Introduction: The Scale of AI Deployment in 2025–2026
The question is no longer whether artificial intelligence will enter clinical practice, but how extensively it already has. By February 2026, the FDA had authorized more than 1,357 AI-enabled medical devices — more than double the count from 2022. In 2025 alone, the agency cleared 295 AI/ML devices from 221 unique manufacturers, with a median clearance time of 142 days. The global AI healthcare market, valued at approximately $39 billion in 2025, is projected to reach $504 billion by 2032.
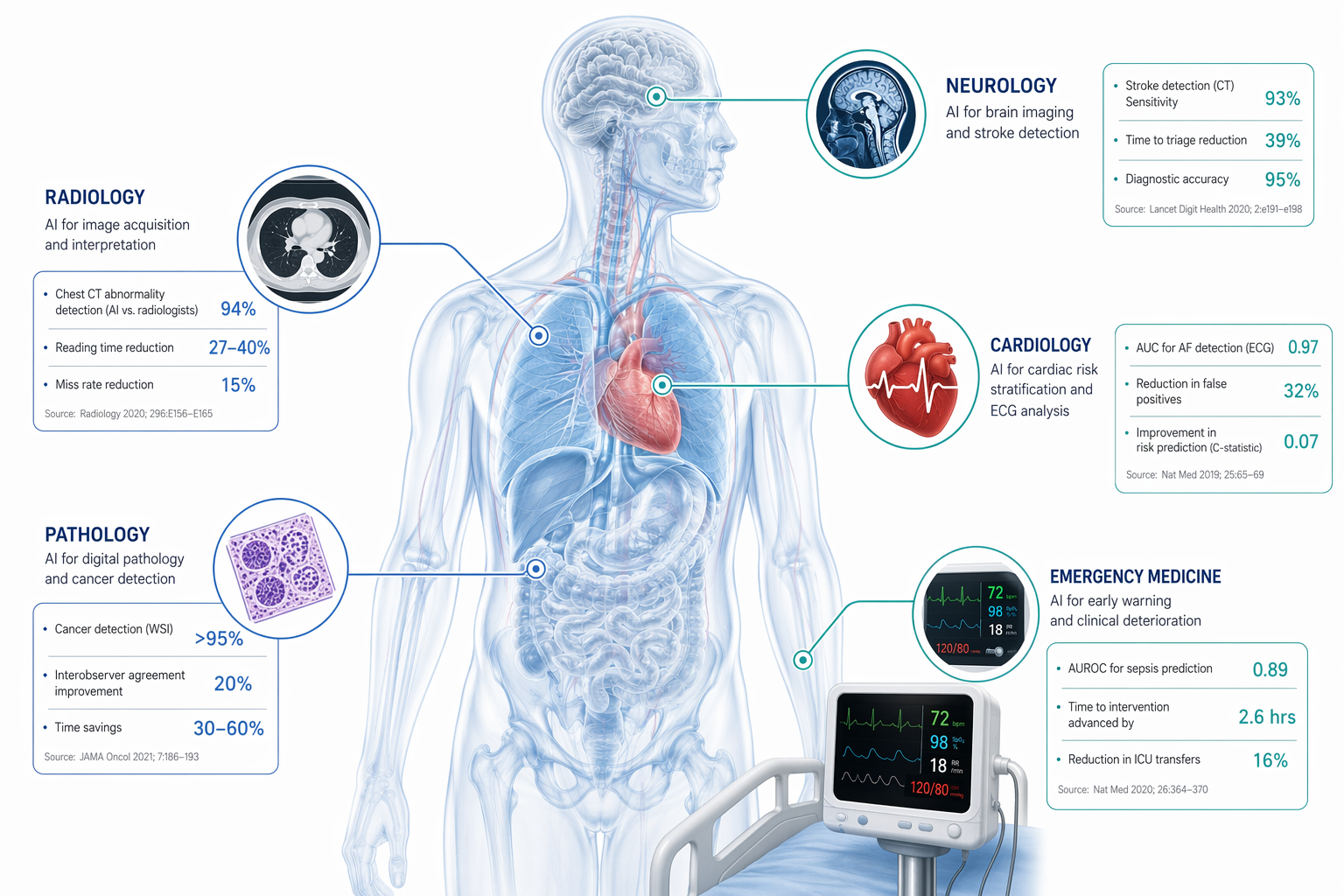
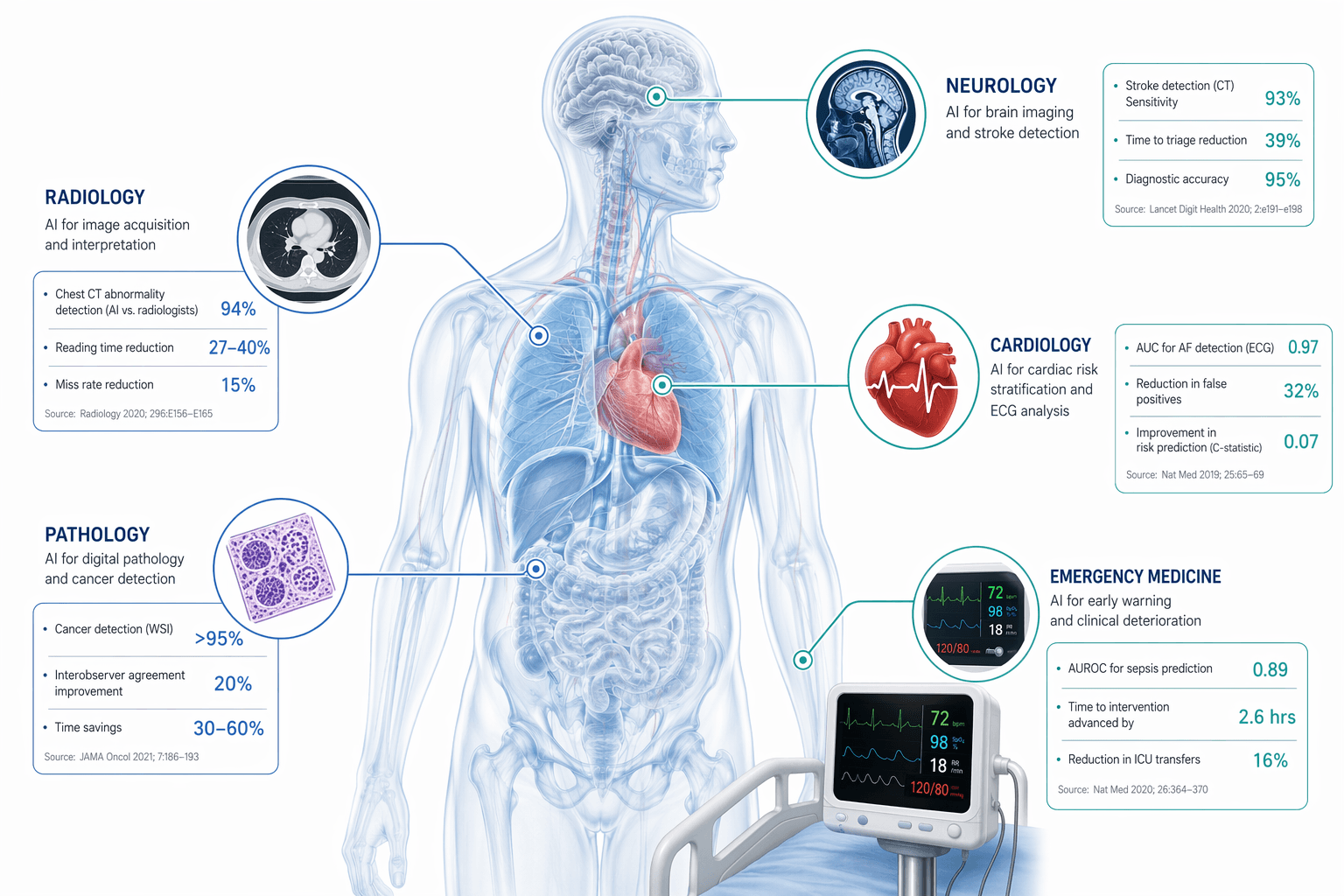
These aggregate figures, however, obscure a more important pattern: AI adoption is not uniform across medicine. It clusters in specific specialties where imaging data is abundant, workflows are repetitive, and the clinical need for speed or accuracy is acute. Radiology alone accounts for 71.5% of all FDA-cleared AI devices. Cardiology, neurology, gastroenterology, and pathology follow at much smaller shares. Understanding where AI is actually producing measurable outcomes — and where it still falls short — requires a specialty-by-specialty examination grounded in specific deployment data, not general claims.
