The interesting moment in artificial intelligence and medical diagnosis is no longer the conference slide where a model matches, or beats, a benchmark. It is the quieter moment in a stroke pathway when the label has already arrived.
A patient has been scanned. Before the full diagnostic reasoning has unfolded across the emergency department, radiology, stroke team, and transfer network, an AI system has flagged a stroke-related finding. The label is now visible to clinicians who still have to decide whether it is right, whether it matters for this patient, and whether it should change the next call, image review, or treatment decision.
That is a different diagnostic order. In the older sequence, clinicians moved from symptoms and images toward a conclusion. In some deployed hyperacute stroke settings, the conclusion appears early, and the team works backward through verification. A five-year qualitative study of AI use across three UK stroke hubs described this shift in practice: AI-generated labels did not simply add another data point; they changed the sequence of work around diagnosis, coordination, and review.[1]

The label now arrives before the reasoning is finished
Stroke services have always been built around time pressure. The work is not only to recognize a stroke, but to move the right patient through imaging, specialist review, transfer decisions, and treatment windows without losing the thread. A scan result may be clinically obvious, borderline, or misleading. A transfer call may depend on whether a receiving team trusts the sending team’s interpretation. A treatment decision may wait on a neuroradiology read, a vascular image, or a senior clinician who is covering more than one urgent problem.
The UK stroke study matters because it watches that chain rather than treating diagnosis as a private mental event. The researchers followed AI deployment over five years across three stroke hubs and documented how AI labels entered the pathway early enough to reorganize subsequent work.[1] The useful word is not replacement. It is inversion.
Once the label appears, the clinical task changes shape. The team is no longer only asking, “What do the symptoms and images suggest?” It is also asking, “Why has the system called this, and can we confirm or reject it quickly enough to act?” That second question is not a trivial check. It creates a new layer of diagnostic labor: reopening images, comparing the AI output with clinical signs, deciding whether the label fits the patient in front of the team, and communicating the degree of confidence to colleagues who may be off-site.
