-performed services, with coding based on the computational complexity and clinical value of the algorithm rather than physician work RVUs. The proposal is still under development and has not been formally adopted by the CPT Editorial Panel.
On the legislative front, the Health Tech Investment Act (S. 1399) represents the most ambitious attempt to create a statutory reimbursement pathway for AI-enabled medical devices. Introduced in April 2025 by Senators Rounds (R-SD) and Heinrich (D-NM), the bill would:
- Define algorithm-based healthcare services (ABHS) as a distinct Medicare benefit category
- Require CMS to place qualifying AI services into a New Technology APC
- Establish payments based on manufacturer-submitted cost data
- Guarantee at least five years of separate reimbursement
- Allow reimbursement for AI services performed adjunctive to other procedures
The bill has bipartisan support and aligns with recommendations from both the Bipartisan Senate AI Working Group (May 2024) and the Bipartisan House AI Task Force (December 2024), which called for a stable reimbursement pathway for AI-enabled devices under Medicare. However, as of mid-2026, S. 1399 has not progressed past referral to the Senate Finance Committee.
Payment Mechanism Challenges: OPPS Bundling, MPPR, and LCD Variation
Getting a Category I code assigned is a necessary condition for reimbursement, but it is not sufficient. Three structural payment mechanisms can significantly reduce — or eliminate — the revenue that providers actually collect.
OPPS Bundling: APC 1511 Packages 75577 with 75574
Under the Outpatient Prospective Payment System, CPT 75577 is assigned to APC 1511 — the same APC that contains CCTA (75574). When both services are performed in the same session, Medicare pays a single bundled rate for the APC, not the sum of the individual code payments. The practical effect is that the AI plaque analysis may generate no additional revenue in the hospital outpatient setting if the CCTA is already being performed.
This bundling creates a fundamental misalignment: the AI analysis adds clinical value (quantitative plaque characterization that improves risk stratification) and requires additional computational resources, but the payment system treats it as a component of the base procedure. The Health Tech Investment Act would address this by allowing separate reimbursement for adjunctive AI services, but until that legislation is enacted, providers must navigate the bundling rules as they stand.
Multiple Procedure Payment Reduction (MPPR)
When multiple imaging codes are billed in the same session, Medicare applies the Multiple Procedure Payment Reduction, which cuts reimbursement by approximately 50% for the second and subsequent codes. For a session that includes both CCTA (75574) and AI plaque analysis (75577), the MPPR reduces the combined payment significantly below the sum of the individual fee schedule amounts.
The MPPR is particularly problematic for AI diagnostics because the AI analysis is inherently adjunctive — it is always performed in conjunction with the base imaging study. Unlike a physician interpreting a second study from a different body part, the AI service has no independent clinical indication; it exists only to enhance the interpretation of the primary study. The MPPR framework does not distinguish between truly independent second services and adjunctive AI analysis.
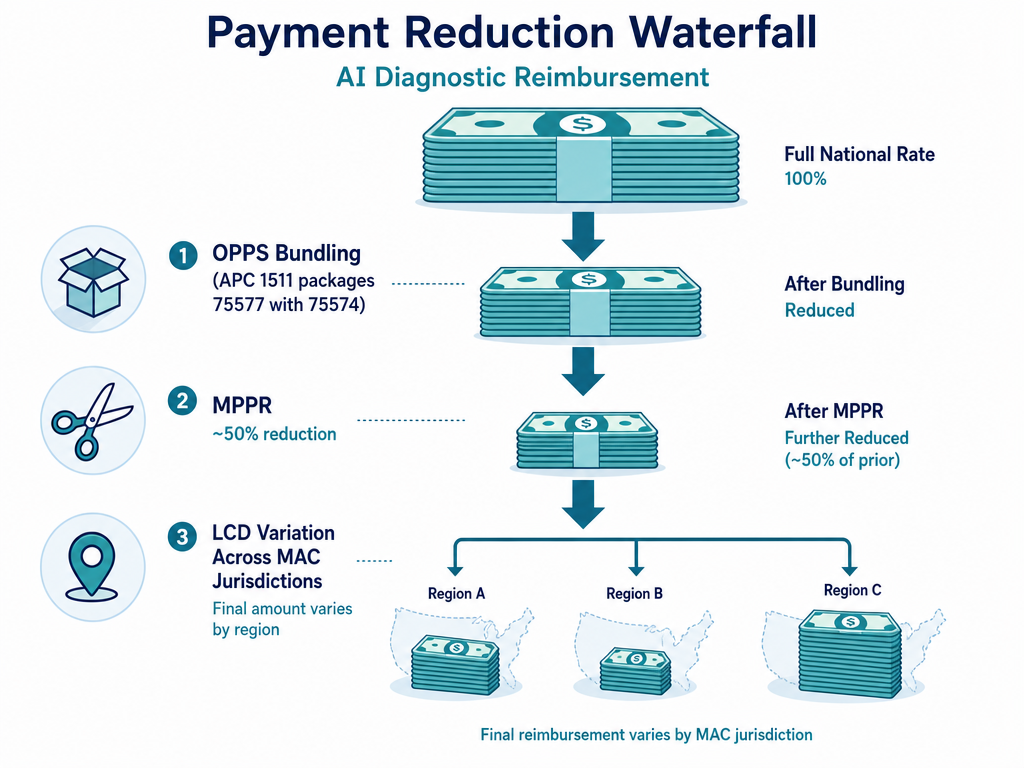
LCD Variation Across MAC Jurisdictions
Local Coverage Determinations vary significantly across Medicare Administrative Contractor jurisdictions, creating a patchwork of coverage criteria that complicates multi-site deployment. Circle CVI reports that Noridian (Jurisdiction A) applies stricter documentation requirements for CPT 75577, while Palmetto (Jurisdiction M) has broader policies. The result is that a radiology practice operating across multiple MAC jurisdictions must maintain separate billing templates and documentation workflows for each region.
