For COPD care, the useful question is not whether AI can forecast tomorrow’s air quality. It is whether those forecasts add anything to a patient’s chart that changes short-term clinical risk detection. In the strongest available clinical evidence, adding AI-derived forecasts for PM2.5, NO2, O3, and PM10 to EHR-based models improved 7-day COPD exacerbation prediction only when the model architecture could use nonlinear pollutant-health interactions. In Ratcliff et al.’s AMIA 2023 study of 6,635 patients and 255,987 encounters in middle Tennessee, a random forest model using clinical plus multi-pollutant inputs reached an AUC of 0.86, compared with 0.83 for a clinical-only random forest model; logistic regression did not show improvement from adding the air quality forecasts.[1]
That distinction matters. A COPD exacerbation often looks foreseeable after it happens: prior exacerbations, comorbidities, medication patterns, season, and neighborhood exposure all seem to have been pointing somewhere. At the visit or outreach decision, however, clinicians do not get to inspect the future with hindsight. They get a risk score, a threshold, a queue, and limited capacity to act.
The Clinical Signal Is Modest, but It Is Real Enough to Examine
Ratcliff et al. did not test air quality forecasting as a public-health map or an environmental dashboard. They tested whether forecasted pollutant exposure could improve prediction of a clinical endpoint: COPD exacerbation within 7 days. The study linked EHR data to AI-derived forecasts for four pollutants and compared clinical-only models with clinical-plus-pollutant models across modeling approaches.[1]
| Model comparison | Result in Ratcliff et al. | Clinical interpretation |
|---|---|---|
| Clinical-only random forest | AUC 0.83 | The chart already carried substantial predictive information. |
| Clinical + multi-pollutant random forest | AUC 0.86 | Forecasted pollutant data added signal when the model could capture nonlinear interactions. |
| Logistic regression with added air quality forecasts | No improvement | Simply adding pollutant variables was not enough. |
The AUC increase from 0.83 to 0.86 is meaningful, but it is still a model performance metric. The more clinically legible result is the net benefit analysis. At a 10% risk threshold, the clinical-plus-pollutant random forest identified 35 exacerbations per 10,000 encounters, compared with 26 per 10,000 for the clinical-only random forest.[1] That is not a dramatic population-wide transformation. It is a small gain in a high-volume setting where missed early deterioration can become an ED visit, hospitalization, or delayed treatment opportunity.
The 10% threshold also deserves attention because it is closer to the way a health system would use such a model. AUC summarizes ranking across thresholds. A threshold decides who enters a work queue, who gets a call, who receives medication review, who is asked about symptoms, and who is left alone. If a model improves discrimination but offers no useful gain at a plausible action threshold, the improvement may remain academically tidy and operationally irrelevant.
Why the Logistic Regression Result Should Not Be Treated as a Footnote
The negative logistic regression finding is one of the most important parts of the study. It narrows the claim. The evidence does not say that any EHR model becomes better once a health system attaches air quality variables. It says improvement appeared with a random forest model and did not appear with logistic regression.[1]
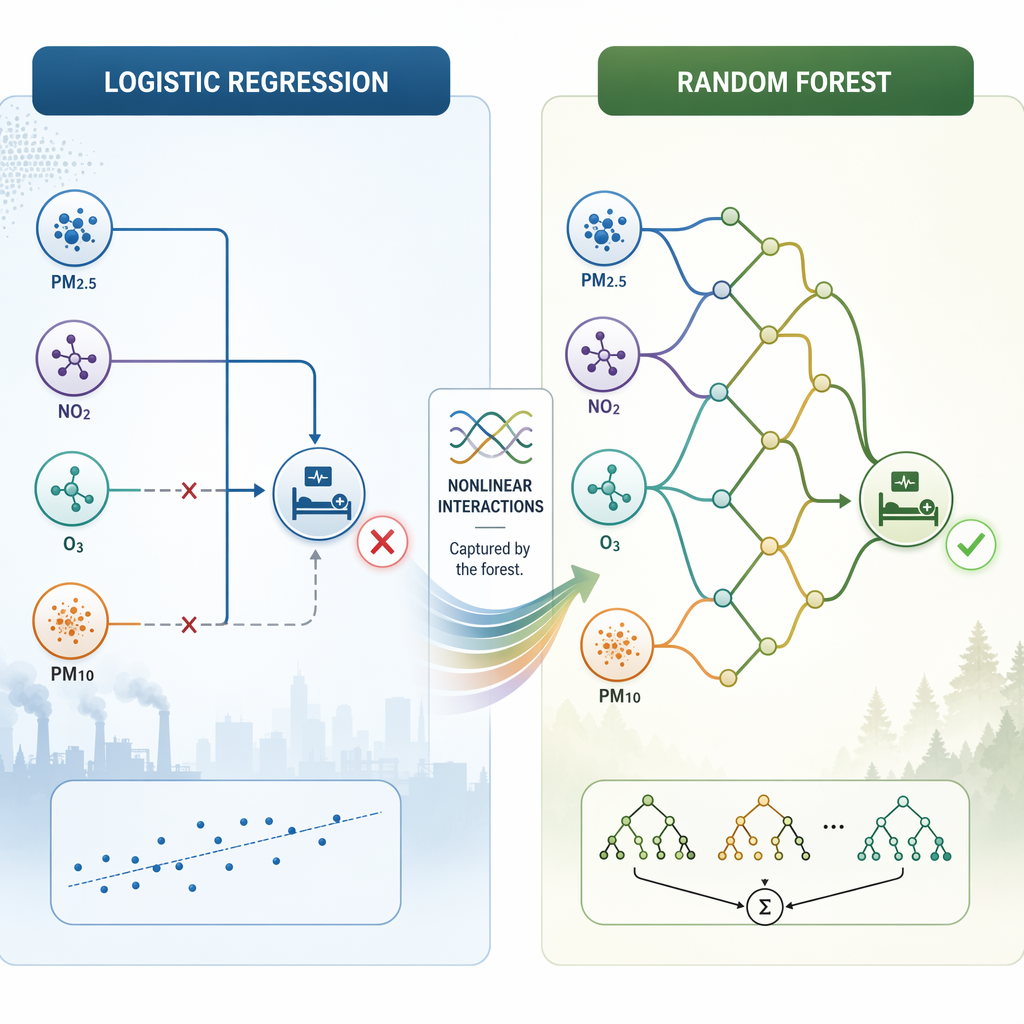