This is where simple claims about speed can become sloppy. If the label reduces the time to a vascular review, gets the right specialist looking sooner, or makes a transfer conversation more concrete, that is a real process gain. If it merely moves uncertainty earlier and leaves the next clinician to absorb the risk, the saved minutes have landed in a different place.
Verification becomes part of the diagnostic workflow, not an afterthought
The stroke study’s strongest contribution is its description of verification as work. AI did not simply produce an answer that clinicians accepted or ignored. It inserted a signal into a time-sensitive clinical system, and that signal had to be handled by people with different roles, pressures, and levels of expertise.[1]
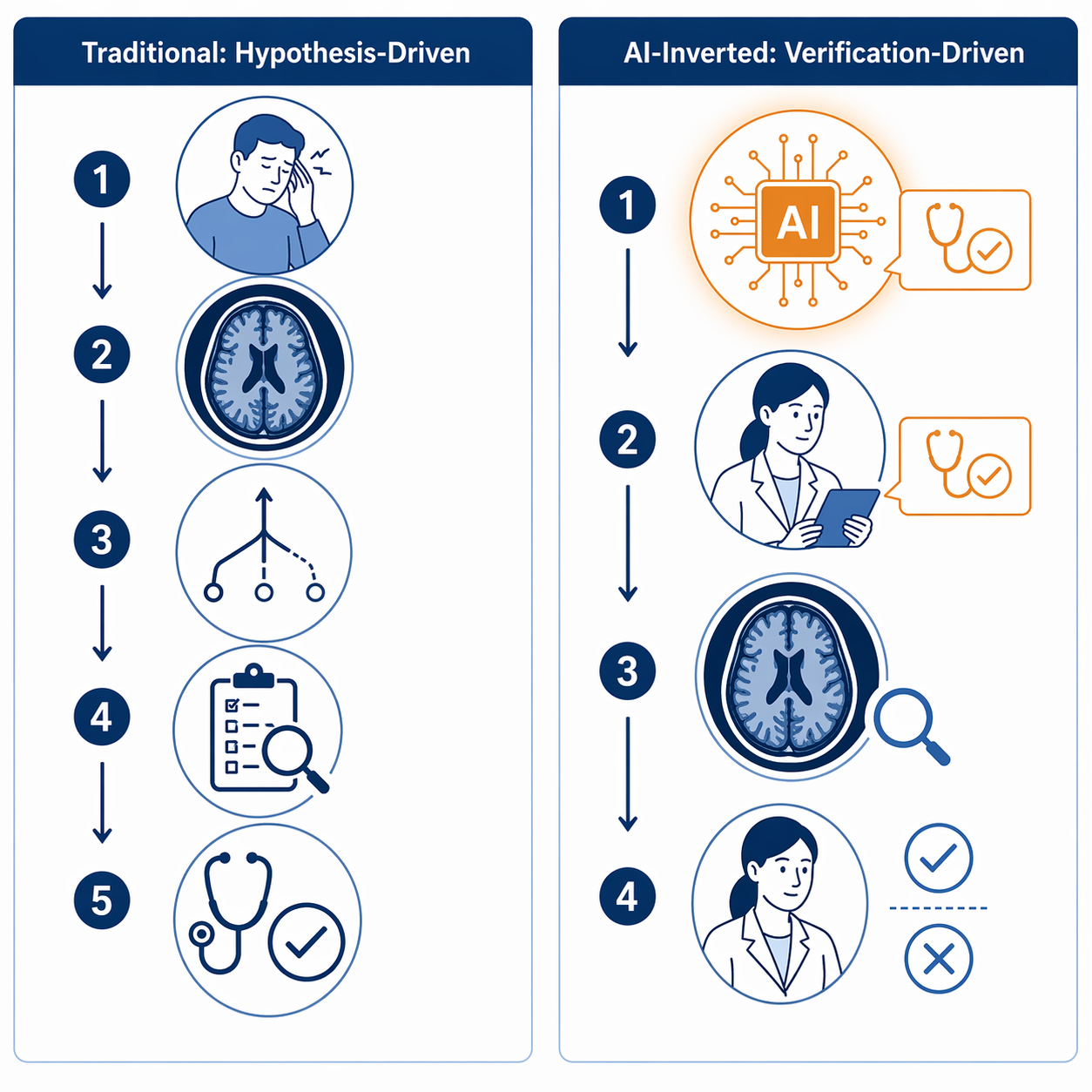
| Traditional pathway | AI-inverted pathway |
|---|---|
| Symptoms, examination, and imaging are assembled before the diagnostic label stabilizes. | An AI-generated label may appear early, before all human reasoning and consultation have finished. |
| Clinicians form and refine hypotheses through sequential review. | Clinicians verify, qualify, or reject a machine-generated label while continuing clinical assessment. |
| Communication often follows a human interpretation of the scan. | Communication may begin around the AI flag, with humans checking whether the flag deserves action. |
| The diagnostic conclusion is the output of the pathway. | The diagnostic label becomes an input into the pathway. |
That inversion can help. In hyperacute stroke, early image interpretation is not an academic exercise; it is tied to thrombolysis, thrombectomy assessment, transfer, and specialist availability. A system that pushes a possible large-vessel occlusion or hemorrhage to the front of attention can shorten the interval before a human with the right authority reopens the images. The study documents this as a change in process, not as definitive proof that every downstream patient outcome improved.[1]
That distinction is not pedantry. Process evidence can be strong while outcome evidence remains incomplete. A pathway may become faster at identifying likely candidates for specialist review, yet still need separate evidence showing improved morbidity, mortality, treatment rates, or functional outcomes. The stroke evidence gives a vivid account of changing clinical practice; it does not close every question about final patient benefit.[1]
The new work is distributed unevenly
The person who receives the alert may not be the person who signs the final report. The clinician who sees the flag may be in an emergency department, a stroke unit, a radiology workflow, or a transfer network. The label may accelerate escalation, but it also creates a responsibility to decide whether escalation is justified.
