The uncomfortable starting point for agentic AI governance in healthcare is not that hospitals are ignoring governance. Many are not. The problem is that activity has moved beyond the control structures most organizations actually have.
In one 2025–2026 healthcare AI governance analysis, 64% of organizations were experimenting with or deploying agentic AI, while only 8% had governance rules specific to agentic systems. The same source reported that 84% had AI governance committees, but only 12% had implemented a formal framework such as the NIST AI Risk Management Framework.[1] That gap matters because a committee can approve a pilot without being able to revoke an agent’s credentials, constrain the PHI it sees, log every tool call, or stop the agent while it is acting.
This is where conventional AI governance starts to fray. Predictive-model governance was built around systems that generate a score, recommendation, draft, or classification for human review. Agentic systems can plan a sequence of steps, call tools, move between clinical and administrative systems, and continue executing after the impressive demo is over. The governance question is therefore not only whether the model is accurate or biased. It is who issued the agent’s credential, what context followed it, which tools it could invoke, who approved those invocations, who can interrupt it, and how its identity disappears when the work is done.

Why Model Review Is Too Small for Agentic Systems
A model-review board can ask useful questions: What data trained the model? How was performance validated? Which users are in scope? What monitoring is planned? Those questions remain relevant, but they do not cover the operational surface of an autonomous agent.
Consider a hypothetical prior authorization agent. It may read a patient record, extract diagnosis and medication history, check payer rules, draft documentation, submit a request through a portal, monitor for a response, and route denials to staff. Even if every component model has been reviewed, the risk sits in the workflow: the access token, the PHI passed between steps, the payer-system action, the exception path, the handoff to a human, and the audit trail after the fact.
That is why an agentic AI governance program in healthcare needs architecture, not just policy language. The control plane has to meet the agent at runtime. It has to know the agent exists, bind it to a permitted purpose, mediate its access, constrain its context, enforce policy while it acts, and retire it cleanly.
The UALM Pattern: Governance as an Operating Flow
