Relapse risk rarely arrives as a clean appointment-note problem. A patient may look stable at a weekly visit, answer honestly, leave with a plan, and then move through a day shaped by pain, craving, conflict, fatigue, confidence, or the simple fact that it is a high-risk hour. By the time a clinician hears about the lapse, the clinically useful window may already have closed.
That timing problem is the strongest argument for studying AI in addiction recovery support. Substance use disorder treatment already operates in a high-relapse field: the National Institute on Drug Abuse describes relapse rates for substance use disorders as similar to those for other chronic medical illnesses, in the range of 40% to 60%.[1] The question is not whether relapse can be reduced to a score. It is whether short-term risk can be detected early enough, accurately enough, and humanely enough for care teams to do something useful.

The prediction problem changes when risk is measured in daily life
Traditional addiction care is often forced to work from sparse observations: clinic visits, urine toxicology, self-report, medication refill patterns, and the clinician’s sense of whether the person in front of them is still connected to care. Those signals matter, but they are poorly matched to a process that can change over hours.
Ecological momentary assessment, usually shortened to EMA, tries to reduce that mismatch. Instead of asking a patient to reconstruct the week from memory, EMA asks brief questions repeatedly in real-world settings. Smartphone-based studies can combine those answers with timing patterns and, in some designs, passive sensing. The result is a different clinical question: not only who is generally vulnerable to relapse, but whether this person is moving into a higher-risk period this week, tomorrow, or within the next few hours.
