A patient can have a reassuring clinic blood pressure, a treated LDL level, and a total PM2.5 exposure that appears to sit within an acceptable regulatory range. That does not mean the exposure history is clinically quiet. The more useful question is increasingly source-specific: how much of that fine particulate exposure came from oil combustion, coal or biomass burning, traffic, or industrial activity, and whether those sources carry the same cardiovascular signal.
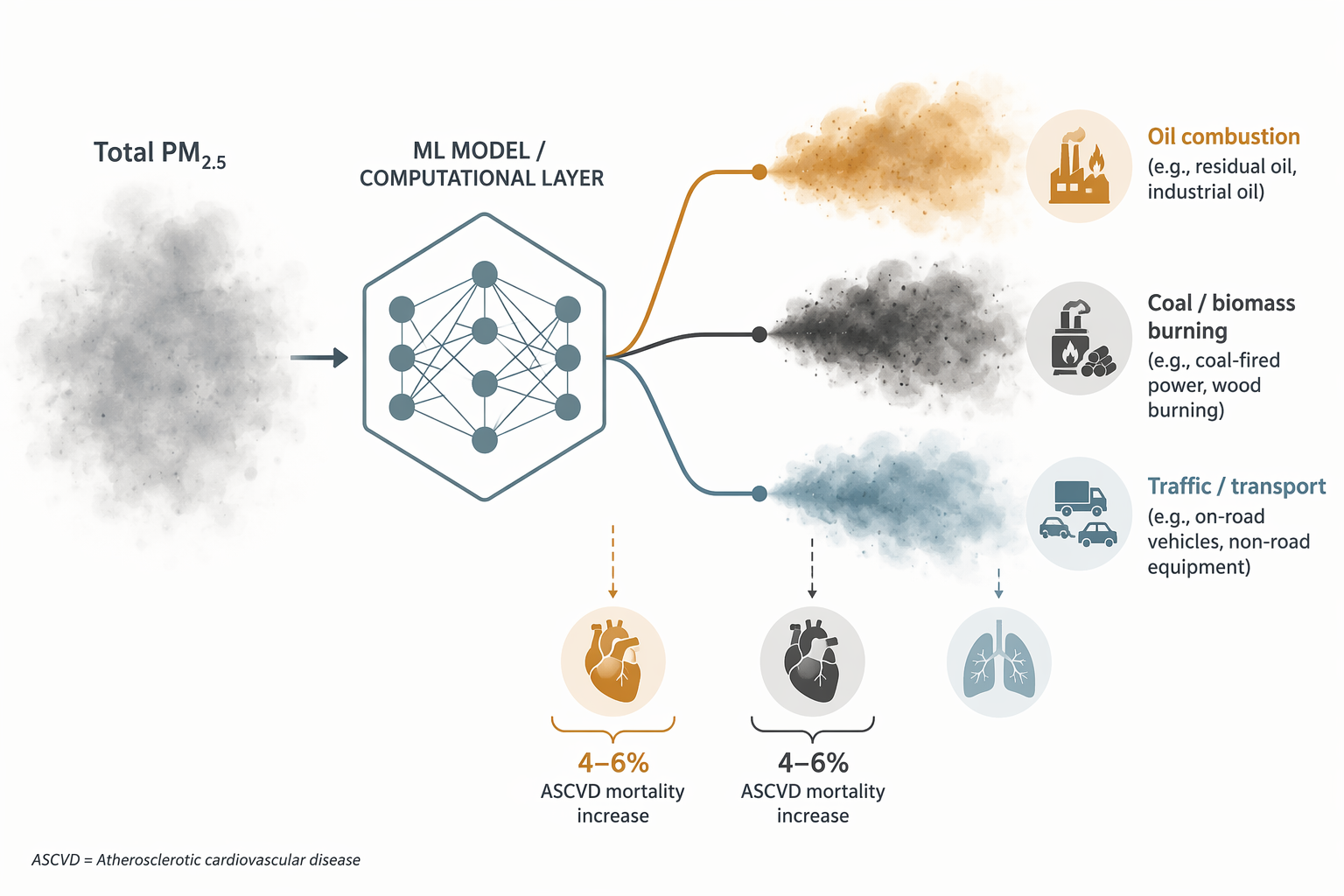
That is where AI-enhanced air quality monitoring is becoming clinically interesting. The strongest current example is a Mount Sinai-led exposomics study published in NEJM Evidence that analyzed more than 65 million US Medicare beneficiaries from 2000 through 2016 and linked source-specific PM2.5 exposure to atherosclerotic cardiovascular disease mortality. In the institutional summary of the study, oil combustion and coal/biomass burning were each associated with a 4–6% increase in ASCVD mortality per unit exposure, and the associations were observed even below current EPA air quality standards.[1]
The scale matters because ambient air pollution is not a marginal exposure. The World Health Organization attributes an estimated 4.2 million premature deaths each year to ambient outdoor air pollution, with stroke, heart disease, lung cancer, and chronic respiratory diseases among the major outcomes.[2] But population burden alone is not the clinical advance here. The advance is the attempt to make the exposure less generic.
Why Total PM2.5 Can Be Too Blunt
PM2.5 is usually handled as a total concentration: a mass of fine particles small enough to reach the distal airways and, through inflammatory and vascular pathways, contribute to cardiopulmonary risk. That summary is useful for surveillance and regulation. It is less satisfying at the bedside because it treats particles from different sources as though they were interchangeable.
A conventional PM2.5 value can obscure the composition of exposure across neighboring communities. A patient living near a highway corridor, another downwind of oil combustion, and another in an area affected by coal or biomass burning may have similar total fine-particle measurements while carrying different source profiles. If those sources differ in their association with ASCVD mortality, the total value is an incomplete risk descriptor.
