The first question for AI in mental health legal cases is not whether a model can find a pattern a clinician might miss. Some can. The first question is what happens when that pattern is translated into a legal opinion about dangerousness, malingering, competency, sentencing, treatment placement, or civil commitment.
That distinction matters because forensic mental health already lives in a narrow passage between clinical probability and legal consequence. A violence risk estimate that helps a team decide who needs closer observation is one thing. The same estimate, offered as if it were independent expert evidence, is another. In court, the score does not remain a score. It becomes a reason someone may lose liberty, receive a harsher sentence, be committed preventively, or be placed under more restrictive treatment conditions.

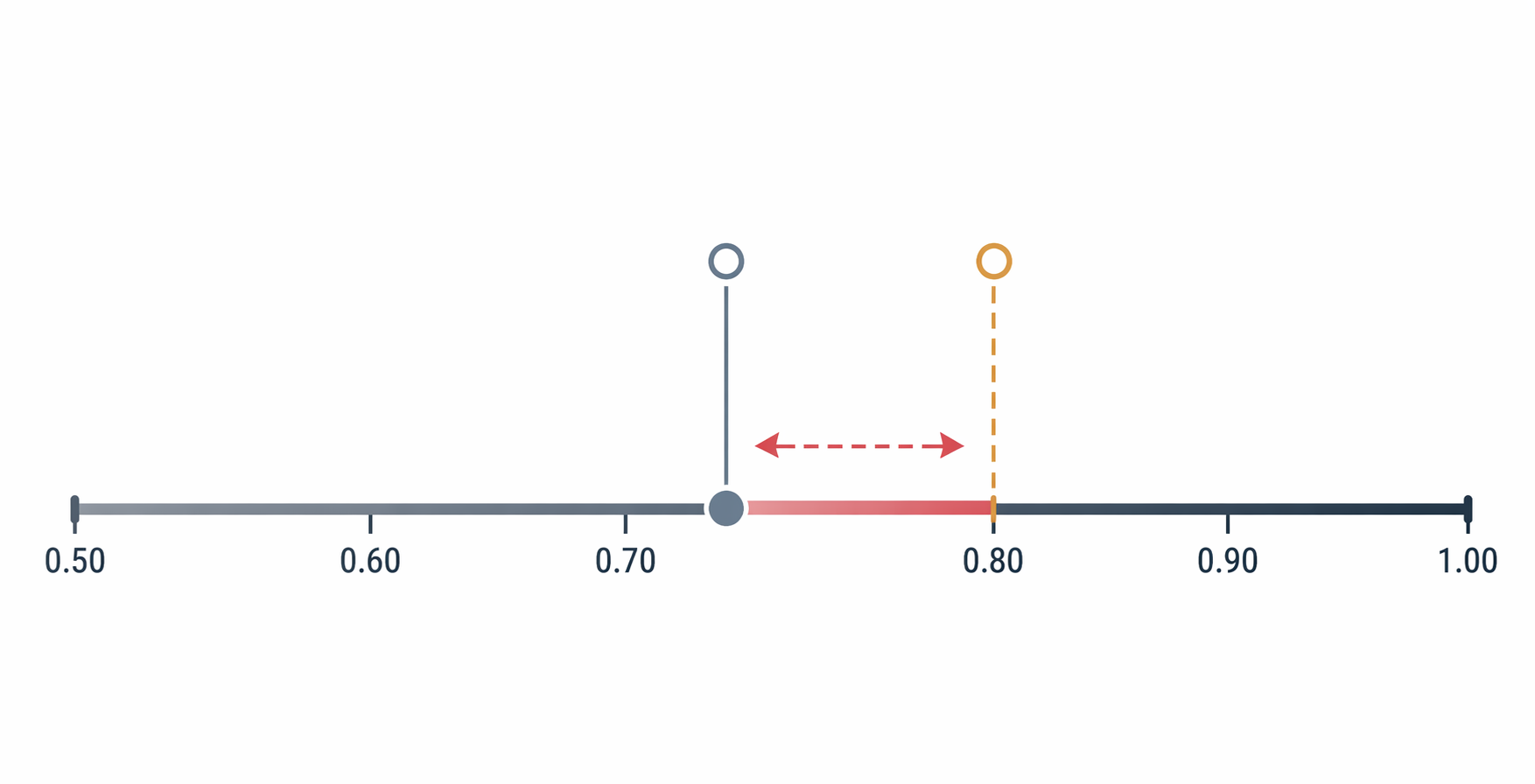
The current evidence does not justify treating AI tools as stand-alone courtroom witnesses. Machine learning systems may improve sensitivity over traditional approaches, especially where structured instruments leave risk undetected. But recidivism prediction remains around an AUC of 0.75, below the roughly 0.80 threshold treated here as clinically useful for this kind of high-stakes forensic decision-making.[1] A model can be better than a familiar instrument and still not be reliable enough for the legal burden being placed on it.