The Unified Agent Lifecycle Management model, or UALM, is useful because it treats agentic governance as a lifecycle problem rather than a meeting artifact. The model describes five layers: a non-human identity registry with credential lifecycle management, an orchestration and mediation layer for tool access control, a PHI-bounded context layer with minimization policies, a runtime guardrails layer with policy enforcement and kill-switch capability, and a lifecycle and decommissioning layer for audit trails and revocation.[2]
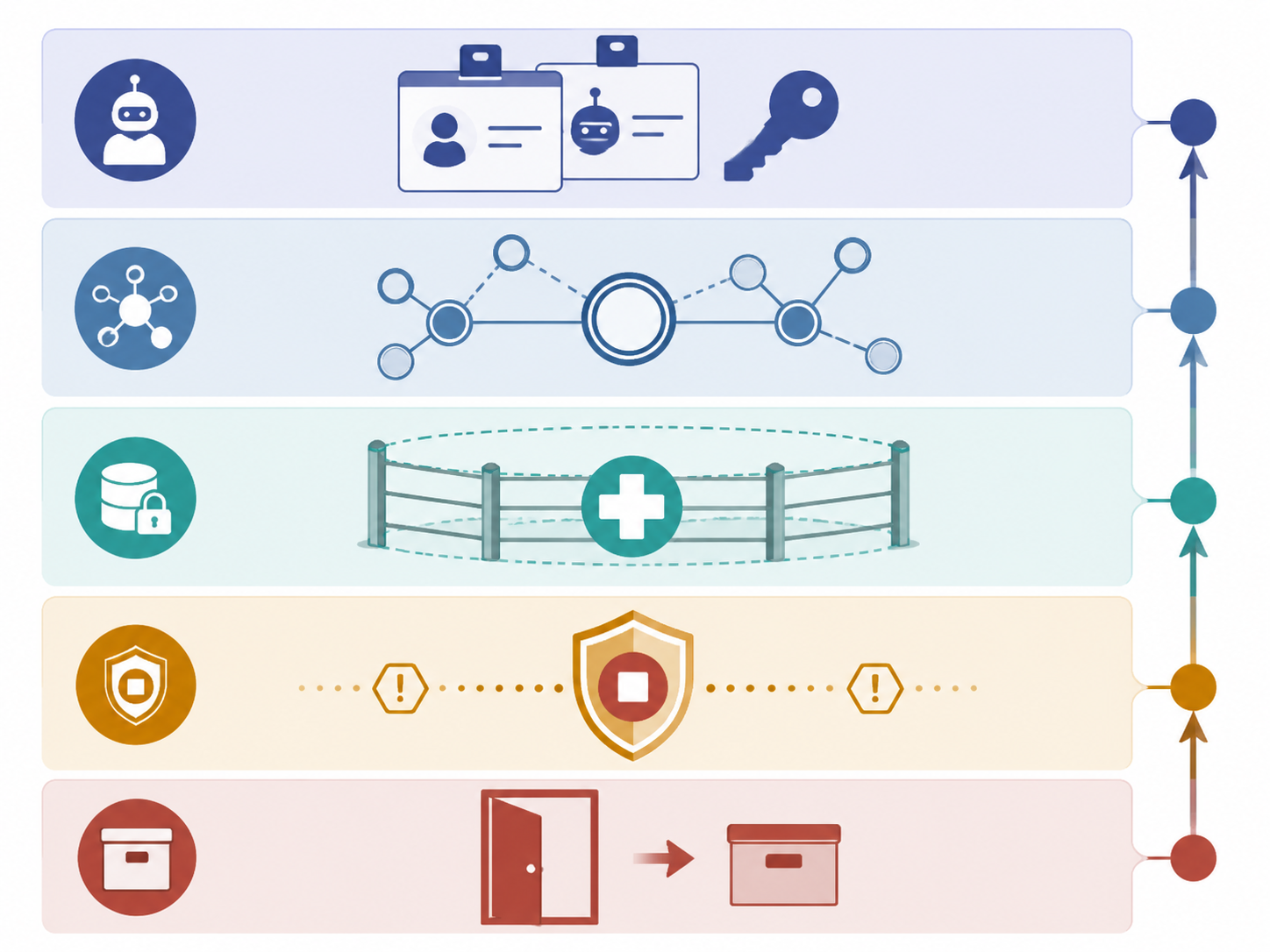
The sequence is straightforward enough to put on a procurement checklist or architecture review agenda: register the agent, issue bounded credentials, route its actions through mediated tools, limit the data context it can carry, monitor and stop it at runtime, then revoke credentials and preserve the audit record when the agent is retired.
| UALM layer | Governance question it answers |
|---|---|
| Non-human identity management | Which agent is acting, under whose authority, for what purpose, and with which credential? |
| Orchestration and mediation | Which tools can the agent call, through what approved interface, and with what approval path? |
| PHI-bounded context | What patient data can follow the agent, and what must be minimized, masked, or excluded? |
| Runtime guardrails | Which policies are enforced while the agent acts, and who can stop it? |
| Lifecycle and decommissioning | When does the agent expire, what access is revoked, and what audit evidence remains? |
Start With Non-Human Identity, Not the Use Case Deck
The first control is identity. An agent should not borrow a service account, hide inside a vendor integration, or act under a human user’s credential unless the organization is prepared to lose basic accountability. A non-human identity registry gives the agent a named, discoverable identity with an owner, scope, purpose, credential, expiration condition, and revocation path.
This sounds administrative until something goes wrong. If an agent updates a queue, submits a document, queries a record, or triggers a downstream workflow, the audit trail must distinguish the agent from the clinician, analyst, vendor, interface engine, or automation account around it. Otherwise the incident review becomes a reconstruction exercise: who authorized the action, which system actually performed it, and why did access persist after the pilot?
Good identity management also changes procurement conversations. A vendor should be able to explain how agent identities are created, rotated, constrained, monitored, and revoked. If the answer depends on a shared credential or an opaque vendor-side agent pool, the healthcare organization is being asked to accept operational risk it cannot inspect.
