The useful question for AI in air quality monitoring and health alerts is not whether a model can notice that smoke, PM2.5, humidity, oxygen saturation, prior exacerbations, and neighborhood context all matter. It is whether those signals can be combined early enough, and reliably enough, to change what happens to a patient with asthma or COPD before the ED triage note is written.
The disciplined answer is: yes, research models can predict clinically meaningful respiratory risk, often 1 to 5 days ahead or at the point of ED presentation, with discrimination that would make most clinicians pay attention. Across key studies, machine learning models have reported AUC or C-statistic values around 0.80 to 0.90 for asthma or COPD exacerbation-related outcomes. But the second half of the answer matters just as much: no prospective clinical trial in this evidence set has shown that AI-driven air-quality or respiratory-risk alerts reduce ED visits, hospitalizations, or other hard patient outcomes.

The Prediction Signal Is Real, But It Is Still Mostly Retrospective
Patel and colleagues are a useful place to start because their model sits close to a real clinical decision point: pediatric asthma patients at ED triage. In a cohort of 29,392 children, a gradient boosting machine predicted hospitalization with an AUC of 0.84 using variables that included oxygen saturation, respiratory rate, weather measures, and socioeconomic status.[1] That combination is clinically plausible. A child breathing fast with lower oxygen saturation during an unfavorable weather window is not just a row in a dataset; that is the patient whose disposition decision already requires attention.
Goto and colleagues looked at ED disposition for asthma and COPD exacerbations and found that gradient boosting machines and XGBoost reached C-statistics of 0.80 to 0.83, outperforming logistic regression.[2] The point is not that logistic regression has suddenly become obsolete. It is that tree-based boosting methods can represent nonlinear interactions more comfortably: a respiratory rate value may mean something different when paired with age, oxygen saturation, prior ED use, weather conditions, or comorbidity. Clinicians reason this way already; the model can search those combinations at scale.
Zein and colleagues reported an acute asthma exacerbation model with an AUC of 0.88.[3] Tong and colleagues then pushed the scale further, using 71 EHR features from 82,888 patients to predict 12-month asthma exacerbation risk with XGBoost. Their model reported an AUC of 0.90, accuracy of 91%, and specificity of 91%.[4] That is a different task from predicting tomorrow’s smoke-associated flare, but it shows the same pattern: when clinical history is represented in sufficient detail, machine learning can sort patients into risk strata with meaningful discrimination.
| Study | Population or setting | Prediction target | Reported performance | What it does and does not prove |
|---|---|---|---|---|
| Patel et al. 2018 | 29,392 pediatric asthma ED triage encounters | Hospitalization | AUC 0.84 | Shows clinically relevant triage prediction using clinical, weather, and socioeconomic variables; does not show that alerts improve outcomes |
| Goto et al. 2018 | ED asthma and COPD exacerbations | Disposition | C-statistic 0.80–0.83 | Shows boosted models can outperform logistic regression for ED disposition prediction; remains a model-performance result |
| Zein et al. 2021 | Acute asthma exacerbation prediction | Acute exacerbation | AUC 0.88 | Adds to the consistent high-discrimination signal; does not establish alert-driven clinical benefit |
| Tong et al. 2021 | 82,888 patients with EHR features | 12-month asthma exacerbation risk | AUC 0.90; accuracy 91%; specificity 91% | Shows strong longer-horizon risk stratification; not the same as a near-real-time air quality alert trial |
AUC values in this range are not trivial. They mean the model is often ranking the patient who will worsen above the patient who will not. But AUC is not a phone call, a steroid prescription, an inhaler technique check, or a safe decision to avoid all of those. It also says little about calibration at the bedside: whether a reported 20% risk actually behaves like 20% risk in a different city, during a wildfire season, or in a clinic serving patients with different housing, transportation, and medication-access constraints.
Why Air Quality Belongs in the Model
The environmental part of this problem does not need much embellishment. Ambient air pollution is associated with major global health burden; the National Institute of Environmental Health Sciences states that it contributes to more than 6.5 million deaths annually worldwide, and notes that PM2.5 from coal has been associated with mortality risk twice as high as PM2.5 from all sources.[5] For asthma and COPD care, the practical issue is narrower: PM2.5, wildfire smoke, ozone-relevant weather, temperature shifts, and humidity can alter airway risk on a time scale that is shorter than the next scheduled visit.
That makes respiratory prediction a data-fusion problem rather than a pure air-monitoring problem. A bad outdoor air day does not mean every patient needs the same intervention. A stable patient with good control, reliable medication access, and no recent exacerbations is not the same as a patient with frequent ED visits, low baseline lung function, missed controller fills, and a bedroom window facing a smoke corridor. A useful alert system has to join exposure conditions with susceptibility.
