The most clinically useful evidence for AI in air quality monitoring for health does not begin with a sensor dashboard or an air-quality forecast. It begins in acute coronary syndrome, where risk scores already shape urgency, monitoring intensity, and post-discharge concern, but generally do not ask what a patient has been breathing.
That omission matters because the strongest current clinical comparison comes from a Malaysian ACS registry study that tested whether machine learning could improve mortality prediction by adding air pollution variables to familiar clinical data. Kasim et al. analyzed 14,145 patients with ACS across 25 Malaysian hospitals from 2006 to 2017, using registry variables together with pollutant exposure data including nitrogen oxides and ozone.[1]
The ACS Signal Is Stronger Than a Generic Accuracy Claim
For STEMI, the random forest model reached an AUC of 0.843, compared with 0.791 for TIMI.[1] That difference is not a bedside protocol by itself, but it is large enough to deserve attention from clinicians who use discrimination metrics as one part of model appraisal. A model with an AUC in that range is separating fatal and nonfatal outcomes better than the conventional score in the tested population, and it is doing so with variables that include the patient’s environmental context rather than only the clinical snapshot at presentation.
The NSTEMI comparison is more dramatic and also more delicate. In the same study, the random forest approach outperformed TIMI, while TIMI had an AUC of 0.565 for NSTEMI mortality prediction.[1] It would be too easy to read that as a sweeping defeat of conventional scoring. A more careful reading is that TIMI may be less well suited to this NSTEMI mortality task in this dataset, and the machine learning model may be capturing risk structure that the score was not designed to represent.
The net reclassification result points in the same direction. Kasim et al. reported an NRI improvement of 86.94% for NSTEMI.[1] Reclassification is clinically tempting because it sounds closer to triage than AUC does: patients move into different risk categories. But it still does not answer whether a cardiology team would change treatment, monitoring, transfer decisions, or discharge planning in a way that improves outcomes. It says the model sorted risk differently and, in the study context, more favorably by the chosen metric.
Why NOx and Ozone in the Model Matter
The most interesting part of the ACS study is not just that the random forest performed better. It is that the model’s interpretability analysis did not bury air pollution as a peripheral feature. SHAP analysis identified NOx and O3 among the top four contributors to mortality prediction, alongside Killip class and fasting blood glucose.[1]
That ranking changes the clinical texture of the finding. Killip class is recognizably bedside medicine; fasting glucose is a familiar metabolic signal. Seeing NOx and ozone placed near those variables does not prove causality for an individual patient, and it does not make exposure data equivalent to a physical exam. It does suggest that environmental exposure can behave like a measurable risk feature inside a clinical prediction task, rather than remaining only a population-level concern outside the chart.
This is where AI adds something more specific than another pollution warning. Conventional ACS scores such as TIMI and GRACE were not built to incorporate daily or historical pollutant conditions. A machine learning model can accept those inputs, test whether they improve prediction, and rank their contribution against clinical features. The important word is test. A pollutant should not enter clinical decision support because it is biologically plausible; it should enter because it improves a defined clinical prediction task under validation.
Kasim et al. also described a web-based deployment for continued validation of the ACS-air pollution model.[1] That matters because the right next question is not whether a registry model can be admired in isolation. It is whether performance survives new patients, changed care pathways, different exposure patterns, and clinicians who need the result at the right moment rather than after the interesting computation has already happened.
Exposure Forecasting Is a Supporting Layer, Not the Endpoint
High-quality exposure estimation is still necessary. In the same study cluster, LSTM models predicted PM2.5 across four urban monitoring stations with R² values up to 0.998.[1] Feature optimization reduced the required inputs from 10 variables to 5—PM2.5, PM10, NO2, humidity, and wind speed—while maintaining accuracy.[1] For health systems or public health settings with limited monitoring infrastructure, that kind of reduction could matter operationally.
But PM2.5 forecasting and clinical risk prediction should not be collapsed into the same claim. A model that forecasts particulate levels well is solving an environmental sensing problem. A model that predicts ACS mortality or asthma exacerbation risk is solving a clinical problem. The first can feed the second, but it does not validate the second.
| Model task | What it measures | Clinical boundary |
|---|---|---|
| Air pollutant forecasting | Expected pollutant concentration such as PM2.5 | Useful exposure input, not a patient outcome |
| ACS mortality prediction | Risk of death after acute coronary syndrome | Needs comparison with established scores and outcome validation |
| Asthma frequency prediction | Likelihood or frequency of asthma-related events | Dataset-specific unless externally validated |
| Wheeze detection | Respiratory sound pattern consistent with wheeze | Physiologic signal, not a complete management model |
Respiratory Monitoring Shows the Emerging Pathway
Respiratory applications are developing along a different but related path: forecast the air, detect the physiologic response, and eventually support management decisions. The evidence is not yet as clinically consolidated as the ACS registry comparison, but it helps show how environmental risk could become actionable outside a hospital encounter.
Machine learning studies have reported asthma-frequency prediction from lifestyle, environmental, and dietary data, with SVM and neural network approaches reaching accuracy as high as 93.19% in specific datasets.[2] That figure is encouraging only if the endpoint and setting remain visible. It is not a general estimate of how accurately asthma exacerbations can be predicted across climates, housing types, medication adherence patterns, or health systems.
Other investigational work, including IGDBN-based asthma monitoring, moves closer to continuous surveillance by combining algorithmic classification with changing patient and environmental inputs.[2] The clinical question is whether such systems can identify deterioration early enough to alter inhaler use, trigger clinician review, or prevent emergency care without flooding patients and clinicians with low-value alerts.
