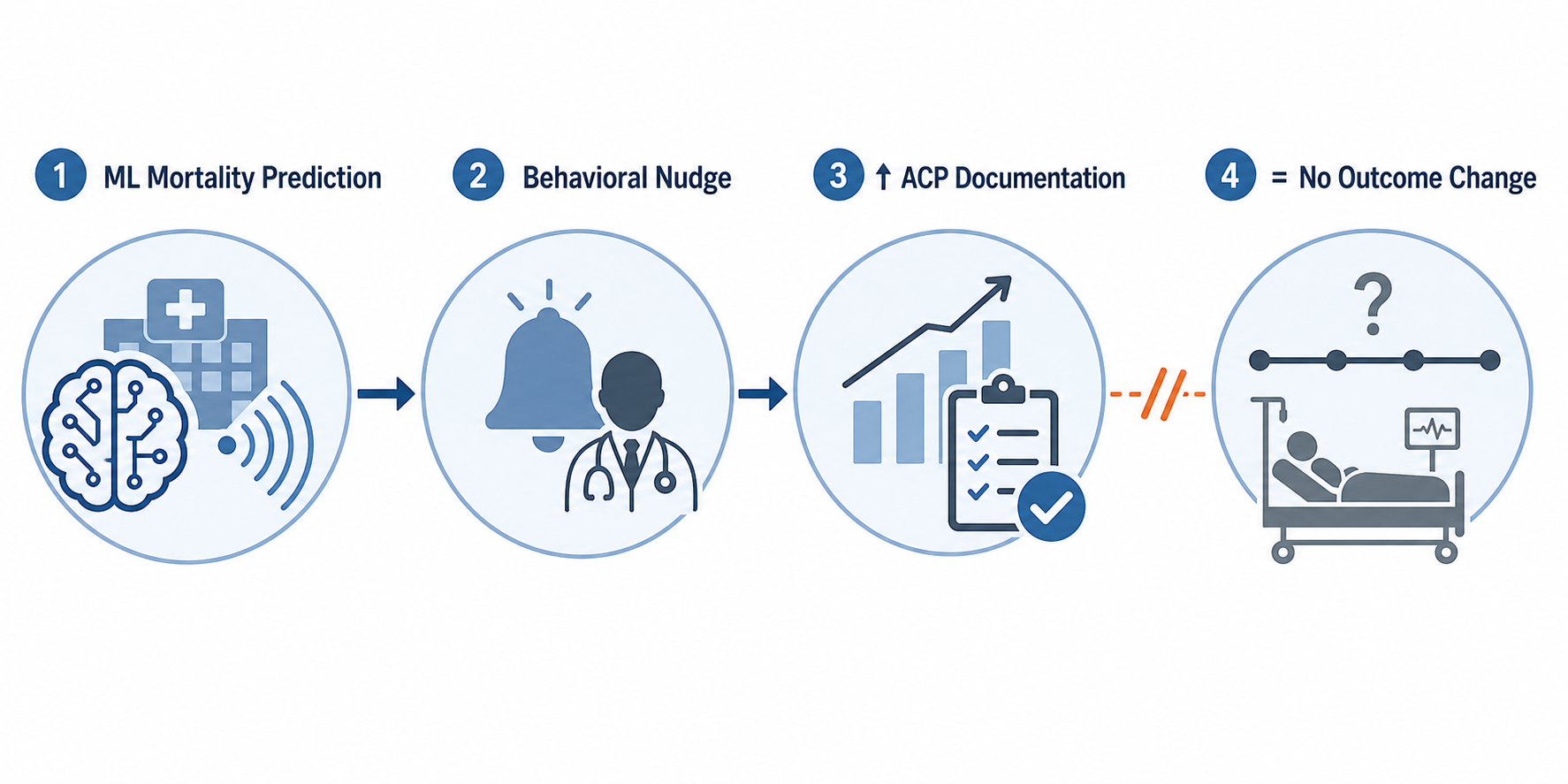
AI in end of life care planning has produced one of the more uncomfortable results in clinical informatics: the workflow intervention works, and that is not the same as the care working. Machine learning mortality estimates can identify patients whom oncology teams are likely to miss, and behavioral nudges can move clinicians to document serious illness conversations. In the strongest randomized evidence, that immediate target changed substantially. What has not yet changed, at least in the studies available so far, is the downstream pattern of end-of-life care.
