The hard part of reopening after a smoke advisory is not deciding that clean air is preferable to dirty air. It is deciding whether Thursday morning is safe enough to restart an endoscopy schedule, recall outpatient staff, tell perioperative services to stop rebooking cases, and let patients know their appointments will actually happen. For hospitals, AI in decision making for reopening after smoke advisory is useful only if it narrows that operational uncertainty before the next public advisory arrives.
Regional air quality alerts and current monitor readings can tell a facility what has happened or what is happening nearby. They do not always tell a clinic director whether the afternoon plume will clear, whether tomorrow’s readings will rebound, or whether a rural site without a nearby monitor is likely to cross its internal threshold again overnight. That is the gap modern air quality forecasting is beginning to address.

Hospitals have managed smoke before without AI. During the 2008 Sesnon and Sayre fires, Providence Holy Cross Medical Center kept operating by using HEPA filtration and manual environmental monitoring, a practical example of facilities and incident teams protecting indoor air while services continued under pressure.[1][2] Those examples are worth remembering because they show both competence and constraint: staff could measure, filter, and adapt, but they did not have a facility-specific forecast that could turn smoke recovery into a defensible reopening timeline.
The newer question is narrower than the sales pitch around AI. It is not whether an algorithm can “decide” that a hospital should reopen. It is whether a forecast can give administrators enough local lead time to prepare a phased return while still leaving the final call with incident command, facilities, clinical leadership, and institutional policy.
What the Forecast Has to Do
A useful reopening forecast has to answer a more demanding question than a public-facing air quality map. It has to estimate whether conditions at or near a specific facility are likely to remain within the organization’s acceptable range long enough to justify staff recall, room turnover, case confirmation, and patient communication.
That requires several things at once: lead time, local relevance, and enough event robustness that the estimate does not collapse on the very days when the hospital most needs it. A 24-hour picture may help a facilities team adjust filtration checks. A multiday outlook can change a scheduling decision, because elective procedures and ambulatory visits are not restarted by flipping a switch at 7 a.m.
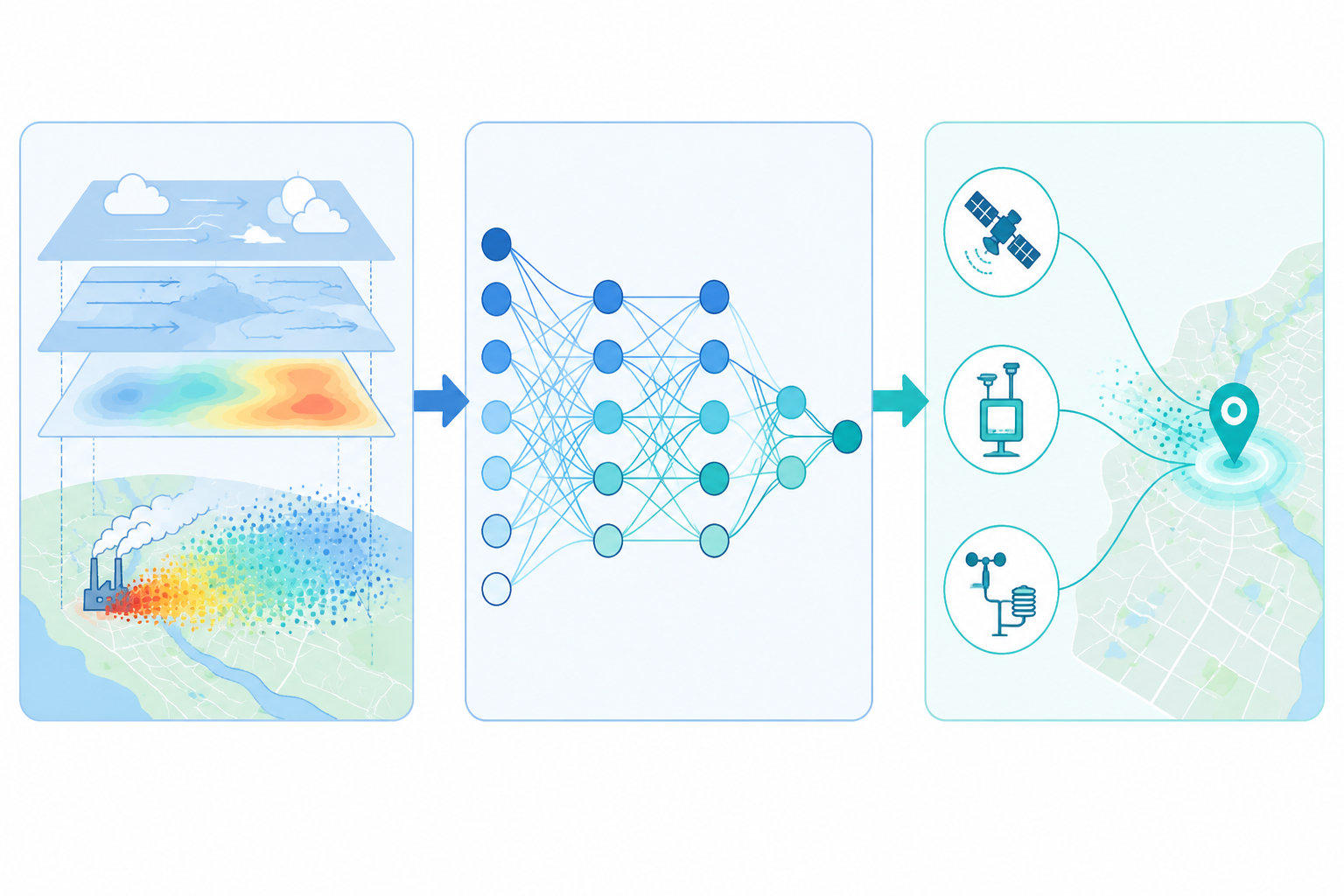