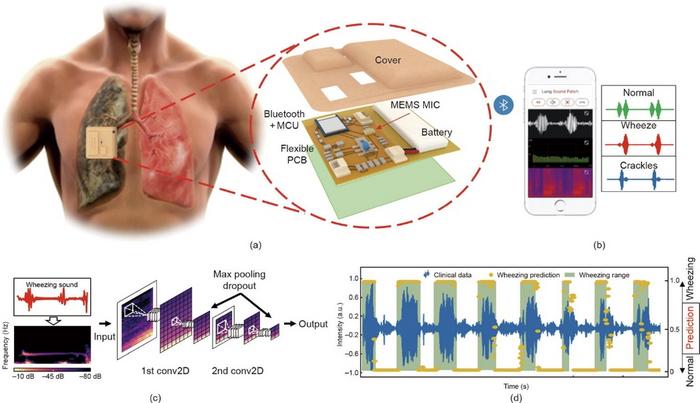
Wearable respiratory sensing begins to connect those alerts to physiology. A wireless lung-sound monitoring patch tested with AI-based breathing-event counting distinguished more than 80% of wheezing events in patients with COPD.[3] That is not the same as predicting a pollution-triggered exacerbation, but it does supply a clinically recognizable signal downstream of exposure: the patient is wheezing, and the system can detect much of that signal without requiring a traditional in-office auscultation.
Connected Asthma Platforms Are Feasible, but Feasibility Is Not Clearance
The AirPredict eHealth feasibility study is useful because it brings the pieces into one asthma-management environment: a Fitbit Charge 6, an Atmotube PRO air-quality monitor, a MIR SmartOne spirometer, and AI analytics. Reported single ease question usability scores ranged from 5.5 to 6.9 on a 7-point scale.[4] That suggests patients can plausibly interact with a connected monitoring stack, at least in a feasibility context.
For clinical deployment, usability is necessary but insufficient. A patient can wear a device, blow into a spirometer, and tolerate an app while the harder questions remain unresolved: which alert matters, who receives it, how quickly it is reviewed, what action is recommended, and whether the intervention improves outcomes rather than increasing surveillance burden.
The regulatory anchor is narrower than the technology story. TytoCare’s Tyto Insights for Wheeze Detection received FDA 510(k) clearance in 2023 for AI-enabled wheeze detection in home respiratory sound analysis.[5] That is important precedent for AI interpretation of respiratory sounds outside the clinic. It is not clearance for an integrated model that combines air pollution exposure, clinical history, wearable physiology, and medication behavior to predict asthma or COPD exacerbations.
What Would Make This Clinically Actionable?
The ACS evidence already justifies serious validation work. A large registry base, comparison with TIMI, pollutant-specific signal, SHAP interpretability, and continued web-based validation make Kasim et al. more than a proof-of-concept exercise.[1] The finding that NOx and ozone rank with established clinical predictors is precisely the kind of result that can change what researchers decide to measure next.
The next layer is less glamorous and more decisive. External validation has to show whether the ACS model performs outside the Malaysian NCVD-ACS setting, across other Western Pacific populations and broader global cohorts. Calibration matters as much as discrimination if clinicians are asked to act on an individual risk estimate. Equity testing is also essential, because environmental exposure is not randomly distributed; a model can reveal exposure-related risk while also importing surveillance gaps from neighborhoods with poorer monitoring coverage.
Workflow testing then determines whether the signal has a place to go. In ACS care, a risk estimate may matter if it changes monitoring level, cardiology review priority, transfer decisions, discharge timing, follow-up intensity, or patient counseling. In asthma care, it may matter if it changes controller therapy review, prompts early contact, or helps distinguish environmental exposure risk from poor symptom perception. A risk score that arrives too late, lacks an owner, or creates no supported action is still only a model output.
Regulatory classification remains a separate boundary. FDA clearance for AI wheeze detection shows that home respiratory AI can enter regulated use, but there is no specific clearance identified here for an integrated air-pollution-plus-clinical-variable risk prediction model as a medical device. Until that changes, claims should stay close to the evidence: improved prediction in defined studies, promising monitoring components, and unresolved deployment requirements.
The Line Between Better Prediction and Routine Use
AI-enhanced environmental monitoring has crossed an important threshold. It is no longer only a plausible public health idea that air quality belongs somewhere near the clinical record. In ACS, machine learning that incorporates NOx and ozone has outperformed a conventional risk score in a large registry analysis and made pollutants visible among top mortality contributors.[1] In respiratory care, asthma prediction models, connected monitoring platforms, wearable lung-sound analysis, and cleared wheeze detection show a pathway from exposure measurement toward physiologic and clinical decision support.[2][3][4][5]
That is evidence of improved prediction, not permission for broad deployment. The remaining work is external validation, calibration, workflow integration, equity assessment, and regulatory clarity. For clinical use, the most defensible conclusion is measured: AI can make environmental exposure clinically legible in cardiorespiratory risk modeling, but health systems still need to prove when that added signal changes care safely and usefully.
References
- Machine learning model incorporating air pollution data to predict mortality in acute coronary syndrome patients. Scientific Reports, 2026. https://www.nature.com/articles/s41598-025-15410-0
- Machine learning models for respiratory outcomes. Source details not specified.
- Wireless wearable stethoscope patch with AI-based breathing-event counter. Source details not specified.
- AirPredict eHealth platform feasibility study. Frontiers in Digital Health, 2025. Source link not specified.
- Tyto Insights for Wheeze Detection, 510(k) K221614. U.S. Food and Drug Administration, 2023. Source link not specified.
Comments
Join the discussion with an anonymous comment.