That pattern fits the clinical problem. Multi-pollutant exposure is not just four independent numbers waiting to be added to a chart. PM2.5, NO2, ozone, and PM10 may matter differently by season, comorbidity, baseline risk, medication use, prior exacerbation history, and the local mix of sources. A linear model can be made more flexible, but a basic logistic regression is not built to discover many higher-order interactions without those interactions being specified in advance.
This is where AI-based air quality forecasting becomes clinically specific rather than atmospheric in the abstract. The useful object is not the forecast alone. It is the forecast inside a prediction architecture that can expose patterns clinicians are unlikely to calculate mentally and that a simpler model may flatten out.
The practical implication is uncomfortable but necessary: a site that cannot support machine learning infrastructure, validation, monitoring, and governance should not assume it can obtain the same benefit by dropping forecasted pollutant values into an existing regression-based risk score. The architecture is part of the intervention.
The Equity Signal Is the Part That Should Slow Deployment Conversations Down
The subgroup result is sharper than the average effect. At the same 10% risk threshold, adding multi-pollutant forecasts produced 21 additional correct exacerbation identifications per 10,000 encounters for Black patients, compared with 7 additional correct identifications per 10,000 encounters for white patients.[1] The ratio is hard to ignore: the additional benefit was three times higher for Black patients in this dataset.
That does not prove the model reduces racial disparities after deployment. Prediction is not treatment. A correct additional identification only becomes a better outcome if someone acts, the action is appropriate, the patient can access care, and the intervention arrives early enough to matter. A model can also create new inequities if outreach capacity is uneven, if thresholds are poorly chosen, or if alerts are ignored in clinics already carrying higher burdens.
Still, the finding is clinically plausible enough to take seriously. Environmental exposure is not evenly distributed, and EHR-only models may miss part of the short-term risk structure for patients whose respiratory status is more tightly coupled to outdoor pollutant patterns. In that setting, pollutant forecasts may not be decorative context. They may be one of the few external signals that helps a risk model see something the chart alone underweights.
The responsible reading is bounded: Ratcliff et al. show a larger prediction gain for Black patients in a middle Tennessee dataset, not confirmed outcome improvement and not proof that the same subgroup pattern will appear in every region.[1] That is enough to justify prospective validation designed with equity endpoints in mind. It is not enough to market the model as a disparity-reduction intervention.
Air Quality AI Is Technically Active, but Clinical Endpoint Validation Is Scarcer
The broader air quality forecasting literature shows that machine learning can perform well on environmental prediction tasks. Jalali et al. reported Random Forest AQI classification accuracy of 99.96% and a TSMixer concentration forecasting R² of 0.9861 using data from Kabul and Istanbul.[2] Those figures are impressive, but they remain environmental task metrics. They do not show that COPD exacerbations, asthma visits, medication needs, or hospitalizations are better predicted.