Machine learning does not solve this by being “smarter” in a vague sense. Its contribution is more concrete: models can integrate monitoring data, emissions inventories, land-use patterns, meteorology, and spatial features to estimate how much PM2.5 at a given place and time is attributable to particular sources. Random forest, gradient boosting, and related source-apportionment approaches can then be linked with health outcomes at scales that would be impractical with monitor-only exposure summaries.
| Exposure Question | Conventional Summary | AI-Enhanced Source-Apportionment Question |
|---|---|---|
| How much fine particulate matter is present? | Total PM2.5 concentration | Total PM2.5 plus estimated source contributions |
| Where did the exposure come from? | Often not specified in clinical interpretation | Oil combustion, coal/biomass burning, traffic, industrial, and related source categories |
| What does the estimate support? | Broad population exposure assessment | More specific epidemiologic and population-health risk interpretation |
| What does it not yet provide? | Individual causal attribution | A validated patient-level treatment threshold |
The Mount Sinai Study Is Clinically Useful Because It Separates Sources
The Mount Sinai study is the central evidence because it does three things many air pollution analyses do not do together. It uses a very large Medicare population, covers a long time window, and estimates source-specific PM2.5 rather than stopping at total particulate burden. The cohort size—more than 65 million beneficiaries—and the 2000–2016 observation period give the analysis unusual statistical reach for ASCVD mortality questions in older adults.[1]
The source distinction is the clinically important part. In the Mount Sinai summary, PM2.5 attributed to oil combustion and coal/biomass burning showed the clearest reported association, with each unit increase linked to a 4–6% increase in ASCVD mortality.[1] That figure should not be inflated into a bedside command. It is an epidemiologic association, not a rule that tells a clinician to start or intensify a medication for one person because a modeled source contribution crossed a line.
Still, 4–6% is not trivial when it is distributed across millions of older adults already carrying competing cardiovascular risks. In cardiology, small relative shifts can matter when baseline risk is high and exposure is chronic. A modest association tied to a common exposure may affect population mortality more than a larger association tied to a rare exposure. That is why the finding deserves attention without being over-sold.