In practice, verification is likely to include several small acts that rarely appear in model-performance tables: checking the scan slice by slice, asking whether the clinical presentation fits the image label, calling a colleague earlier than usual, documenting why a flag was overruled, or deciding that an equivocal label should not trigger a transfer. These are not ceremonial human-in-the-loop gestures. They are where safety is either preserved or eroded.
A good implementation therefore changes more than software. It changes who is notified, what the alert contains, how disagreement is recorded, when senior review is required, and whether false positives and false negatives are reviewed as service events rather than treated as isolated annoyances.
Regulatory scale does not answer the workflow question
Stroke is not an isolated curiosity. AI medical devices are now part of a much larger diagnostic-imaging and triage environment. Innolitics’ 2025 year-in-review reported more than 1,300 FDA-cleared AI/ML medical devices, with many operating in areas such as imaging, detection, prioritization, and triage.[2] That scale makes workflow inversion a practical issue for clinical leaders, not a niche informatics debate.
But clearance and deployment do not settle the clinical question. A cleared tool may perform a defined function acceptably for its intended use, while the service still has to decide how its output enters clinical work. Does the label go to radiology only, or also to the stroke coordinator? Does it interrupt a clinician, sit in a worklist, or trigger a transfer conversation? Who can override it? Who audits disagreement?
These questions become more important as similar patterns appear in adjacent areas such as lung nodule triage, pneumothorax detection, sepsis warning, and acute myocardial infarction workflows. The stroke study should not be stretched into proof that every specialty is undergoing the same transformation. It is better read as a detailed warning that when AI enters early enough, diagnostic practice may change before outcome research has caught up.
The AI chasm opens between model performance and clinical benefit
The broader diagnostic-accuracy literature helps explain why the stroke evidence should be handled carefully. Stanford HAI has described the gap between promising AI performance in controlled diagnostic settings and the harder question of whether those systems improve real-world clinical decision-making and patient outcomes.[3] That gap is sometimes discussed as an “AI chasm”: the space between a model that performs well under evaluation and a tool that reliably improves care inside messy clinical systems.

The chasm is not only technical. A model can be accurate enough to be useful and still fail to improve care if alerts arrive too late, go to the wrong person, produce too many interruptions, or are trusted in the wrong cases. Conversely, a tool with imperfect performance may still improve a pathway if it reliably brings urgent cases to expert attention earlier and the surrounding team is disciplined about verification.
This is why the most serious evaluation of AI diagnosis has to include both model behavior and work behavior. Sensitivity, specificity, and area under the curve remain important, but they are not enough. A service also needs to know whether clinicians reopen the scan, whether alerts shorten time to specialist review, whether overrides are examined, whether the tool changes transfer volume, and whether the final patient outcomes justify the change.
There is a useful connection here to the broader translational problem in AI healthcare research: promising systems often struggle when moved from controlled development into clinical deployment. The same concern sits underneath workflow inversion. A diagnostic label that works well in retrospective evaluation still has to survive the live pathway, with its handoffs, staffing gaps, competing alerts, and incomplete information. See also why most AI healthcare research never reaches clinical practice.
The early label can narrow attention
The discomfort begins with a familiar human tendency: once a label is visible, it becomes hard to unsee. In a stroke pathway, that can be useful when the label pulls attention toward a real emergency. It can be dangerous when the label is wrong, incomplete, or too confidently displayed.
Automation bias is not unique to medicine, but medicine gives it unusually high stakes. A less-experienced clinician may be more likely to treat the AI output as a starting anchor, particularly when the label appears during a crowded shift and seems to come from a validated system. A senior clinician may be more comfortable challenging the label, but senior review is exactly the scarce resource that many AI triage systems are designed to ration more efficiently.