The stepped-wedge randomized clinical trial by Manz and colleagues is the load-bearing study here because it tested a health system intervention rather than a model in isolation. The intervention combined machine learning mortality estimates with behavioral nudges to clinicians. Serious illness conversation rates rose from 1.3% to 4.6% overall, and among high-risk patients from 3.6% to 15.2%.[1] That is not a trivial documentation bump. In a setting where these conversations often do not happen before a crisis admission, moving the rate at all matters.

The Duke quality improvement experience made the documentation signal even harder to ignore. In high-risk cancer patients identified by a machine learning model, clinician notifications through the Epic EHR were associated with an increase in advance care planning documentation from 2.3% to 81%.[2] A result that large deserves attention. It also deserves restraint. Documentation can be an essential first step, but it is still a step inside a larger clinical chain.
What the intervention actually changes
The mechanism is straightforward enough to be attractive to health systems. A mortality prediction model scans available clinical data and identifies patients whose near-term risk is high enough to justify prompting a clinician. The nudge then appears inside a workflow the clinician already uses: a reminder, a notification, performance feedback, peer comparison, or an opt-out prompt. The intended behavior is not a medication order or a procedure. It is a conversation, or at least documentation that a conversation about goals, preferences, prognosis, and future care has occurred.
That design fits a real operational problem. Clinicians are busy, prognostication is uneven, and serious illness conversations are easy to defer until the patient is already in the hospital, decompensating, or surrounded by family members trying to make decisions under pressure. A model that quietly surfaces risk can make the invisible queue visible. A nudge can turn that risk estimate into a task someone is expected to address.
The technical performance is not the center of the story, but it is not irrelevant. Across the studies summarized in the AAHPM PC-FACS review, machine learning models showed AUC-ROC values in the 0.86 to 0.95 range.[2] Those numbers suggest strong discrimination in the studied settings. They do not prove that the right clinician will act, that the right family member will be present, that the note will be visible during the next admission, or that the plan will survive the next clinical turn.
| Intervention layer | What improves | What remains uncertain |
|---|---|---|
| Mortality prediction | Identifies patients at elevated near-term risk | Whether the model generalizes across populations and health systems |
| Behavioral nudge | Moves clinicians toward serious illness conversations or ACP documentation | Whether the prompt creates a high-quality conversation rather than a completed task |
| EHR documentation | Creates a retrievable record of preferences or discussion | Whether that record changes orders, handoffs, escalation decisions, or family understanding |
The outcome gap is not a footnote
The difficult part is that the same body of evidence that supports the intervention’s effect on documentation does not support a claim that it improves end-of-life outcomes. The AAHPM PC-FACS synthesis of the Manz, Patel, and Piscitello studies notes no significant downstream effects on outcomes such as length of stay, hospice referral rates, code status changes, ICU admissions, 30-day readmissions, or mortality.[2] For patients and families, those are not secondary abstractions. They are often where the consequences of planning, or the absence of planning, become visible.
The PC-FACS commentary states the interpretive problem plainly: “holding and documenting ACP discussions may be insufficient to impact downstream outcomes and ensure goal-concordant end-of-life care.”[2] That sentence should sit near any institutional slide showing a documentation spike. It does not negate the value of the spike. It prevents the spike from being mistaken for proof that care became aligned with the patient’s goals.
This is where clinical workflow matters more than model elegance. A serious illness conversation note may say that a patient values time at home, fears prolonged dependence on machines, or wants a trial of treatment only if recovery is plausible. But the next hospitalization may be handled by a different team. The note may be buried. The family may remember the conversation differently. The patient’s condition may have changed. A consultant may recommend escalation without seeing the documentation. A night team may treat full code status as the only actionable signal. None of those failures would be solved by making the original prediction more accurate.
Piscitello and colleagues add to the same pattern rather than resolving it. Their retrospective analysis examined a nudge tied to a 90-day mortality prediction threshold of 30%.[2] That design again reflects a plausible operational use of AI: find patients at risk, prompt clinicians, and hope that earlier planning changes later care. The current evidence supports the first two steps more strongly than the third.
Why documentation may stop short of care alignment
Advance care planning documentation is often treated as a discrete event because EHRs are good at counting events. A note exists or it does not. A smart phrase was completed or it was not. A billing or quality field can be queried. Goal-concordant care is harder to count because it depends on whether the documented preference was understood, updated, accessible, and translated into decisions when the patient became sicker.
Several links can fail between the nudge and the bedside outcome. The clinician may open the prompt but have too little time for a meaningful conversation. The conversation may focus on forms instead of prognosis and tradeoffs. The patient may express goals that require follow-up by oncology, palliative care, social work, or home services, but no pathway assigns responsibility for that follow-up. The documented preference may not trigger hospice education, medication changes, treatment de-escalation, caregiver preparation, or a revised escalation plan.