The Gap Between Better Prediction and Legal Sufficiency
Violence risk assessment was not a pristine field before AI arrived. Traditional tools have limits that deserve candor. Correlations for traditional violence risk instruments rarely exceed r=0.40, and Iozzino et al.'s 2015 meta-analysis found that up to 1 in 5 psychiatric inpatients may become physically violent.[1] Those facts are part of the reason machine learning attracts serious attention rather than mere institutional fashion.
A clinician responsible for a unit, jail diversion program, forensic hospital, or conditional release plan has reason to be interested in tools that catch risk signals missed by a structured interview or by an instrument with modest predictive strength. Sensitivity matters. Missed risk has victims, clinical consequences, and legal consequences. The problem begins when sensitivity gains are presented as courtroom readiness.
AUC is often attractive because it appears to compress performance into one clean number. It does not answer the legal question by itself. An AUC near 0.75 means the model is ranking risk better than chance and may be useful in some triage contexts. It does not tell the court whether the model's false positives are tolerable in a civil commitment hearing, whether its false negatives are tolerable in a release decision, or whether its training population resembles the person being evaluated.
The legal system does not suffer consequences symmetrically. A false negative may expose others to harm. A false positive may deprive an examinee of liberty, intensify supervision, or harden a sentencing recommendation. The same operating point on a model can therefore look acceptable to an administrator trying to prioritize reviews and unacceptable to a judge deciding whether the state has met a commitment standard.
Population Validity Is Not a Technical Footnote
The most important limitation is not that AI is new. It is that much of the evidence base for AI violence risk prediction comes from forensic or offender populations, while some of the most legally consequential uses being discussed involve civil psychiatric settings and civil commitment thresholds.[1] That is not a minor sampling concern. It changes the question being asked.
A model trained or validated in an offender population may learn signals associated with criminal justice exposure, prior arrests, institutional behavior, or documentation patterns. Those variables may carry predictive information in that setting. They may also fail to travel cleanly into a civil psychiatric population where the legal issue is dangerousness linked to mental illness, the decision is preventive detention rather than sentencing, and the documentation record has been created for different purposes.
This is where claims about AI in forensic mental health often become too broad. A tool may be promising for identifying people in a forensic hospital who need closer review. That does not establish that the same tool can justify involuntary hospitalization, extended confinement, or a court's finding of future dangerousness in a civil case. The target population, base rate, legal threshold, and available interventions all matter.
The University of Toronto scoping review protocol is useful precisely because it does not pretend this literature is settled. It notes that no prior synthesis exists of ethical and legal issues specific to AI in psychiatric violence risk assessment.[1] In Q3 2026, that gap should make legal actors slower, not faster, to treat AI violence scores as admissible expert conclusions.
Why Daubert Problems Become Clinical Problems
In ordinary clinical workflow, opacity can be irritating. In forensic work, it is a vulnerability. If a model cannot be audited, explained, or tested against the relevant population, the clinician who relies on it may be unable to defend the opinion under cross-examination. The examinee may be unable to challenge the basis for a risk label. The court may be left with the outward appearance of scientific precision without the underlying conditions that make scientific evidence testable.
Daubert-style admissibility concerns are sometimes described as legal procedure, but in this setting they are also clinical safeguards. Testability asks whether the claim can be examined rather than merely asserted. Error-rate scrutiny asks how often the method is wrong and for whom. Explainability asks whether the path from data to conclusion can be understood well enough to permit meaningful challenge. Those questions are not hostile to science. They are what keep a probability estimate from becoming an unreviewable administrative fact.