The research base does not yet provide a clean prevalence estimate for automation bias across clinician groups in AI-assisted stroke diagnosis. The risk is better described as a plausible and observed concern in human-AI clinical work, not as a quantified inevitability. That narrower statement is still serious enough. If a diagnostic pathway is becoming verification-driven, then the quality of verification becomes a central safety property.
Bias can hide inside apparently useful shortcuts
Verification also has to defend against errors that are systematic rather than random. MIT researchers reported in 2024 that AI models analyzing medical images can learn demographic shortcuts, using features associated with attributes such as race, sex, or age in ways that contribute to biased diagnostic performance.[4] For a clinician receiving an early label, the practical implication is blunt: the label may be wrong in patterned ways that are not obvious from a single case.
That does not mean every AI stroke alert is demographically biased, and it does not mean bias can be detected by bedside skepticism alone. It means local governance has to look beyond case-by-case impressions. A hospital cannot rely on clinicians to notice a fairness problem one alert at a time, especially when urgent workflows reward rapid acceptance of plausible outputs.
Fairness concerns in medical AI are increasingly discussed alongside automation bias and accountability because biased outputs can be amplified when users over-rely on system recommendations.[5] In a label-first pathway, the order of presentation matters. The AI output does not wait politely at the end of reasoning; it may shape what the clinician looks for next.
Expertise can erode quietly
There is another risk that is harder to measure than a missed alert: the slow erosion of diagnostic confidence. If trainees and early-career clinicians repeatedly encounter the AI label before they have worked through the image themselves, they may get fewer chances to practice forming the first hypothesis. They may still learn to verify. They may not learn, as deeply, to originate.
This is not an argument for hiding useful AI outputs during an emergency. In hyperacute stroke, delay has consequences. But education and service design should not pretend that the sequence is neutral. A pathway that always shows the answer key first teaches a different skill from one that requires independent image review before revealing the machine’s view.
Some services may decide that the tradeoff is worth it in defined urgent contexts. Others may build role-specific displays, delayed reveal for training cases, mandatory independent reads for certain staff groups, or structured disagreement review. The right design depends on staffing, case mix, risk tolerance, and evidence of benefit. What should not survive is the assumption that an early label is educationally harmless because a human remains “in the loop.”
What a safer label-first pathway has to prove
The practical test for AI diagnosis is not whether clinicians like the technology, or whether a model once performed well in a dataset. A safer label-first pathway has to show that the label improves the work around the patient without weakening independent judgment.
- Who receives the alert, and whether that person can act on it.
- How quickly the alert leads to expert image review, not merely notification.
- How clinicians document agreement, uncertainty, and override decisions.
- Whether false positives, false negatives, and near misses are reviewed as workflow events.
- Whether performance is monitored across patient groups, sites, shifts, and clinician experience levels.
- Whether faster coordination translates into better treatment and patient outcomes.
Those measures are less glamorous than model accuracy. They are also closer to where patients are helped or harmed. In stroke care, the critical question is not only whether the system can identify an abnormal image. It is whether the alert changes the right human actions at the right time, while leaving enough room for clinicians to distrust it when distrust is warranted.
The UK stroke evidence shows that AI is already changing the order of diagnostic work in hyperacute care.[1] That change matters even before definitive outcome data arrives, because workflow is not a neutral container for diagnosis. It is part of diagnosis. If medicine is becoming label-first in some pathways, the safety question is no longer only whether the model is accurate in a study. It is whether the surrounding clinical system preserves independent judgment, detects systematic error, and proves that faster diagnosis becomes better care.
References
- Transforming diagnosis through artificial intelligence. npj Digital Medicine, 2025.
- 2025 Year in Review: AI/ML Medical Device 510(k) Clearances. Innolitics, 2025.
- Can AI Improve Medical Diagnostic Accuracy?. Stanford HAI.
- Study reveals why AI models that analyze medical images can be biased. MIT News, 2024.
- Bias in Medical AI: Algorithmic Fairness and Ethics Challenges. Journal of Young Investigators, 2026.
Comments
Join the discussion with an anonymous comment.