That distinction matters. A long-term risk profile can support treatment planning, but it does not tell anyone when to intervene. A next-day or hour-level prediction begins to resemble the kind of signal that could support a just-in-time adaptive intervention: a check-in, coping prompt, clinician outreach, medication adherence support, or other response delivered close to the period of risk. Whether those responses actually improve outcomes is still an open question. The prediction work, however, has become technically serious enough to deserve careful reading.
Alcohol lapse prediction: week, day, and hour windows
Wyant and colleagues’ 2024 study is useful because it does not treat relapse prediction as one generic task. The investigators studied 151 people with alcohol use disorder and used EMA data collected four times per day to train machine learning models for temporally precise alcohol lapse prediction across week-, day-, and hour-level windows.[2]
The reported performance is difficult to ignore: the models achieved auROC values from 0.89 to 0.93 across those prediction windows.[2] In plain clinical language, that means the models were substantially better than chance at distinguishing higher-risk from lower-risk periods in this sample. It does not mean the models are ready to run a clinic, and it does not mean every alert would be right. But it is a level of discrimination that moves the discussion beyond vague digital-health optimism.
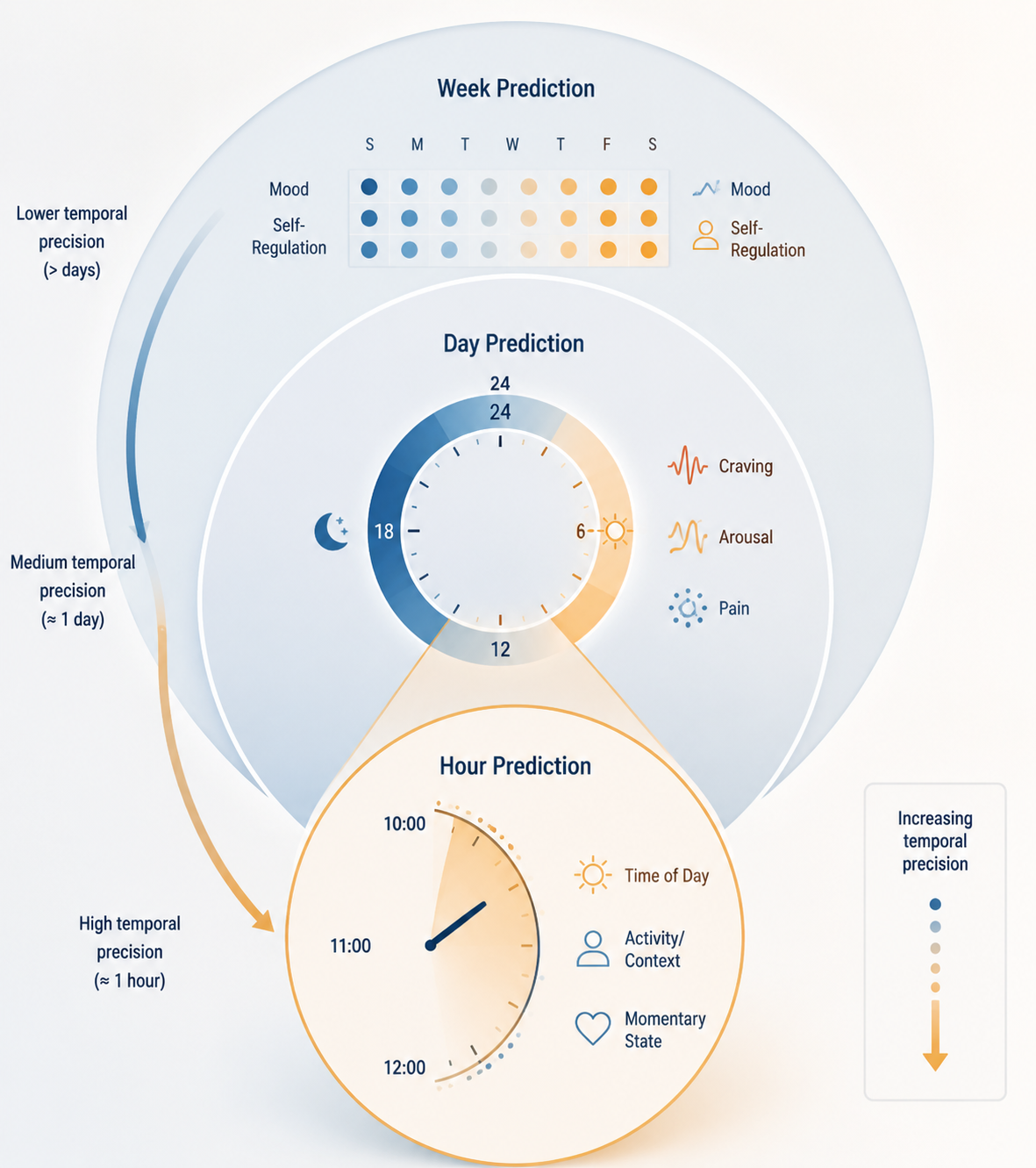
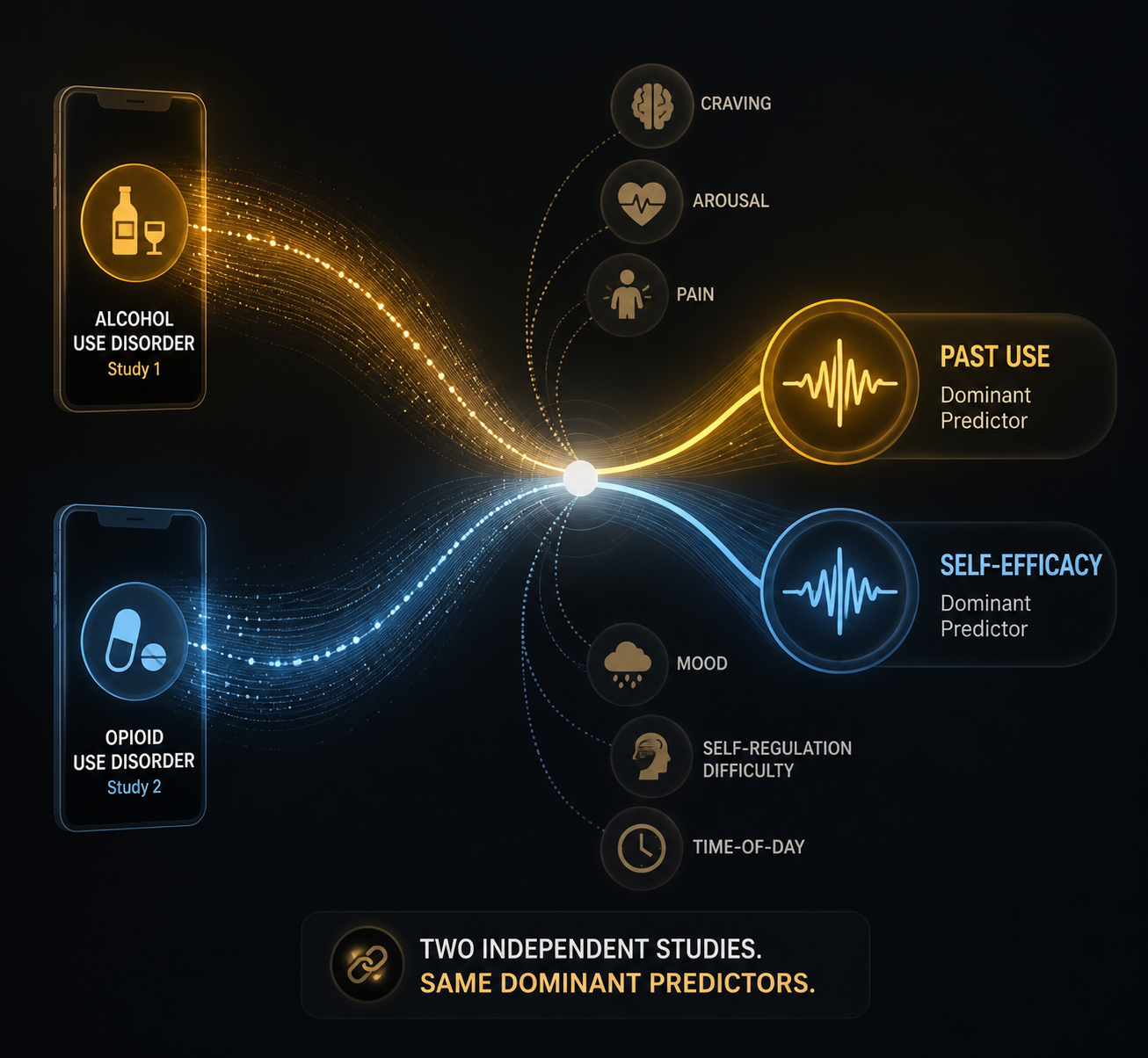
The more clinically interesting part is what the models used. Past alcohol use and self-efficacy were globally important features across prediction windows, while craving, arousal, and time of day contributed to hour-level precision.[2] That pattern is reassuring in a narrow but important sense. The model was not merely finding an opaque digital fingerprint. It was weighting signals that addiction clinicians already recognize: recent use, confidence in resisting use, momentary craving, physiological or emotional activation, and the timing of the day.
The hour-level window is where the promise becomes most concrete. A weekly risk estimate may help identify who needs more support. A day-level estimate may help prioritize outreach. An hour-level estimate, if validated and paired with an effective response, could narrow the gap between “I was doing okay” and “I used.” That is the interval addiction care often sees only after the fact.