This article provides that examination. It organizes evidence from FDA clearance records, peer-reviewed studies, and documented real-world deployments at institutions including Emory Healthcare, Mayo Clinic, Lexington Medical Center, and Assuta Hospital. Each section covers a specialty's AI footprint, concrete performance metrics, regulatory context, and known limitations. The goal is to give clinicians and health IT professionals a structured reference for where AI is yielding measurable results — and where caution remains warranted.
Regulatory Backbone: How FDA Clearance Shapes Clinical AI Adoption
Before examining specialty-specific deployments, it is essential to understand the regulatory framework that determines which AI tools reach clinical settings. The vast majority — 96% — of AI-enabled medical devices are cleared through the FDA's 510(k) pathway, which requires the device to demonstrate substantial equivalence to an already marketed predicate device. This is a lower bar than the premarket approval (PMA) pathway required for high-risk devices, and it has implications for the evidence clinicians should expect.
In 2025, the median clearance time for AI/ML devices was 142 days, with an average of 150 days. About 24% of submissions were cleared in under 90 days, while 22% took more than 200 days. Of the 295 devices cleared in 2025, 62% were classified as Software as a Medical Device (SaMD), and 63% were designated as diagnostic. Notably, 10.2% — 30 devices — were authorized with Predetermined Change Control Plans (PCCPs), which allow manufacturers to make iterative updates to algorithms without requiring a new 510(k) submission each time.
| Metric | Value |
|---|---|
| Cumulative AI/ML devices authorized (Feb 2026) | 1,357+ |
| Devices cleared in 2025 | 295 |
| Median clearance time (2025) | 142 days |
| Devices with PCCPs (2025) | 30 (10.2%) |
| Devices cleared via 510(k) | 96% |
| Radiology share of 2025 clearances | 71.5% (211 devices) |
| Cardiovascular share | 8.8% (26 devices) |
| Neurology share | 4.7% (14 devices) |
The FDA's February 2026 TEMPO pilot marks a regulatory shift toward requiring manufacturers to demonstrate measurable clinical benefit — not just technical performance — for AI devices. This matters for clinicians because it signals that future clearances may come with stronger evidence requirements. For now, however, the majority of cleared devices have not been validated in prospective, multi-center trials, and clinicians should treat FDA clearance as a safety and substantial-equivalence marker, not a stamp of proven clinical efficacy.
Radiology: The Dominant Specialty (71.5% of FDA AI Clearances)
Radiology is where AI has penetrated most deeply, and for good reason. Medical imaging generates vast quantities of standardized digital data — the ideal substrate for computer vision models. Of the 295 AI/ML devices cleared in 2025, 211 were for radiology applications. The top product code, QIH (Radiological Computer Assisted Detection/Diagnosis), accounted for 75 clearances alone. Shanghai United Imaging Healthcare led all manufacturers with 10 clearances in 2025, while 183 manufacturers had single clearances.