PHI Boundaries Have to Travel With the Agent
Agentic systems make PHI minimization harder because the data problem is no longer a single query or prompt. The agent may carry context across steps: the reason for the task, the patient attributes needed to complete it, prior tool outputs, intermediate notes, exception messages, and instructions for the next action.
A PHI-bounded context layer answers a narrower and more enforceable question than “is this system HIPAA compliant?” It asks what information the agent may see for this task, what it may retain between steps, what it may pass to a tool, what must be redacted from logs, and what should be discarded when the workflow ends.
That boundary should be purpose-specific. A scheduling agent does not need the same context as a clinical documentation agent. A claims-status agent does not need the same context as an agent drafting a response to a payer denial. If all of them receive broad record access because the integration was easier, the governance failure is already present before any model misbehaves.
Tool Calls Need Mediation, Not Trust
The orchestration and mediation layer is where autonomy becomes observable. Agents should not call clinical, revenue-cycle, identity, messaging, or document-management tools directly simply because they can. Tool access should pass through a mediated layer that checks the agent identity, task scope, data boundary, requested action, and approval requirement before execution.
The important distinction is between recommending an action and performing one. Drafting a message for staff review is one risk category. Sending the message, submitting a payer request, changing an appointment, updating a task status, or writing back into a system of record is another. The mediation layer is where those distinctions become enforceable instead of advisory.
This layer also gives clinical and operational leaders a place to define human-in-the-loop requirements without pretending every action deserves the same review. A low-risk lookup may need logging only. A write-back to a clinical workflow may require approval. A request involving sensitive data or an unusual execution path may need escalation before the agent proceeds.
Runtime Guardrails Are Where Policy Becomes Control
Policies written before deployment do not stop an agent in the middle of a bad execution path. Runtime guardrails do. They evaluate the agent’s actions while the workflow is active: whether the agent is exceeding its scope, calling tools in an unexpected sequence, attempting to carry too much PHI, repeating failed actions, or encountering a condition that requires human review.
The kill switch is not a dramatic feature. It is ordinary operational hygiene. Someone must be able to pause or terminate an agent’s execution without waiting for a vendor ticket, a change window, or a meeting. The decision rights should be explicit: clinical safety leaders may need authority to stop a workflow for appropriateness concerns, while security leaders may need authority to stop it for access, data-exposure, or abnormal-behavior concerns.
Runtime monitoring should also preserve enough detail for review. A governance committee cannot learn from an incident if it sees only that “the AI completed the task.” It needs the agent identity, tool calls, data context category, policy checks, human approvals, exceptions, overrides, and final disposition.
Decommissioning Is Part of Deployment
Healthcare pilots have a way of leaving residue: dormant accounts, lingering API tokens, unreviewed integrations, abandoned dashboards, and unclear ownership after the champion moves on. Agentic systems make that residue more dangerous because an agent identity may retain access to tools and data even after the pilot that justified it has ended.
Lifecycle governance should define expiration at the beginning. An agent approved for a limited pilot should have a time-bound credential, a named owner, a review date, a retirement condition, and a documented process for revocation. Decommissioning should remove credentials, disable tool access, archive logs, record unresolved exceptions, and confirm whether downstream systems still trust the retired identity.
What the Simulation Evidence Supports—and What It Does Not
Once the architecture is visible, the UALM simulation results are easier to interpret. In Monte Carlo simulations using synthetic data, the five-layer UALM approach reduced incident rates by 56–63% across simulated healthcare organization sizes compared with no governance. The largest projected effects were in credential revocation, with an 80% improvement; PHI minimization, with a 77% improvement; and tool-call logging, with a 57% improvement.[2]

Those are material differences, but they are not real-world outcome measurements. The authors explicitly frame the findings as model-based projections from synthetic data, not observed performance from deployed health system agents.[2] The right conclusion is that the architecture is worth serious investment and validation, not that it has already proven a specific incident-reduction rate in production.