Madan et al. reported a hybrid CNN-LSTM model achieving about 91% F1 for AQI forecasting in Gurugram, India, but the study was limited to a single city and a 4-month data window.[3] Again, the result supports technical plausibility. It does not establish clinical transportability.
Operationally, AI air quality forecasting is no longer hypothetical. The NASA-State Department ZephAir program has applied AI forecasting across more than 260 global locations, showing that environmental data pipelines can be built and maintained beyond a single research lab.[4] For clinical decision support, however, the hard part begins after the forecast exists: linking exposure to individual patients, validating against health endpoints, choosing action thresholds, and monitoring performance as both air pollution and clinical practice change.
What a Health System Would Need Before Treating This as Decision Support
The Ratcliff et al. study used middle Tennessee data from 2014 through 2020 and linked patients to the nearest outdoor EPA monitors.[1] That design is reasonable for retrospective modeling, but it leaves several deployment questions unresolved. A patient’s nearest outdoor monitor is not the same as personal exposure. Indoor air, housing conditions, occupational exposure, commuting, time spent away from home, and monitor distance can all weaken the connection between forecasted outdoor pollution and the air a patient actually breathes.
Generalizability is also not automatic. Pollutant composition differs by region. A model trained where traffic emissions, industrial sources, weather patterns, and seasonal allergens combine in one way may not behave the same in a region with a different mixture. Local validation should not be treated as a regulatory formality; it is where the health system learns whether the environmental signal survives contact with its own patients.
- Model architecture: the clinical benefit in the core study appeared with random forest modeling, not logistic regression.
- Exposure linkage: nearest outdoor monitor data may miss indoor, commuting, workplace, and time-activity exposure.
- Local validation: pollutant mixtures and baseline COPD risk may differ substantially outside middle Tennessee.
- Threshold selection: the reported net benefit depends on a 10% risk threshold, and other action thresholds may change the balance.
- Drift monitoring: environmental patterns, coding behavior, treatment patterns, and patient populations can shift after deployment.
There is also a workflow question that model papers rarely settle. If the risk score rises because of tomorrow’s pollutant mix, what is the expected action? A nurse call? Rescue medication review? Same-day telehealth? Advice to reduce exposure? A reminder to check oxygen saturation? Different actions tolerate different false-positive rates. A low-cost automated message may justify a lower threshold than a clinician-staffed outreach queue.
This is where broader clinical AI governance matters. Teams already thinking about AI in medicine evidence, transfer across settings, and clinical AI model drift monitoring will be better positioned than teams treating environmental forecasts as a plug-in data feed. The model needs the same scrutiny as any other clinical prediction tool, with the added burden that the external environment is changing continuously.
A Bounded Clinical Conclusion
AI-derived multi-pollutant forecasts can improve 7-day COPD exacerbation detection when paired with machine learning models capable of capturing nonlinear interactions. The best current clinical evidence shows a random forest improvement over EHR-only prediction, a net benefit gain at a 10% risk threshold, and a larger added benefit for Black patients than white patients.[1]
The same evidence also sets the limits. Logistic regression did not improve. The main study is regional. Exposure linkage is imperfect. The equity signal is a prediction result, not an outcomes result. High AQI forecasting accuracy in other studies supports feasibility of environmental modeling, but it does not substitute for endpoint validation in respiratory care.[2][3][4]
The next step is not broad clinical adoption as if the intervention were already proven. It is careful external validation, subgroup analysis, threshold testing, and workflow design in settings prepared to monitor the model after it starts influencing care.
References
- Impact of Incorporating Air Quality Data into COPD Exacerbation Prediction Models, AMIA Annual Symposium Proceedings, 2023, https://pmc.ncbi.nlm.nih.gov/articles/PMC10785856/
- Artificial intelligence-based air quality forecasting using machine learning and deep learning models, Discover Atmosphere, 2025, https://link.springer.com/article/10.1007/s44292-025-00052-8
- Hybrid CNN-LSTM model for air quality index forecasting, Scientific Reports, 2026, https://www.nature.com/articles/s41598-026-36564-5
- AI Air Quality Forecasting: A State-NASA Partnership, Foreign Service Journal, 2024, https://afsa.org/ai-air-quality-forecasting-state-nasa-partnership
Comments
Join the discussion with an anonymous comment.