For hospital hurricane preparedness, the practical question behind AI weather forecasting for hurricane preparedness in healthcare is not whether a model wins a forecast contest. It is whether a forecast arrives early enough, with enough confidence, to change the work before the narrow part of the funnel begins: patient transport, fuel contracts, oxygen deliveries, dialysis continuity, pharmacy inventory, generator testing, staff childcare, mutual-aid calls, and transfer agreements.
That is why the Hurricane Melissa forecast mattered. Google DeepMind reported that WeatherNext predicted Melissa’s Category 5 landfall in Jamaica five days in advance at about 80% confidence, rising to near 100% three days out, for a storm that rapidly intensified from Category 1 baseline winds.[1] A five-day signal does not evacuate a hospital. It does, however, move several expensive and slow decisions out of the last 48 hours, when every other institution in the region is competing for the same buses, vendors, beds, fuel, and staff attention.
Five days changes the hospital calendar
A two- or three-day hurricane forecast is already useful, but it often arrives when the hospital is shifting from planning into compression. The command center may be open, but the fragile decisions are already stacked: which patients can safely transfer, which units can shelter in place, which vendors are still reachable, whether staff can report, and whether regional partners have capacity.
A credible five-day signal creates a different kind of room. It gives operations leaders time to start work that is reversible or staged: confirming patient census categories, checking oxygen and pharmaceutical burn rates, contacting transport vendors before contracts are saturated, reviewing generator fuel posture, identifying dialysis-dependent patients, and preparing staff coverage options without yet making a final evacuation call.
The Melissa example is especially important because rapid intensification has historically been one of the most difficult hazards to fit into hospital timelines. A facility can tolerate uncertainty about a distant tropical system; it has a harder time tolerating uncertainty when a storm becomes much stronger inside the same window in which frail patients would need ambulance, air, or bus movement. WeatherNext’s reported five-day confidence did not remove the need for official National Hurricane Center synthesis, but it would have justified earlier internal watch conditions for high-consequence planning.[1]
The operational value is not the extra days alone. It is the ability to attach those days to predefined decisions. If an AI ensemble repeatedly shows a high-impact hurricane threat at day five, the useful hospital response is not to announce an evacuation. It is to start the work that makes either evacuation or shelter-in-place safer when the official forecast converges.
Where AI guidance belongs in the emergency operations workflow