This is where hybrid AI-chemistry models become more interesting than either traditional atmospheric models or machine learning alone. Chemical transport models provide physics-based structure: emissions, atmospheric chemistry, transport, and dispersion. Machine learning can then learn local error patterns, relationships between sensor streams, and repeated conditions that a coarse regional model may miss. The operational value comes from the combination, not from treating AI as a replacement for atmospheric science.
Why Hybrid Models Matter More Than a Better Map
One reported hybrid approach, described by Fu in 2023, combined machine learning with chemical transport modeling and achieved more than 90% forecast accuracy for air quality. The same account reported that the hybrid model was 66% more accurate than chemical transport models alone and 12% more accurate than machine learning alone.[3] Those figures should not be lifted out of context and turned into a hospital reopening guarantee. They do, however, support a practical point: the best signal for operations may come from models that preserve atmospheric structure while correcting local blind spots.
For a hospital, a modest local improvement can matter. If a regional advisory says smoke is improving but the facility sits in a valley, near a recurring plume path, or far from a regulatory monitor, the regional signal may be too blunt. A forecast that better estimates the facility’s own recovery window can help operations leaders decide whether to reopen all services, reopen only low-risk ambulatory services, or keep a reduced footprint until the next forecast cycle.
More recent deep learning work also points toward stronger predictive performance, though not specifically for hospital reopening. A 2025 hybrid deep learning model combining CNN, BiLSTM, Attention, GNN, and Neural-ODE components reported an RMSE of 6.21 and an R² of 0.988 for air quality prediction.[4] The architecture matters less to a hospital executive than the implication: multiple model families are being combined to capture spatial, temporal, and nonlinear air quality behavior that a single method may not handle as well.
Still, strong air quality metrics are not the same as a validated reopening decision. RMSE and R² describe model performance against air quality targets. They do not say whether a hospital avoided unsafe exposure, reduced cancellations, protected vulnerable patients, or improved staffing reliability after using the forecast. That distinction is not academic. It is the difference between a planning input and a clinical operations decision system.