There is also a timing problem. A mortality model can identify risk at a point in time, but preferences are not static. Patients revise what they want as symptoms, treatment options, family capacity, and prognosis change. The scoping review on AI approaches to ACP notes a particularly important gap: no study addressed AI’s role in supporting ongoing review and updating of ACP information.[3] A system that prompts one note and then treats the planning work as complete is misaligned with the clinical reality of serious illness.
This distinction is not academic. If an oncology clinic documents a patient’s preference to avoid prolonged ICU care but does not create a visible escalation plan, the hospital medicine team may still admit to the ICU during the next acute event. If a patient says they want to be home if time is short, but no one discusses hospice eligibility or caregiver support, the documented preference may not become a feasible plan. The problem is not that the ACP note is meaningless. The problem is that the note has to be connected to decisions, services, and accountability.
The implementation risks arrive before outcome benefit is proven
Health systems considering these tools should not wait for perfect evidence before improving serious illness communication. But they also should not deploy mortality prediction as if the only unresolved question is adoption. Transparency remains uneven. In a 2025 scoping review of 41 AI studies in advance care planning, 78% did not disclose source code, and 41.5% gave no data availability information.[3] Those gaps make it harder for clinicians, patients, and health systems to understand whether a model can be evaluated, reproduced, audited, or safely adapted outside its original context.
The same review raises another practical concern: ACP is culturally, linguistically, and socially situated.[3] A mortality estimate may be numerical, but the conversation it triggers is not. If a tool prompts the same action without regard to language access, health literacy, disability, mistrust, family structure, or prior experiences with the health system, it may increase documentation while leaving the most vulnerable patients with the least meaningful planning.
Clinician trust also depends on how mortality data might be used beyond the immediate care team. In Hamer and colleagues’ qualitative work, palliative care clinicians expressed concern that mortality data could be used by insurers to deny coverage.[4] That fear is not a small ethics add-on. If patients or clinicians believe a prediction may become a rationing tool, the conversation around prognosis and preferences becomes contaminated before it begins.
Bias needs the same operational seriousness. A model trained in one population may perform differently in another. A nudge may be acted on differently depending on the clinician, clinic resources, patient language, diagnosis, insurance status, or access to palliative care. If a system monitors only aggregate documentation rates, it may miss whether certain patients receive more prompts, better conversations, faster referrals, or more constrained choices.
A more honest deployment standard
The right conclusion is not that AI has no place in end-of-life care planning. The evidence says something more specific: machine learning mortality prediction plus behavioral nudges can increase serious illness conversations and ACP documentation. That is a clinically useful capability, especially in busy oncology and hospital medicine environments where high-risk patients can pass through multiple encounters without anyone clearly owning the planning conversation.
The deployment standard should therefore be built around what must happen after the prompt. A health system using these tools should be able to answer several operational questions before celebrating success:
- Who is responsible for responding to the nudge, and what time or staffing support makes a real conversation possible?
- Where is the documented preference displayed during emergency, inpatient, ICU, and oncology decision-making?
- Which documented goals trigger downstream actions such as palliative care referral, hospice education, home support planning, or code status review?
- How are ACP notes revisited when prognosis, symptoms, treatment options, or family circumstances change?
- How will the system monitor bias, language access, cultural sensitivity, and possible coercive or payer-driven uses of mortality prediction?
Those questions move the intervention from documentation capture toward care pathway redesign. They also make clear why an unchanged length of stay, hospice referral rate, ICU admission rate, readmission rate, code status pattern, or mortality outcome should not be waved away as a disappointing but distant endpoint. These are the places where a documented plan either enters care or does not.
For now, AI-guided nudges should be presented as evidence-supported tools for increasing ACP documentation and serious illness conversation rates, not as proven tools for improving end-of-life outcomes. The more responsible promise is narrower and more useful: these systems can help clinicians find patients who need planning conversations earlier, but the health system still has to make those conversations visible, revisable, protected, and actionable when decisions are made.
References
- Effect of Integrating Machine Learning Mortality Estimates With Behavioral Nudges to Clinicians on Serious Illness Conversations. JAMA Oncology. 2020.
- AI for Advance Care Planning. AAHPM PC-FACS.
- Artificial intelligence approaches for advance care planning: a scoping review. PMC. 2025.
- Study: AI Can Aid in End-of-Life Care Decisions, But Can't Replace Human Teams. UMD Today. 2025.
Comments
Join the discussion with an anonymous comment.