| Challenge | Impact on AI Reimbursement | Mitigation Strategy |
|---|---|---|
| OPPS bundling (APC 1511) | AI plaque analysis may generate $0 incremental revenue in hospital outpatient setting | Shift to Physician Fee Schedule billing where possible; track downstream revenue from improved risk stratification |
| MPPR (~50% reduction) | Second and subsequent imaging codes in same session cut by half | Structure session to minimize concurrent imaging codes; document medical necessity for each separately |
| LCD variation across MACs | Coverage criteria differ by jurisdiction; Noridian stricter than Palmetto | Implement jurisdiction-specific LCD-compliant reporting templates; centralize template management |
| Initial denial rates (20-30%) | High administrative burden for appeals and rework | Use structured, LCD-compliant templates; train coders on AI-specific documentation requirements |
Circle CVI's data on denial rates illustrates both the problem and the solution: initial denial rates for CPT 75577 run 20–30%, but practices that implement structured, LCD-compliant reporting templates see denial rates drop to below 5%. The difference is not in the clinical quality of the AI analysis — it is in the documentation.
Operational Strategies for Maximizing Reimbursement
For radiology practices, cardiology departments, and health systems deploying AI diagnostics, the gap between coding correctly and getting paid is bridged by operational discipline. The following strategies are drawn from the experience of early adopters and the documented requirements of CMS billing articles and MAC LCDs.
Implement LCD-Compliant Reporting Templates
CMS billing article A59813 specifies that the patient's medical record must document: history and physical exam, symptoms consistent with stable ischemic heart disease, clinical findings leading to CCTA, and the clinical indication for AI analysis. A structured reporting template that captures these elements at the point of order entry — not retrospectively during coding — is the single most effective intervention for reducing denials. Circle CVI's data showing denial rates dropping from 20-30% to under 5% with compliant templates is not an outlier; it is the expected result of aligning documentation with payer requirements.
Manage OPPS Bundling and MPPR Proactively
In the hospital outpatient setting, the bundling of CPT 75577 with 75574 in APC 1511 means that the AI analysis may not generate incremental payment. Strategies to address this include:
- Billing under the Physician Fee Schedule where possible (e.g., in independent imaging centers or professional component billing)
- Documenting the medical necessity of the AI analysis separately from the base CCTA to support separate payment appeals
- Tracking downstream revenue from improved risk stratification and preventive care (e.g., statin prescriptions, follow-up testing) to build a business case that extends beyond direct code-level reimbursement
Navigate Commercial Payer Coverage
Commercial payer coverage for AI diagnostics is expanding but remains uneven. Aetna, UnitedHealthcare, and Cigna now cover AI-based coronary plaque analysis, reaching approximately 70% of insured Americans. However, coverage criteria vary: some payers require prior authorization, others require specific documentation templates, and some limit coverage to specific FDA-cleared devices. Revenue cycle teams should verify coverage for each commercial payer before submitting claims and maintain a payer-specific coverage matrix.
Prepare for Future Policy Changes
The reimbursement landscape for AI diagnostics is evolving rapidly. Practices should:
- Monitor CMS rulemaking for changes to APC assignments, MPPR policies, and LCD updates
- Track the progress of the Health Tech Investment Act (S. 1399) and the AMA's CMAA proposal
- Engage with MACs during comment periods for proposed LCDs affecting AI diagnostics
- Build flexible billing infrastructure that can accommodate new codes, revised payment rates, and changing documentation requirements
Outlook for 2027 and Beyond
The 2026 coding changes are not an endpoint — they are the beginning of a multi-year transition toward a dedicated reimbursement infrastructure for AI diagnostics. Several developments will shape the trajectory over the next 12 to 24 months.
First, the Health Tech Investment Act, if enacted, would fundamentally restructure how Medicare pays for AI services. The creation of a distinct ABHS benefit category, mandatory New Technology APC placement, and five-year separate reimbursement guarantee would address the most significant structural barriers — OPPS bundling, MPPR, and the lack of a dedicated payment mechanism. However, the bill's progress through the Senate Finance Committee remains uncertain, and even if enacted, implementation would take 18 to 24 months.
Second, CMS's Transitional Coverage for Emerging Technologies pathway, finalized in August 2024, provides a parallel track for Breakthrough Devices to obtain national coverage within six months of FDA authorization. The pathway accepts up to five candidates per year and includes an Evidence Preview and Evidence Development Plan to address evidence gaps. TCET coverage may last approximately five or more years, providing a stable reimbursement window for qualifying AI diagnostics.
Third, the pipeline of Category III codes for AI diagnostics is expanding. Perivascular fat analysis, multispectral burn imaging, and AI-ECG cardiac dysfunction detection are early-stage candidates that may progress to Category I status if clinical evidence and utilization data support the transition. The AMA's CMAA proposal, if adopted, would create a more efficient pathway for algorithm-based services to enter the code set without the current multi-year Category III waiting period.
For providers and health systems, the strategic imperative is clear: build the operational infrastructure for AI reimbursement now, while the codes and payment rates are still being defined. The practices that invest in LCD-compliant documentation templates, payer-specific coverage verification, and flexible billing systems today will be best positioned to capture the revenue opportunity as the reimbursement landscape matures.
Readers seeking a broader perspective on the clinical evidence and research landscape for AI in medicine should consult the comprehensive research overview, which covers the peer-reviewed literature across specialties and study types.