The cleanest way to use AI hurricane forecasts is to treat them as an earlier uncertainty and confidence layer, not as a replacement trigger. In a hospital emergency operations center, that means the AI signal should appear before final action thresholds, alongside ensemble spread, trend direction, and comparison with official and physics-based products.
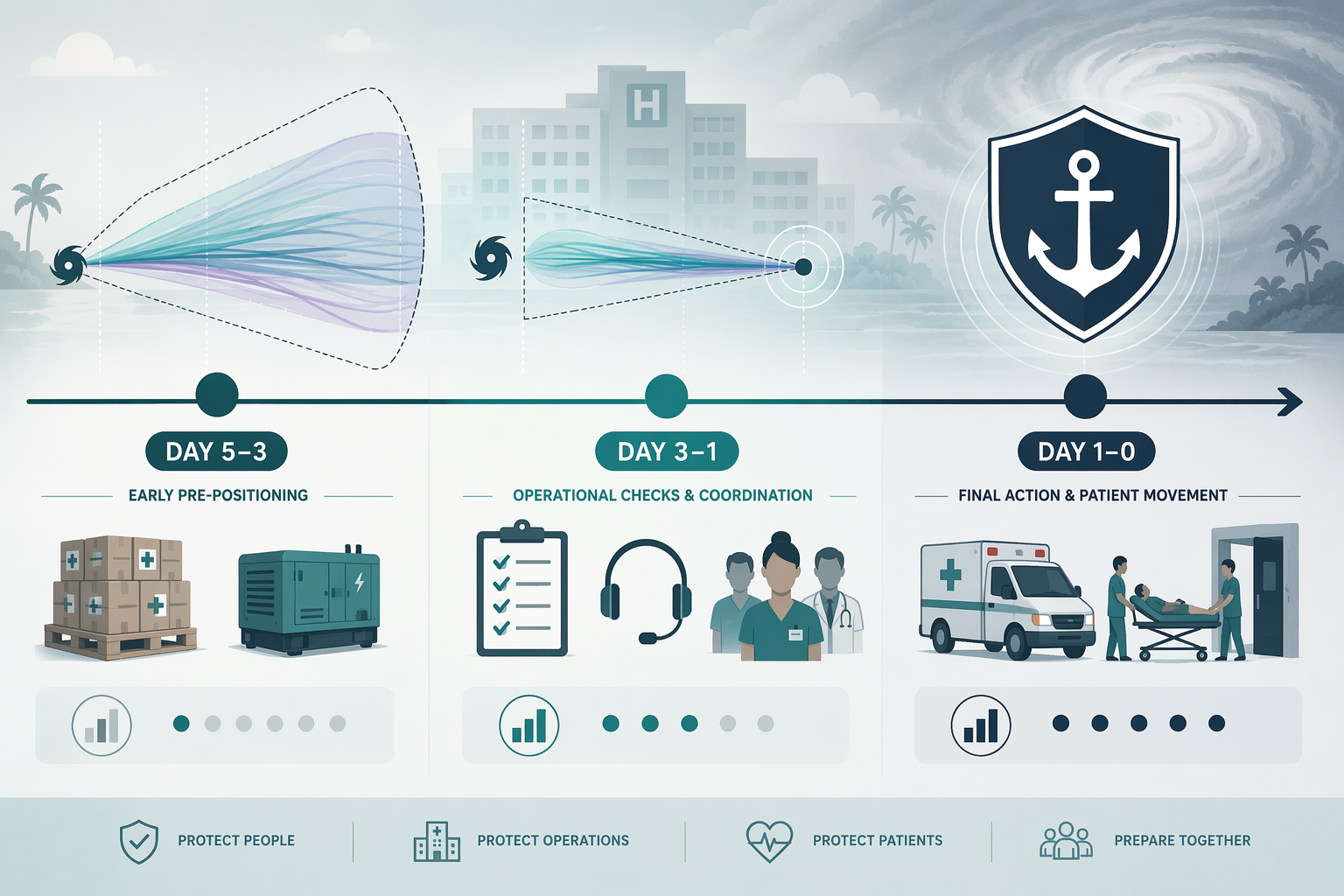
| Forecast window | AI forecast role | Hospital actions that can start | What should not happen yet |
|---|---|---|---|
| Day 5 to day 3 | Extended watch signal and ensemble confidence check | Review vulnerable patient lists, verify vendor availability, pre-stage supply conversations, check fuel and generator readiness, alert staffing leaders | Do not make final evacuation or facility closure decisions from AI output alone |
| Day 3 to day 1 | Confidence escalation when AI, NHC products, and traditional models increasingly align | Move from planning checks to staged commitments: transport holds, receiving-facility calls, pharmacy and oxygen adjustments, staff housing and childcare contingencies | Do not ignore storm size, rainfall, wind-field structure, local flood exposure, or official watches and warnings |
| Day 1 to landfall | Situational awareness and comparison layer | Execute the adopted incident action plan, monitor official updates, coordinate with emergency management, document decision rationale | Do not let a late AI run override official guidance without expert review |
The early window is where AI has the most room to help without asking it to do work it cannot safely own. If an ensemble signal is wide but repeatedly points toward a severe regional threat, the hospital can open a preparedness watch internally. That may mean a shorter command-center call, not a full activation. The point is to pull forward the checks that become painful when they wait until the forecast cone is on the front page.
By the middle window, the question becomes convergence. Are AI ensemble members tightening? Are official NHC products moving in the same direction? Do traditional physics-based models support the same timing, track, and intensity scenario? Are local emergency-management partners changing posture? When those answers begin to align, the hospital can move from reversible checks to conditional commitments.
That structure matters because hospital decisions carry asymmetric consequences. Moving medically fragile patients too early can expose them to transport risk, interrupt care, and consume scarce receiving beds. Waiting too long can leave the same patients in a facility facing wind damage, flood isolation, power failure, staffing gaps, or oxygen supply disruption. AI forecasts are most valuable when they make those tradeoffs visible earlier, not when they pretend to dissolve them.
Use ensemble spread as a threshold, not a decoration
Hospitals should avoid treating an AI model run as a single deterministic answer. The more useful object is the ensemble: how many plausible futures cluster around a damaging scenario, how quickly that cluster is changing, and whether the risk crosses a threshold already written into the emergency plan.