Four Days Can Change the Reopening Conversation
The most operationally useful claim in the current evidence is lead time. Trace AQ, a University of Utah spinout, forecasts wildfire smoke out to 4 days using CMAQ chemical transport modeling with machine learning augmentation.[5] A 4-day smoke outlook is not a final clearance to reopen, but it is enough time to move from passive waiting to staged preparation.
| Forecast Signal | Hospital Action It Can Support | What Still Requires Human Decision |
|---|---|---|
| Smoke expected to clear and stay below the facility’s internal threshold | Prepare a phased reopening schedule and begin patient messaging | Whether threshold criteria are met and which services return first |
| Recovery likely, but with rebound risk overnight | Hold high-disruption services, staff essential clinics, and recheck facilities readiness | Whether the rebound risk is acceptable for specific patient populations |
| Persistent smoke likely for several days | Extend cancellations earlier and reduce repeated patient rebooking | Whether emergency, urgent, or time-sensitive services need alternate pathways |
| Facility-level estimate differs from regional advisory | Escalate local review instead of relying only on regional messaging | Which source governs institutional communication and reopening authority |
In practice, the forecast would sit upstream of several workstreams. Perioperative scheduling could avoid confirming a full day of elective cases if the model suggests a likely smoke rebound. Facilities could time filtration checks and indoor air verification before staff and patients arrive. Department chiefs could prepare tiered staffing plans instead of calling everyone back on short notice. Communications teams could tell patients what is likely, what remains conditional, and when the hospital will make the next update.
The forecast does not remove the need for institutional thresholds. A children’s hospital, an oncology infusion center, and a general outpatient clinic may not use the same tolerance for residual risk. A model can estimate air quality recovery; it cannot decide whether a medically fragile population should be brought back through a smoky parking lot, whether staff can safely commute, or whether a facility’s HVAC performance is adequate that morning.
The Facility-Level Problem: Monitors Are Not Everywhere
Many reopening decisions are local even when the public advisory is regional. A hospital may have multiple clinics spread across different microclimates, or a main campus with indoor air controls that perform differently from an older ambulatory site. When the nearest regulatory monitor is not representative, administrators either overgeneralize from regional data or spend precious hours collecting local measurements before making a call.
AI-driven sensor fusion is relevant because it can estimate conditions where no physical monitor exists. One 2026 account described platforms that generate “virtual stations” estimating air quality at more than 90% accuracy in places without a physical monitor.[6] For healthcare operations, that is potentially more useful than another regional dashboard. The reopening question usually belongs to a particular building, entrance, clinic, or service line.
Virtual station estimates should still be treated as estimates. They can help flag whether a facility is likely aligned with, better than, or worse than the surrounding area. They should not replace indoor measurements, HVAC verification, or the hospital’s own environmental safety procedures. The best use is to narrow uncertainty before boots-on-the-ground checks confirm the reopening plan.
How This Becomes a Hospital Workflow
A workable reopening process would not ask a model for a yes-or-no answer. It would turn the forecast into a trigger for staged work. If the 4-day outlook shows likely improvement, incident command can authorize preparation without authorizing reopening. That distinction protects the organization from both paralysis and premature certainty.