Opioid-use prediction shows a related signal, with a smaller sample
A 2025 study summarized by Recovery Research Institute extended the same basic question into opioid-use outcomes. Heinz and colleagues analyzed daily smartphone survey data from 62 people and reported artificial intelligence models predicting next-day non-prescribed opioid use with AUC values up to 0.97.[3]
The sample size is modest, so the right response is cautious attention rather than procurement enthusiasm. Still, a next-day prediction target is clinically meaningful. It is close enough to the risky period to matter, but not so immediate that a care team has no time to respond. For opioid use, where the consequences of a lapse can include overdose risk, the difference between a general risk label and a tomorrow-risk signal is not academic.
Feature importance again pointed toward clinically legible variables. Past substance use and self-efficacy emerged as dominant predictors, converging with the alcohol findings.[2][3] That convergence is one of the most useful pieces of evidence in the current literature. It suggests that, across at least these two substance-use contexts, the strongest short-term signals are not exotic discoveries. They are familiar recovery variables measured with greater frequency and modeled across tighter time windows.
Why the features matter as much as the AUC
High model performance can be seductive, especially when the number is clean enough to fit in a slide deck. In addiction care, feature interpretability deserves nearly equal attention. A black-box warning that a patient is “high risk” may be difficult to act on without creating mistrust, alarm fatigue, or a vague sense that the patient is being watched. A risk signal tied to recent use, falling self-efficacy, rising craving, pain, mood disturbance, or self-regulation difficulty is easier to translate into care.