The maturity findings are just as important as the incident-reduction numbers. The same study found that stalled governance adoption at approximately 70–74% effectiveness erased about 80% of UALM’s benefits, and only 18–21% of simulated organizations reached Level 2 maturity within six months.[2] That finding should make any executive cautious about treating agentic governance as a policy launch. Partial control is not just incomplete; in the simulation, it gave back much of the benefit.
There is also a business reason to avoid weak control designs. Gartner predicted that 40% of agentic AI projects would be canceled by the end of 2027 because of high costs, unclear value, and weak risk controls, as cited by IBM.[3] Governance is not a brake added after innovation. For many agentic projects, it may be the condition that keeps the project from being shut down.
How to Put UALM on the Governance Agenda
The practical move is to stop asking only whether an agentic AI use case has committee approval. Approval is a decision; control is an operating capability. A governance packet for an agentic workflow should show how the organization will identify the agent, constrain its access, mediate its tools, bound its PHI context, enforce runtime policy, and retire it.
- Agent registration: name, owner, sponsor, purpose, workflow scope, environment, vendor or internal builder, and expiration condition.
- Credential design: non-human identity, least-privilege access, rotation schedule, revocation authority, and prohibition on shared or borrowed human credentials.
- Tool mediation: approved tools, read/write permissions, human approval thresholds, exception handling, and logging requirements.
- PHI boundary: permitted data elements, minimization rules, retention limits, logging exclusions, and downstream sharing constraints.
- Runtime enforcement: policy checks, anomaly triggers, escalation paths, pause and kill-switch authority, and post-event review.
- Decommissioning: pilot end date, access removal, token revocation, audit archive, downstream dependency review, and final owner signoff.
This agenda also helps separate vendor claims from enterprise responsibilities. Vendor-neutral agentic governance guidance commonly emphasizes identity, access control, runtime monitoring, tool-use governance, and lifecycle oversight.[3][4] A healthcare organization still has to decide how those controls map to its EHR, identity platform, data warehouse, integration engine, messaging tools, payer connections, and security operations.
Committee Ownership Is Not Control Ownership
The existence of an AI governance committee is not trivial. It creates a forum for prioritization, review, and accountability. But agentic AI exposes the limits of committee-centered governance when no one owns the control plane. A committee can say a workflow is acceptable; it usually cannot rotate a credential, block a tool call, inspect a PHI payload, or terminate an agent at runtime.
The better model is dual accountability. Clinical leaders own safety, appropriateness, workflow fit, escalation criteria, and the conditions under which a human must review or approve an action. CIO and CISO functions own identity, access, PHI boundaries, tool mediation, runtime enforcement, auditability, and decommissioning. Privacy officers need visibility into data flows and retention. Compliance leaders need evidence that controls operated as designed, not only that policies existed.
This division avoids a familiar failure mode. Clinical leaders should not be asked to bless invisible access architecture. Security leaders should not be asked to decide whether an autonomous workflow is clinically appropriate. The governance design has to force both judgments into the same operating record.
A Credible Blueprint, Not a Proof of Safety
UALM is credible because it moves agentic AI governance from intent to enforceable runtime control. It gives healthcare organizations a concrete way to govern the handoffs that matter: identity issuance, PHI context, tool access, runtime interruption, audit review, and credential revocation.
The simulation evidence is strong enough to justify investment in that control architecture, especially given the projected reductions in incidents and the specific gains in revocation, PHI minimization, and tool-call logging. It is not strong enough to replace staged implementation, production monitoring, independent validation, and periodic review. For agentic AI in healthcare, governance should not end when the use case is approved. It should begin when the agent receives an identity and continue until that identity is gone.
References
- The Governance Gap in Healthcare AI Is Wider Than Most Leaders Realize. Censinet.
- Agentic AI Governance and Lifecycle Management in Healthcare. arXiv. May 2026.
- Agentic AI governance playbook. IBM.
- A Complete Guide to Agentic AI Governance. Palo Alto Networks.
Comments
Join the discussion with an anonymous comment.