The Clinical Workflow Is Where Prediction Becomes Fragile
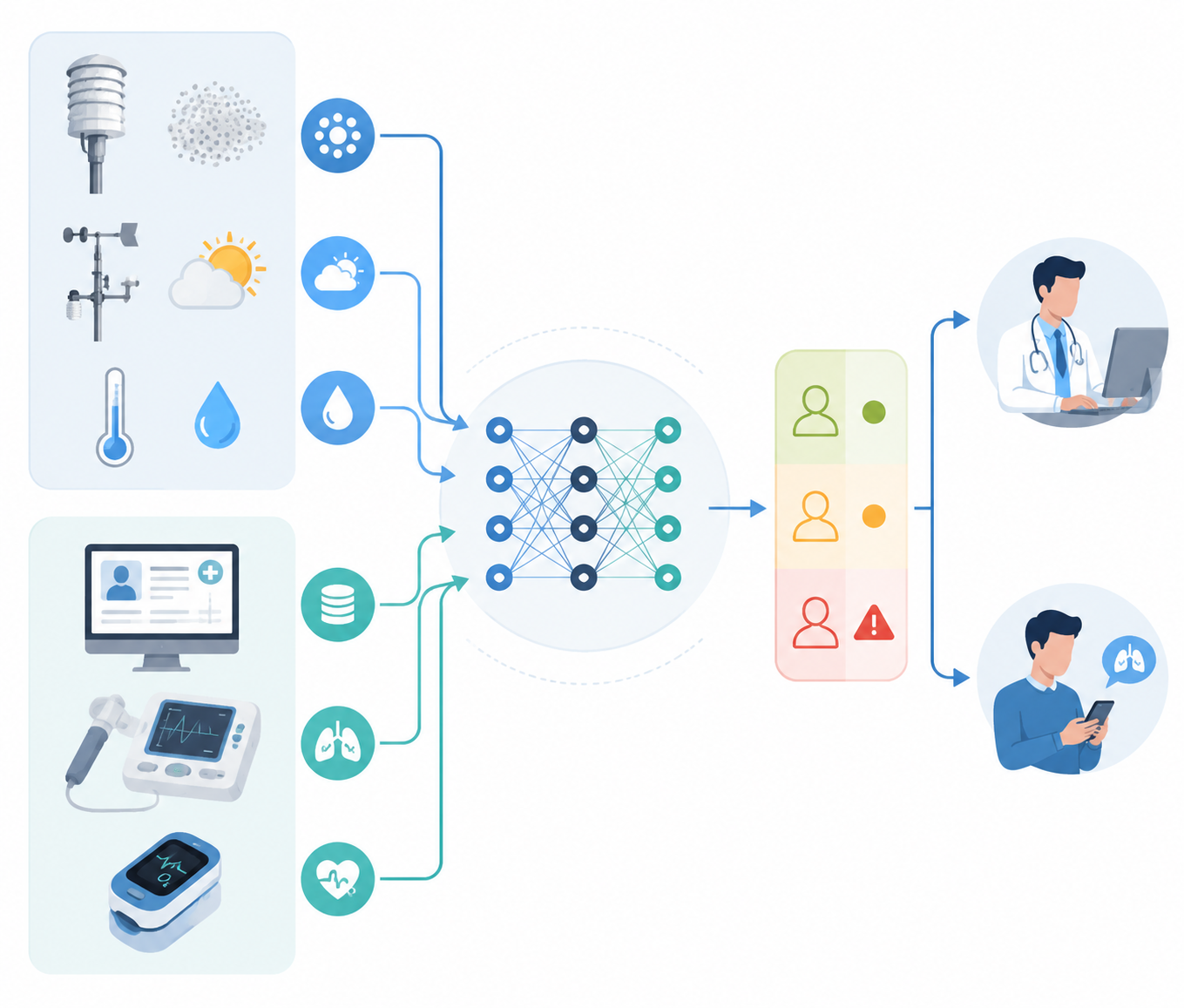
A credible AI respiratory alert system would have four moving parts. Environmental feeds would describe the exposure window. Clinical data would identify who is vulnerable. A model would estimate risk. Then an alert would have to land somewhere: in a patient app, a nurse pool, a respiratory therapist queue, an ED risk banner, or a pulmonologist’s inbox.
Each handoff changes the safety question. A model can estimate that a patient’s exacerbation risk is rising, but the next step depends on local protocol. A nurse may review symptoms and rescue inhaler use. A respiratory therapist may check inhaler technique or nebulizer access. A clinician may adjust treatment only if symptoms, peak flow, or recent medication history support that decision. A patient-facing message may advise avoiding smoke exposure, but that advice is limited if the patient cannot stay indoors, lacks filtration, or works outside.