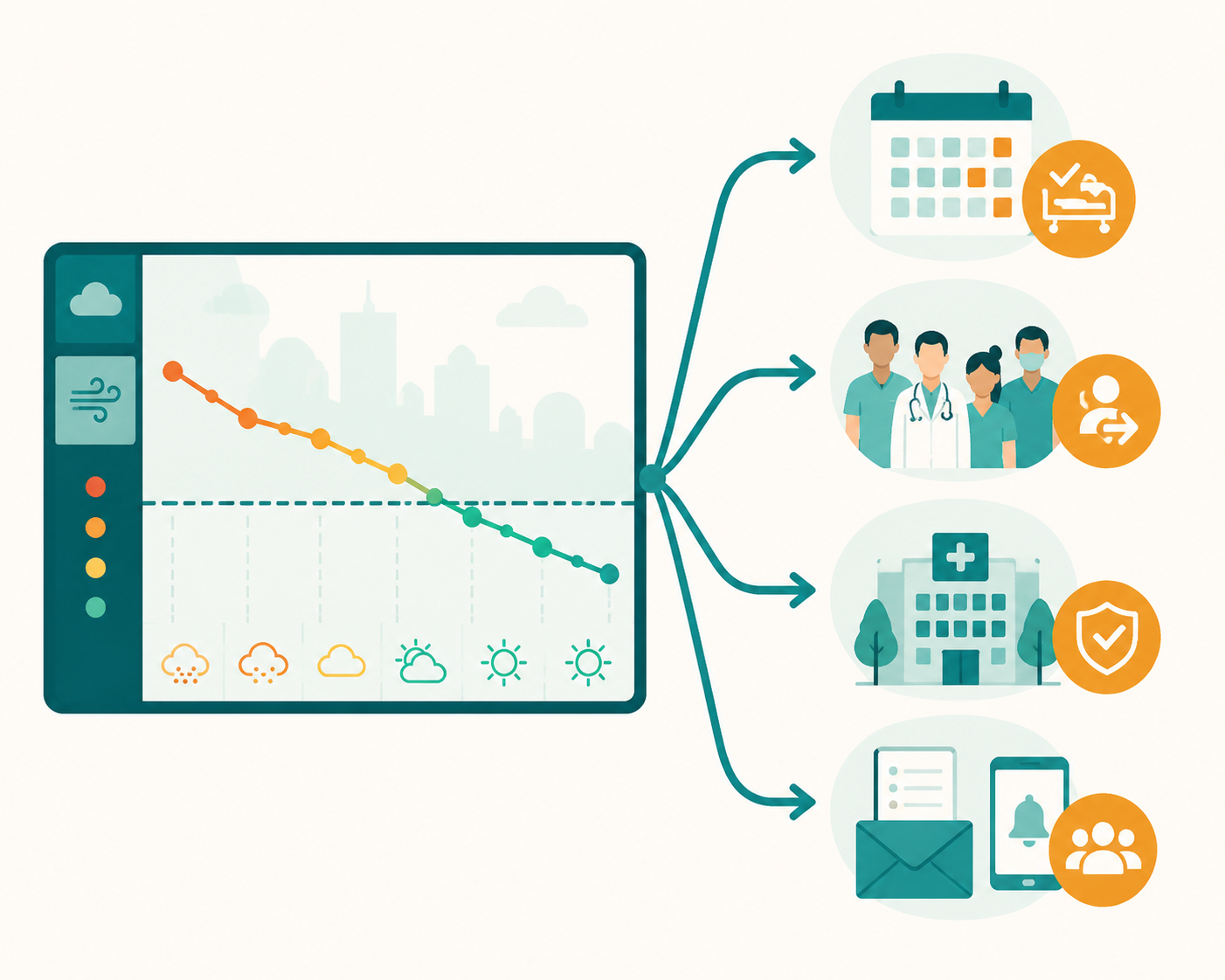
- Facilities reviews filtration status, indoor air readings, intake settings, and any smoke intrusion reports before the forecasted recovery window.
- Clinical operations identifies which services can restart first, which should remain delayed, and which require special patient screening or transport planning.
- Staffing leaders prepare recall lists and contingency coverage, especially for areas that cannot tolerate another same-day cancellation.
- Schedulers hold or release appointment blocks based on the next decision point rather than repeatedly canceling and rebooking patients.
- Communications teams draft conditional patient and staff messages that state what is reopening, what remains paused, and when the decision will be confirmed.
The operational gain is not that AI makes the decision. The gain is that the hospital starts the right work earlier. If the forecast later worsens, the organization may still cancel services, but it does so with a clearer rationale and fewer improvised handoffs. If the forecast holds, reopening is no longer compressed into the few hours after an advisory changes.
This is also where environmental forecasting differs from patient-level prediction. A hospital reopening plan has to coordinate rooms, staff, supplies, patient transportation, call centers, and public messaging. Air quality is one decisive input, but it is not the entire state of readiness.