This is where 2026 model development becomes operationally relevant. Lowry reported that WeatherNext expanded from 50 to 1,000 ensemble members, a change that can support probabilistic confidence thresholds rather than one-off interpretation of a single forecast line.[3] For hospitals, the important phrase is not “1,000 members” by itself. It is the possibility of asking, before the official short-fuse period, whether a defined proportion of plausible outcomes would strain evacuation, supply, or staffing plans.
A hospital protocol does not need to wait for perfect certainty to act. It can define watch conditions such as: begin vendor confirmation when a high-impact regional threat persists across multiple forecast cycles; initiate transfer-bed reconnaissance when confidence rises and official guidance begins to align; reserve final evacuation decisions for official products, local hazard assessment, and executive incident command review. The thresholds should be written before the storm exists. If they are improvised during a command-center call, the model output becomes another argument instead of a decision aid.
Why NOAA’s AI models matter to hospital operations
NOAA’s AI work matters less because it is fast in the abstract and more because speed and lower computing cost can make probabilistic guidance more routine. NOAA said its AIGFS produces a 16-day forecast in about 40 minutes using 0.3% of the computing resources required by the traditional GFS, while AIGEFS extends forecast skill 18 to 24 hours beyond GEFS at 9% of the computing cost. NOAA also reported that its 62-member hybrid HGEFS consistently outperforms both GEFS and AIGEFS across most verification metrics.[2]
For a hospital, those figures point toward a practical future: more frequent ensemble refreshes, more scenarios available earlier, and better ability to see whether confidence is growing or dispersing. That does not automatically tell a facility whether a basement will flood, whether a helipad will be unusable, or whether a specific access road will close. It does make it more plausible that emergency managers will have structured probabilistic information before the usual scramble begins.
The performance story also needs careful wording. DeepMind and Lowry both cite NHC 2025 verification data indicating that Google DeepMind was the top-performing individual model for both track and intensity across the Atlantic and Eastern Pacific basins, and that the DeepMind ensemble system was best at predicting rapid intensification at two- to three-day lead times, although it struggled at short lead times.[1][3] That is important evidence, but the NHC verification report is being cited here through those secondary accounts rather than treated as directly reviewed.
The part AI forecasts still do not give a hospital
Track and intensity are not the same as facility-level hazard. A hospital fails locally. It loses power on a campus, not across a basin. Its oxygen delivery is blocked by a road segment, not by a forecast category. Its roof, loading dock, emergency department entrance, wastewater system, and transfer routes are exposed to storm structure, wind field, rainfall, surge, and timing.
That is where the limits of current AI weather models remain material. Lowry notes that AI models do not reveal internal storm features such as wind shear, structure, size, and rainfall fields in the way traditional physics-based models can. NOAA also reported that AIGFS v1.0 shows degradation in intensity forecasts, and Lowry reported that the ECMWF AI model showed “no skill whatsoever” for hurricane intensity in 2025 because of coarse ERA5 training data.[2][3]
The Rice University work belongs in this discussion, but in the right lane. A March 2026 study by Weng and Gori in JGR: Atmospheres found that Pangu-Weather and Aurora generated hurricane windfields that violated gradient wind balance and overestimated inner-core size.[4] That is not direct proof that WeatherNext has the same defect. It is evidence that some AI weather models can produce storm structures that look operationally risky if used beyond what they have been verified to provide.
For hospital leaders, the lesson is straightforward: do not convert an AI landfall or intensity signal into a campus hazard assessment. Use it to start earlier. Use traditional model fields, NHC products, local flood maps, engineering knowledge, and emergency-management intelligence to decide what the storm means for the facility.
The NHC forecast remains the governing baseline
This is not institutional politeness. In an emergency operations center, an authoritative forecast baseline matters because decisions must be explained, documented, and defended. If a hospital evacuates early, leadership needs to show why the trigger was reasonable. If it shelters in place, the same record matters after the fact.
NHC Science Operations Officer Wallace Hogsett has described AI models as providing “new, independent guidance on the range of possible outcomes,” while also emphasizing that “none of the models are perfect, and they never will be.”[5] NHC Deputy Director Jamie Rhome has characterized AI as “evolution not a revolution” that will “push humans forward.”[6] Those statements are a useful operating doctrine for healthcare: welcome the earlier independent guidance, but keep expert synthesis in charge of final action.