This is why an alert threshold is a clinical policy, not only a model parameter. If the threshold is too low, teams inherit repeated warnings with unclear actionability. If it is too high, the model becomes a late alarm. During a prolonged smoke event, the same high-risk patient could be flagged again and again. Someone has to decide whether repeated alerts trigger repeated outreach, temporary suppression, escalation, or documentation that no safe additional action is available.
- Who receives the first alert: patient, nurse, respiratory therapist, primary care clinician, pulmonologist, or ED team?
- What time window does the risk estimate cover: same-day, 48-hour, 5-day, or 12-month risk?
- What action is allowed without a visit: symptom check, medication reconciliation, trigger counseling, peak-flow review, or urgent evaluation?
- How are repeat alerts handled during wildfire smoke or stagnant-air episodes?
- Who audits false positives, false negatives, calibration drift, and disparities in alert delivery?
AirNow Shows What Mature Public Alerting Already Does
The AirNow Fire and Smoke Map is not an individualized asthma prediction model, and it should not be judged as one. Its value is operational clarity. It combines current air quality conditions, smoke context, health guidance, and location-aware access in a form that patients, clinicians, schools, and public agencies can understand quickly.[6] That maturity matters. Many AI proposals underestimate how much work is required simply to make an environmental warning visible, interpretable, and usable at the moment someone needs it.
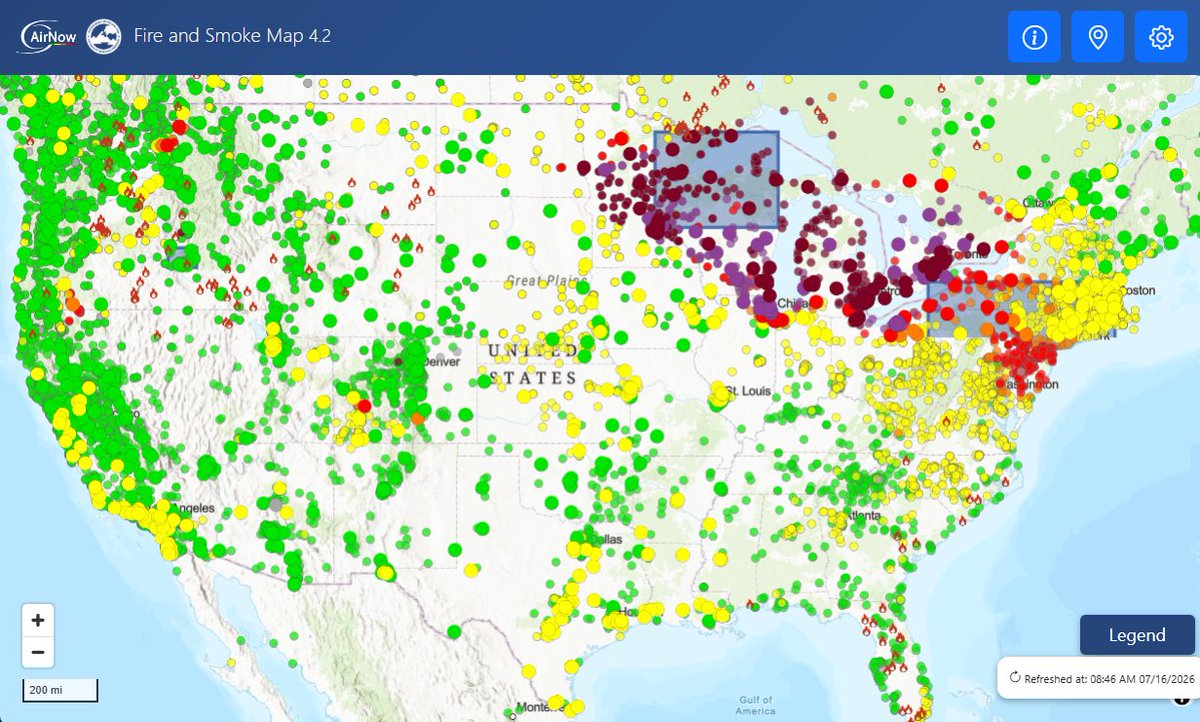
For a clinician, AirNow often functions as shared context. A patient reports worse wheeze; the map shows smoke and degraded air quality; counseling about exposure reduction becomes more concrete. But AirNow does not know the patient’s recent ED use, controller adherence, oxygen saturation, spirometry, pregnancy status, transportation barriers, or whether a prior steroid burst was complicated. That is the gap AI systems are trying to fill.
The distinction is important because public alerts and clinical alerts fail in different ways. A public map can be broad and still useful. A clinical alert that is broad can become noise. The clinical version needs patient-level relevance, a defensible threshold, and an accountable response path.