The current studies do not make the alert-response problem disappear. They do, however, show why smartphone data can be more than surveillance. Craving and arousal can mark acute internal pressure. Pain may be especially relevant in opioid-use trajectories. Mood and self-regulation difficulty may signal a person losing the capacity to use the coping plan they endorsed earlier. Time of day can locate risk in the rhythm of actual life rather than in a retrospective clinical summary.[2][3]
Treatment dropout is part of the same implementation problem. Related evidence suggests that dropout risk could be detected 5 to 8 days in advance using mood, self-regulation difficulties, cravings, and pain signals. That kind of lead time is clinically attractive because disengagement often precedes visible relapse. But here again, detection is not treatment. A system that predicts dropout without increasing a program’s capacity to respond may simply document abandonment earlier.
| Study focus | Data source | Prediction window | Reported performance | Clinically recognizable signals |
|---|---|---|---|---|
| Alcohol lapse prediction | Four-times-daily EMA in 151 people with alcohol use disorder | Week, day, and hour windows | auROC 0.89-0.93 | Past use, self-efficacy, craving, arousal, time of day |
| Non-prescribed opioid use prediction | Daily smartphone surveys in 62 people | Next-day use | AUC up to 0.97 | Past substance use and self-efficacy |
The evidence is promising, but not yet a clinical intervention system
The strongest current claim is narrow: machine learning models using smartphone-based self-report data can predict short-term substance use outcomes with strong discrimination in the studied samples. The weaker claim, which should be resisted, is that these models are already proven tools for improving recovery outcomes in routine care.
Several limitations sit directly between model performance and clinical readiness. Both the alcohol and opioid studies involved samples described as predominantly White and non-Hispanic, and both were recruited from single geographic regions.[2][3] That matters because relapse risk, treatment access, phone use patterns, trust in monitoring, housing stability, drug supply, and clinic responsiveness are not evenly distributed across populations or places.
Generalizability is not a ceremonial concern in addiction medicine. A model trained in one region with a relatively homogeneous sample may perform differently in a rural medication treatment program, an urban harm-reduction setting, a court-involved population, a Native community, a Spanish-speaking clinic, or a program serving people with unstable housing. The model may still work. The point is that current evidence does not yet show that it does.
There is also a missing evidence layer: randomized trials showing that ML-triggered just-in-time adaptive interventions improve outcomes. Predicting risk is a prerequisite for that kind of system, not proof that the system helps. An alert could arrive too late, too often, to the wrong person, or without an available clinician to respond. A patient could experience the alert as support, or as another form of scrutiny. A care team could use the signal to reach out skillfully, or it could become one more unmanaged queue.
Regulatory status keeps the boundary clear
The current relapse-prediction use case should also be separated from broader digital therapeutics. Some digital tools for substance use treatment have received FDA authorization, but that does not mean smartphone-based ML relapse prediction systems have been cleared for this specific clinical purpose. Current evidence places this relapse-prediction category in a pre-clearance stage, and broader reviews of artificial intelligence in addiction describe a field still working through validation, implementation, and oversight challenges.[4]
That distinction protects patients and clinicians from a common category error. A model can be scientifically impressive, clinically plausible, and still not be ready to guide care at scale. Before adoption, the relevant question is not only whether the model predicts. It is whether the prediction improves decisions, whether the response is available, whether patients understand what is being collected, and whether the system reduces harm rather than redistributing it.
For now, the evidence supports a careful middle position. Smartphone-based AI relapse prediction has moved beyond speculation: independent studies report strong AUC performance across alcohol and opioid-use outcomes, and the most important features align with recognizable relapse dynamics.[2][3] But the field has not yet shown, in diverse samples and randomized intervention trials, that acting on these predictions improves real-world recovery outcomes.
References
- Treatment and Recovery. National Institute on Drug Abuse.
- Machine learning models for temporally precise lapse prediction in alcohol use disorder. Journal of Psychopathology and Clinical Science. 2024.
- Artificial intelligence and smartphones for predicting opioid use outcomes. Recovery Research Institute. 2025.
- Artificial Intelligence in Addiction: Challenges and Opportunities.
Comments
Join the discussion with an anonymous comment.