A black-box model can create a particularly awkward forensic report. The evaluator may write that the tool indicates elevated risk, but cannot say which features drove the classification, whether those features are clinically relevant, whether they are proxies for race or poverty, whether missing data altered the output, or whether the model has been validated in a population resembling the examinee. That is not a defensible opinion. It is a delegated conclusion.
This does not mean AI risk tools have no place in practice. It means their place has to be described accurately. A model can be used to prompt additional record review, flag a need for collateral interviews, identify inconsistent documentation, or support team triage. Those uses keep the tool inside a human assessment process. They do not ask the court to accept the model as an independent expert.
Confident Outputs Are Not Clinical Data
The risk of over-deference is not hypothetical. The ABPP newsletter's discussion of AI, mental health, and forensics describes ChatGPT-4 generating confidently stated predictions without sufficient clinical data.[2] The important lesson is not that a chatbot behaved badly. It is that legal and clinical readers can be drawn toward fluent certainty even when the underlying information is inadequate.
Forensic clinicians are trained to notice missing records, inconsistent collateral information, unclear symptom timelines, substance use confounds, and incentives embedded in the referral question. A fluent AI output can flatten all of that. It may produce a coherent paragraph where the appropriate professional response would be, "I cannot answer that without more data." In court, that difference is not stylistic. It is the difference between a defensible limitation and an unsupported opinion.
Legal professionals are also vulnerable to the clean surface of an AI-generated conclusion. A risk score or generated narrative may appear less biased than a clinician because it does not sound emotional, tired, adversarial, or uncertain. But absence of visible hesitation is not absence of bias. It may simply mean the uncertainty has been hidden from view.
That is why human-in-the-loop language is too weak if it merely means a person clicked approve. The human reviewer must know what data entered the model, what data were missing, what the model was validated to predict, what its error profile looks like, and whether the output changes the opinion or merely prompts further inquiry. Otherwise the clinician becomes a conduit for a conclusion that neither the evaluator nor the court can adequately interrogate.
Malingering Detection Deserves Interest, Not Exemption
Malingering detection is one of the more intriguing areas because the signal is not limited to what the examinee says. Monaro, Gamberini, and Sartori reported up to 96% accuracy in distinguishing true depression from feigned depression using mouse-movement analysis.[3] For anyone who has evaluated effort, symptom validity, or response style, that finding is difficult to ignore.
It is also easy to overstate. A mouse-movement study does not settle malingering assessment across criminal responsibility evaluations, disability claims, competency evaluations, immigration proceedings, or civil litigation. It shows that behavioral-computational signals may add something important under studied conditions. It does not eliminate the need to examine incentives, symptom consistency, medical records, collateral reports, cultural presentation, literacy, medication effects, neurologic illness, or the quality of the testing environment.
Bias concerns are especially hard to dismiss in this domain. Mouse behavior and digital task performance can be affected by device access, motor familiarity, education, disability, language, testing anxiety, and socioeconomic exposure to technology. If those factors are unevenly distributed across groups, a tool may appear to measure deception while partly measuring digital fluency or access. Documented racial and socioeconomic bias risks should keep the result in the category of promising signal, not courtroom shortcut.
Explainability matters here as much as in violence risk assessment. If a malingering tool classifies someone as feigning depression, the evaluator must be able to explain what behavioral features contributed to that classification and why those features are valid indicators rather than artifacts of the testing setup. A bare accuracy statistic does not answer the individual forensic question.
Pilots Show Experimentation, Not Readiness
Machine learning violence risk assessment pilots are underway at Duke University Health System and Waypoint Centre for Mental Health Care.[1] Those projects are worth watching. They also illustrate why implementation evidence and admissibility evidence are different things.
A pilot can show whether a tool integrates into workflow, whether clinicians use it, whether alerts are too frequent, whether documentation improves, or whether teams identify risks earlier. Those are meaningful outcomes for a health system. They do not by themselves establish that the same tool should shape testimony about an individual examinee's future dangerousness.