Wearables Make the Future More Personal, and More Difficult to Validate
AirPredict points toward a more individualized version of the field. In a 2025 feasibility study, Atzeni and colleagues integrated a wearable air quality sensor, spirometer, and smartwatch for asthma self-management. The study included 16 participants and reported Single Ease Question usability scores of 5.5 to 6.9 out of 7, a patient System Usability Scale score of 63 out of 100, and a clinician SUS score of 81 out of 100.[7] Those numbers are encouraging for usability, especially from clinicians, but they are not outcome evidence.
A wearable sensor also shifts the quality-control problem from a public monitoring network to a device carried through daily life. Calibration drift, placement, humidity, charging behavior, and missing data can all change the signal. If a model is trained on one sensor behavior and deployed after that behavior changes, the alert may look precise while the measurement underneath it has degraded.
Rajesh and colleagues describe another forward-looking approach: a machine learning framework that integrates random forest, gradient boosting, XGBoost, and LSTM models with SHAP-based interpretability to generate health risk maps and alerts every 5 minutes.[8] Conceptually, this is where the field is heading. LSTM models are designed to handle time sequences, which is useful when air quality and weather change hour by hour. SHAP methods try to show which features pushed a prediction upward or downward, which can help clinicians decide whether an alert is plausible rather than mysterious.
Interpretability should not be oversold. A SHAP display can explain the model’s behavior; it does not prove the model is right, fair, calibrated, or clinically useful. Still, if an alert says risk rose because PM2.5 increased, rescue inhaler use rose, oxygen saturation fell, and the patient had two recent exacerbations, that is easier to trust and audit than a red icon with no explanation.
The Missing Trial Is an Alert Trial, Not Another Dashboard
The next evidentiary step is not simply a larger retrospective AUC. Larger and more diverse validation sets are needed, but the field also needs prospective testing of alert-driven care pathways. That means randomizing or otherwise rigorously comparing what happens when a risk prediction is actually routed to a care team or patient with a predefined action protocol.
The outcome measures should match the claim. If the claim is clinical prevention, then ED visits, hospitalizations, symptom burden, oral corticosteroid use, missed school or work, and adverse effects from unnecessary treatment belong on the table. If the claim is workflow support, then response time, alert burden, clinician acceptance, equity of outreach, and override reasons matter. Feasibility and usability are necessary, but they do not substitute for clinical benefit.
Generalizability also has to be measured rather than assumed. A model developed in one health system may not travel cleanly to another region with different wildfire exposure, housing quality, race and ethnicity distribution, insurance coverage, baseline controller use, or coding practices. Seasonal drift is not a theoretical concern when the exposure itself changes from routine urban pollution to weeks of smoke.
Regulatory status is similarly narrow. There are AI-enabled respiratory tools near this space, including monitors that detect wheeze, but the cited evidence does not establish an FDA-cleared device specifically for air-quality-based respiratory health alerts. For now, these systems are best viewed as investigational clinical decision support or public-health-adjacent tools, depending on how they are deployed.
Where the Field Stands
AI can already identify asthma and COPD exacerbation risk with accuracy that deserves clinical attention. The strongest signal comes from models that combine environmental context with patient-level clinical data, not from air quality data alone. The unresolved question is whether a health system can turn those predictions into timely, safe, equitable action without creating another stream of poorly owned alerts.
The practical threshold is clear enough: prospective workflow trials, external validation across regions and seasons, monitoring for model and sensor drift, and explicit plans for alert fatigue. Until then, the best reading of the evidence is neither dismissal nor adoption. The prediction problem is increasingly solvable. The clinical accountability problem is still open.
References
- Predicting Asthma Hospital Encounters in Patients With Asthma Using Machine Learning, PubMed, 2018, https://pubmed.ncbi.nlm.nih.gov/30382605/
- Prediction of Clinical Outcomes for Emergency Department Patients With Asthma and Chronic Obstructive Pulmonary Disease Exacerbations: A Machine Learning Approach, PubMed, 2018, https://pubmed.ncbi.nlm.nih.gov/29970272/
- A Machine Learning Approach to Predicting Acute Asthma Exacerbation, PubMed, 2021, https://pubmed.ncbi.nlm.nih.gov/33440184/
- Predicting Asthma Exacerbation With Machine Learning: Retrospective Cohort Study, PubMed, 2021, https://pubmed.ncbi.nlm.nih.gov/33861206/
- Air Pollution and Your Health, National Institute of Environmental Health Sciences, https://www.niehs.nih.gov/health/topics/agents/air-pollution
- Fire and Smoke Map, AirNow, https://fire.airnow.gov
- AirPredict: A Digital Health System for Asthma Self-Management, Frontiers in Digital Health, 2025
- An interpretable machine learning framework for real-time air quality monitoring and health risk prediction, Scientific Reports, 2025, https://www.nature.com/articles/s41598-025-14214-6
Comments
Join the discussion with an anonymous comment.