A layered protocol also protects staff from a familiar failure mode. Without predefined roles for AI guidance, each new model run can become a command-center debate. The transport coordinator sees risk rising. The finance lead sees avoidable cost. The nursing supervisor sees staffing disruption. The administrator waits for an official escalation. The better plan assigns each forecast layer a job before the storm: AI ensembles for early watch and uncertainty, NHC official products for authoritative baseline, traditional models for structure and fields, and local emergency management for ground truth.
A practical protocol for the 2026 season
Hospitals do not need to create a separate AI hurricane plan. They need to revise the existing hurricane annex so AI-enhanced forecasts have a defined place in the timeline. The revision should be specific enough that a night-shift supervisor and an incident commander would interpret the same signal in the same way.
- Add a day-five AI ensemble review to hurricane season procedures, focused on high-consequence regional scenarios rather than facility evacuation.
- Define internal watch thresholds before the season, including who reviews ensemble confidence, who compares NHC guidance, and who alerts supply chain, transport, pharmacy, dialysis, oxygen, and staffing leaders.
- Separate reversible actions from commitment actions, so early AI signals can trigger checks and holds without forcing premature patient movement.
- Require convergence review before major commitments: AI ensemble trends, NHC official forecast, traditional model fields, local emergency-management input, and facility vulnerability.
- Document when AI guidance influenced timing, but record final evacuation, shelter-in-place, and service-line decisions against authoritative products and local judgment.
This approach is consistent with forecast-based action frameworks already discussed in health and disaster planning. Gish and Rapaport point to anticipatory action and forecast-based financing literature showing how predefined thresholds linked to weather forecasts can activate interventions; in their January 2026 npj Digital Medicine article, they discuss this as a conceptual model rather than a documented hospital deployment.[7] For healthcare, that distinction matters. The framework is useful. The implementation still has to be built, drilled, and audited locally.
What to rehearse before the first serious forecast
The safest time to decide what an 80% five-day signal means is not during a hurricane call. Before peak season, the emergency preparedness team can run a tabletop using a hypothetical AI ensemble signal. The exercise should ask what changes at day five, what waits until day three, and what never moves without official guidance.
| Drill question | Why it matters |
|---|---|
| Who is authorized to interpret AI ensemble guidance? | Avoids informal model-watching becoming an unofficial trigger |
| Which actions are reversible at day five? | Lets the hospital act early without locking in patient movement |
| Which vendors need earlier contact? | Targets the bottlenecks most likely to disappear when regional demand rises |
| What evidence is required before transfer or evacuation decisions? | Keeps final action anchored to NHC guidance, traditional model fields, and local risk |
| How is uncertainty documented in the incident record? | Supports later review of why action began early or why escalation waited |
A drill like this should feel mundane. That is a virtue. The purpose of AI guidance in hospital preparedness is not to create a dramatic forecast moment. It is to make the first useful decisions earlier and less improvisational.
The boundary hospitals should keep
AI hurricane forecasting has moved the outer edge of preparedness. For high-consequence storms, especially where rapid intensification and landfall location are at issue, hospitals can now justify earlier internal watch conditions, earlier vendor coordination, earlier staffing conversations, and earlier review of medically fragile patients.
The same progress does not make AI a facility hazard model, an evacuation authority, or a substitute for the NHC forecast process. The practical standard for 2026 is layered: use AI forecasts to start earlier and quantify uncertainty; use NHC official guidance, traditional model output, and local emergency-management judgment to make final evacuation and facility-level decisions.
References
- How WeatherNext helped the National Hurricane Center better predict Hurricane Melissa's historic landfall in Jamaica — Google DeepMind
- NOAA deploys new generation of AI-driven global weather models — NOAA, December 2025
- AI Weather Models Changing the Hurricane Forecast Game — Lowry Substack, June 2026
- Rice University news release on Weng & Gori, JGR: Atmospheres — Rice University, March 2026
- NHC Q&A on AI and hurricane forecasting — weather.gov
- Google AI is a hurricane genius — Palm Beach Post, June 2026
- Gish & Rapaport article on agentic AI and forecast-based action — npj Digital Medicine, January 2026
Comments
Join the discussion with an anonymous comment.