The below-standard result is also important. The reported risk persisted at exposure levels below current EPA air quality standards.[1] That does not prove that the standard is wrong for every pollutant mixture or every community. It does mean that a threshold built around total concentration may miss source-specific risk gradients. For clinicians, the immediate implication is not to reinterpret EPA compliance as danger; it is to stop treating regulatory compliance as equivalent to absence of exposure-related cardiovascular risk.
What a 4–6% ASCVD Mortality Increase Can and Cannot Mean
A 4–6% increase in ASCVD mortality per unit exposure is a relative association tied to a modeled exposure unit. It is not a patient’s absolute risk increase, and it is not interchangeable with a hazard estimate from a randomized intervention. Before it enters clinical decision-making, the exact exposure unit, model specification, adjustment strategy, confidence intervals, and sensitivity analyses need to be checked in the full NEJM Evidence manuscript, especially because the effect-size wording available in the research materials comes from an institutional press release rather than from an extracted manuscript table.[1]
For cardiovascular prevention, the most defensible use is contextual. Source-aware exposure data can help explain why observed risk may be higher than a conventional risk profile suggests, particularly in older patients, patients with established ASCVD, and communities with persistent exposure to combustion-related pollution. It may also help population health teams identify neighborhoods where prevention outreach, medication adherence support, blood pressure control, smoking cessation services, or cardiopulmonary screening deserve more attention.
At the individual bedside, the signal is softer. A clinician should not tell a patient that oil-combustion exposure caused their myocardial infarction based on these data. Nor should a modeled source contribution override standard risk assessment. But it can sit beside social history, occupational exposure, housing conditions, heat exposure, and access-to-care barriers as part of a more honest account of risk. Many patients do not live in the “average” environment assumed by risk equations.
The Medicare population also shapes interpretation. Older adults have higher baseline ASCVD risk, more comorbidity, and more vulnerability to inflammatory or hemodynamic stressors than many younger populations. That strengthens the clinical relevance for geriatric cardiology and primary care, but it limits generalization. The same association should not be casually transferred to children, young adults, or non-US populations without additional evidence.
Respiratory Risk Is a Secondary Signal, Not a Side Note
The Mount Sinai result is primarily a cardiovascular story, but clinicians rarely see cardiovascular and respiratory vulnerability in isolation. COPD, asthma, heart failure, ischemic heart disease, and frailty often cluster in the same patients and the same neighborhoods. Source-specific PM2.5 estimates therefore have plausible relevance beyond ASCVD mortality, even when the article’s strongest evidence remains cardiovascular.
A systematic review of machine learning applications for air pollution health impact assessment described work across cardiovascular disease, respiratory disease, perinatal outcomes, cancer, and COVID-19 mortality.[3] The review supports a broader conclusion: ML methods are already being used to connect pollutant exposure patterns with multiple health outcomes. It does not, by itself, establish that every model is clinically deployable or that every pollutant-source association is causal.
The JACI review on artificial intelligence in air pollution and health research similarly frames AI as a set of methods for exposure estimation, pattern detection, and risk modeling, while emphasizing unresolved methodological issues.[4] For respiratory medicine, the relevant outcomes include asthma exacerbations, COPD, and reduced lung function, but the evidence should be read as consistent association across studies rather than as a completed clinical algorithm.
That distinction matters in clinic. If a patient with COPD reports worsening symptoms during periods of visible smoke or local combustion activity, source-aware monitoring may eventually give clinicians a better exposure history than regional PM2.5 alone. But current evidence does not support prescribing a specific respiratory intervention solely because an AI model attributes a fraction of PM2.5 to one source rather than another.
What AI Adds—and Where It Can Mislead
The best use of AI in this setting is not automation for its own sake. It is resolution. Health risk models are often asked to work with exposures that are averaged over space, time, and source. Machine learning can reduce some of that averaging by estimating local source contributions and by detecting nonlinear or interacting exposure patterns that conventional regression may miss.