Health-System Relevance Without Overclaiming
The broader health-system case for taking smoke forecasting seriously is strong. A 2024 Lancet paper on health system wildfire preparedness places wildfire smoke within a larger operational preparedness problem for healthcare systems.[7] That context matters because reopening is not just a facilities issue. Smoke affects demand, staff availability, respiratory risk, and the credibility of institutional communication.
Adjacent AI work on health effects is also relevant, but it does not prove the reopening use case. A 2025 pediatric hospitalization prediction study was single-center and retrospective, and external validation is still needed.[8] Studies like that may eventually help hospitals combine environmental forecasts with expected patient demand. For now, they should be read as supporting evidence that smoke-related prediction is clinically important, not as evidence that a reopening tool has been validated.
For readers focused on that adjacent question, the companion discussion of AI wildfire smoke health predictions belongs in a separate lane. Forecasting smoke concentration and predicting clinical harm are connected, but they are not interchangeable.
Where the Evidence Still Stops
The main limitation is simple: no study in the available evidence directly examines an AI system built and prospectively validated for hospital reopening after a smoke advisory. The strongest support comes from adjacent air quality forecasting, smoke forecasting, sensor fusion, and health-system preparedness evidence. That is enough to justify planning use. It is not enough to claim formal decision support validation.
Extreme wildfire events are the uncomfortable test. The 2023 discussion of hybrid forecasting explicitly cautioned that freak events such as that summer’s wildfire smoke require traditional methods too, because machine learning models can struggle when training data are sparse or conditions fall outside familiar patterns.[3] Hospitals should be especially skeptical on those days. A model that performs well in routine seasonal variation may be less reliable when smoke behavior is unprecedented, monitors are sparse, and public health consequences are highest.
There is also an integration gap. Current air quality forecasting tools do not, by themselves, know whether the hospital has enough respiratory therapists on shift, whether postponed cases have created a backlog, whether a clinic’s air handling unit passed inspection, or whether supply chain delays affect service restart. Those constraints decide whether a forecasted clean-air window is operationally usable.
That distinction will matter if these systems are embedded into clinical decision support. A forecast dashboard used by emergency management is one thing. A system that recommends reopening services, stratifies patients, or triggers clinical actions moves into a different evidence and governance category. Hospitals evaluating that path should also examine current AI clinical decision support expectations, including the issues discussed in FDA CDS guidance for AI and the broader medical AI evidence gap.
A Defensible Use Today
The safest current role for hybrid AI-chemistry smoke forecasting is as an operational planning input. It can help hospitals anticipate when air quality is likely to recover, compare facility-level conditions with regional advisories, prepare phased reopening plans, and reduce last-minute disruption for staff and patients.
The strongest systems are promising because they combine physical atmospheric modeling, machine learning correction, sensor fusion, and multiday lead time. The reported performance is good enough to deserve attention from emergency managers and operations leaders. It is not yet good enough to let the model carry the authority of reopening.
Until prospective validation catches up, the defensible posture is practical: use the forecast to start planning earlier, require local verification before reopening, preserve human incident-command judgment, and treat extreme smoke events as higher-risk conditions where traditional monitoring and conservative thresholds still matter.
References
- Health Care Facilities Maintain Indoor Air Quality Through Smoke, NOAA Climate.gov.
- Wildfire Smoke and Hospital Air Quality, California Hospital Association.
- AI can help forecast air quality, but freak events like 2023’s summer of wildfire smoke require traditional methods too, The Conversation, 2023.
- Scientific Reports article by Lilhore et al. on hybrid deep learning air quality prediction, Scientific Reports, 2025.
- U scientists develop AI-powered tool to forecast wildfire smoke, University of Utah, 2025.
- How AI Is Turning Clean Air Into a New Kind of Health Data, AI Journal, 2026.
- The 2024 Lancet paper on health system wildfire preparedness, The Lancet, 2024.
- Pediatric hospitalization prediction study by Barnett-Itzhaki et al., 2025.
Comments
Join the discussion with an anonymous comment.