The harder questions come later: Was the model externally validated? Was performance stable across racial, socioeconomic, diagnostic, and age groups? Were false positives and false negatives analyzed separately? Did clinicians override the model, and when? Did the tool change outcomes or simply change documentation? Could an examinee's attorney obtain enough information to challenge the output? Until those answers are available, pilots should be cited as active experimentation rather than proof of forensic reliability.
Civil Commitment Is the Sharpest Boundary
AI-assisted risk assessment becomes most legally fraught when it intersects with civil commitment. The clinical question may be framed as risk management, but the legal act is preventive detention. That shift raises the evidentiary burden. A model that helps a hospital decide who needs a safety plan is not automatically strong enough to help the state confine someone because of predicted dangerousness.
Civil commitment requires attention to standards that differ from criminal sentencing or correctional classification. The examinee may not have been convicted of a new offense. The evidence may need to connect mental illness, dangerousness, and need for treatment. The court may require a specific legal threshold rather than a general risk ranking. A model developed in a forensic or offender population cannot fill those legal elements simply by producing a probability estimate.
This is also where racial and socioeconomic bias becomes more than an ethics paragraph. If a model overestimates risk for a group that is already more likely to experience coercive systems, the output can compound state power behind a mathematically polished surface. If the model is opaque, the affected person may not be able to identify or contest the mechanism of that overestimation.
Forensic clinicians should be careful about report language in this area. It is one thing to write that an AI-assisted review prompted examination of specific records, collateral information, or behavioral incidents that the clinician then independently analyzed. It is quite another to write that the AI tool found the person dangerous. The first statement describes a support function. The second risks attributing legal significance to a method that has not earned it.
What Responsible Use Looks Like in 2026
Responsible use begins by refusing to blur purpose. A tool used for clinical triage should be described as clinical triage. A tool used to organize record review should be described as record-review support. A tool used to generate hypotheses should be described as hypothesis generation. The more directly the output affects a liberty interest, the more demanding the validation, transparency, and accountability requirements should become.
| Use | More Defensible Role | Boundary |
|---|---|---|
| Violence risk prediction | Prompting further review, collateral gathering, safety planning, or team discussion | Not a stand-alone finding of dangerousness |
| Malingering detection | Adding one behavioral signal to a broader symptom-validity assessment | Not a substitute for clinical, collateral, and contextual analysis |
| Competency-related screening | Flagging records or symptoms that require evaluator attention | Not an independent opinion on legal competency |
| Court reports | Disclosing limited decision-support use when relevant and explainable | Not presenting opaque outputs as expert conclusions |
Several conditions should be explicit before AI output appears in a forensic mental health report: the tool's intended use, the population in which it was validated, the outcome it predicts, the time horizon if applicable, the known error profile, the handling of missing data, the possibility of bias across relevant groups, and the degree to which the evaluator can explain the output. If those conditions cannot be stated, the report should not make the model sound more settled than it is.
Clinicians also need institutional protection from quiet automation pressure. If a hospital, correctional system, or court service adopts a tool, the evaluator should not be left to defend a proprietary score without access to validation evidence. Procurement is not admissibility. Vendor confidence is not peer review. Workflow convenience is not a forensic opinion.
Legal professionals have a corresponding responsibility. They should ask whether the tool has been validated for the specific population and legal question, whether the error rates are known, whether the output is explainable, and whether the human expert independently evaluated the underlying facts. These questions are especially important as broader healthcare AI regulation continues to develop; readers tracking that landscape may also need resources such as The 2026 State Healthcare AI Law Tracker and related work on AI ethics training for clinicians.
The narrow conclusion is the safer one. AI tools in forensic mental health can be useful under human oversight, particularly when they improve detection, organize complex records, or prompt questions a clinician might otherwise miss. They should not yet be framed as independent expert evidence in court. The evidence is not empty, but it is not strong enough, transparent enough, or population-specific enough to carry that burden.
References
- Artificial Intelligence in Psychiatric Violence Risk Assessment: A Scoping Review Protocol, University of Toronto, 2025.
- AI, Mental Health and Forensics: Is This the Future?, American Board of Professional Psychology.
- Monaro, Gamberini & Sartori mouse-movement malingering detection study, 2018.
Comments
Join the discussion with an anonymous comment.