Interpretability tools such as SHAP values are helpful because they can show which features contributed most to a model’s prediction. For clinicians, that is a bridge from black-box output to plausible exposure narratives: oil combustion mattered more here, traffic there, meteorology somewhere else. But SHAP is not a causal test. It explains model behavior; it does not prove that changing a source would change an outcome by the same amount.
This is where enthusiasm needs discipline. A model can be well calibrated and still reflect confounding. It can identify a high-risk exposure pattern and still fail when transported to a different region, age group, housing pattern, or emissions mix. It can produce a stable association while missing the policy-relevant causal pathway. These are not reasons to ignore the findings; they are reasons to keep the interpretation proportional.
The Caveats Are Part of the Evidence, Not Fine Print
Several limitations should travel with any clinical reading of this literature. First, the Mount Sinai effect sizes available here come through an institutional study summary, so the full manuscript should remain the source of record for method details, uncertainty intervals, and robustness checks.[1]
Second, Medicare data are powerful but not universal. They privilege older US adults and the administrative structures used to capture their diagnoses and mortality. That is appropriate for ASCVD mortality in aging populations, but it does not answer how the same exposure patterns operate in younger workers, pregnant patients, children with asthma, or populations outside the United States.
Third, source-apportionment models depend on the quality of their inputs. Emissions inventories, monitoring networks, meteorologic data, and spatial proxies vary by geography. Areas with sparse monitoring or rapidly changing emissions may be modeled with more uncertainty than the final exposure surface makes obvious.
Fourth, the causal question remains open. Difference-in-differences designs, instrumental variables, natural experiments, and other causal inference methods are still needed to estimate what happens when source-specific exposure changes. Without that step, it is premature to set exposure-source clinical action thresholds or to claim that one modeled source contribution requires a specific medical response.
How Clinicians Can Use the Signal Now
The most practical near-term use is risk context. In cardiovascular clinics, source-aware exposure information can help explain residual risk in patients whose traditional factors appear controlled. In primary care, it can inform community-level prevention priorities. In pulmonary care, it can sharpen environmental histories for patients whose symptoms fluctuate with local pollution patterns.
- Use source-aware exposure data as a contextual risk signal, not as a standalone indication for treatment.
- Pay particular attention to older adults, patients with established ASCVD, COPD, asthma, or multimorbidity, and communities with persistent combustion-related exposure.
- Avoid equating compliance with current PM2.5 standards with absence of clinically relevant exposure risk.
- Treat model explanations as aids to interpretation rather than proof of causality.
- Look for full-methods validation before using any exposure-specific threshold in patient-level decision-making.
For health systems, the implications may be more immediate than for individual prescribing. If source-apportioned PM2.5 maps identify neighborhoods with persistent oil combustion or coal/biomass-related exposure, those data can be layered with ASCVD prevalence, hospitalization patterns, medication access, and preventive care gaps. That is not precision medicine in the narrow genomic sense, but it is a more precise account of risk environment.
The Mount Sinai findings make air pollution less of a background variable and more of a measurable risk context. AI-enhanced monitoring is beginning to show which pollution sources matter most for particular outcomes, and the reported persistence of ASCVD mortality associations below current EPA standards should make clinicians cautious about relying on total PM2.5 thresholds alone. The evidence is strong enough to inform cardiovascular and respiratory risk interpretation; it is not yet strong enough to function as an individual-level clinical directive.
References
- New study using machine learning links air pollution exposure to increased risk for atherosclerotic cardiovascular disease, Mount Sinai Exposomics
- Ambient (outdoor) air pollution, World Health Organization
- A federated learning framework for air pollution health impact assessment, PMC
- Opportunities for using artificial intelligence in air pollution and health research, Journal of Allergy and Clinical Immunology, 2024
Comments
Join the discussion with an anonymous comment.