The following examples illustrate how radiology AI is performing in real clinical environments, with specific, quantified outcomes.
AI Lung Nodule Detection: 29% More Nodules, 26% Faster
Lung nodule detection on CT scans is a high-volume, high-stakes task where missed findings can delay cancer diagnosis. Philips reports that AI-based lung nodule detection performs the nodule search 26% faster than manual inspection and detects 29% of previously missed nodules. These figures come from studies using Philips' AI algorithms, and while the vendor source warrants caution, the magnitude of improvement is consistent with findings from independent evaluations of similar tools.
AI for Multiple Sclerosis Lesion Tracking: 44% Improvement in Diagnostic Accuracy
Monitoring disease progression in multiple sclerosis requires precise tracking of lesion burden on MRI over time. AI algorithms for MR image analysis of the brain in MS patients improved diagnostic accuracy by 44% while also reducing reading times, according to Philips. This represents a meaningful clinical gain in a condition where subtle changes in lesion count or volume can alter treatment decisions.
AI Stroke Triage: Under 60 Seconds at Lexington Medical Center
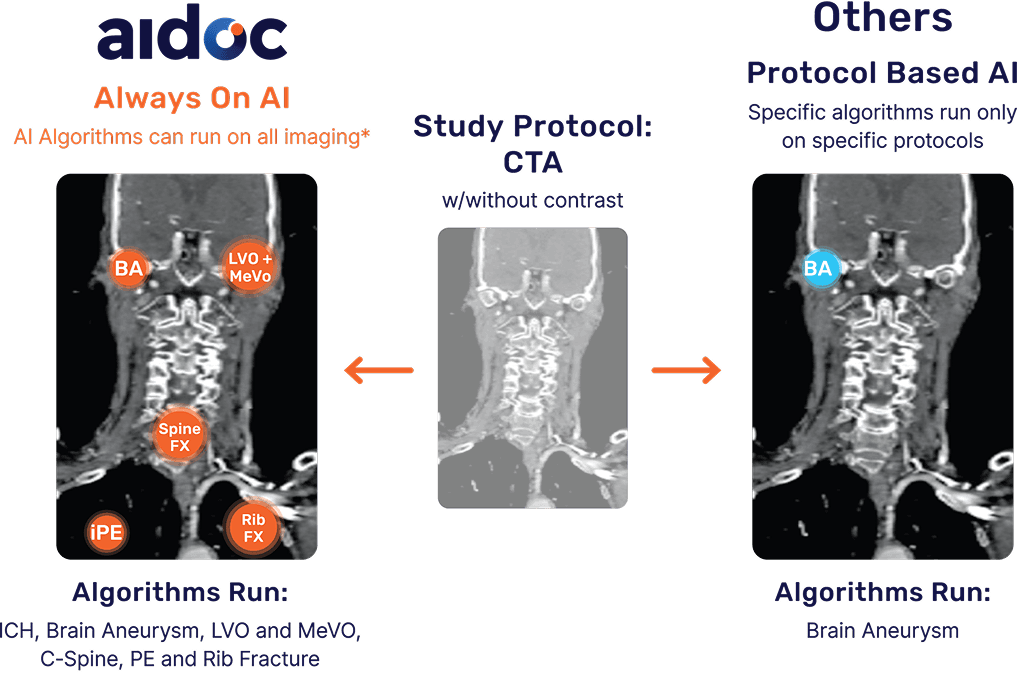
Time is brain in acute ischemic stroke. At Lexington Medical Center, an AI-powered stroke triage system (Aidoc/Brainomix) reduced notification times to under 60 seconds from image acquisition to physician phone notification. In three sampled ischemic stroke cases, the physician received an alert on their phone in less than 60 seconds, enabling stroke teams to mobilize before the emergency call was even placed. This kind of workflow compression — from minutes to seconds — is one of the clearest examples of AI delivering a measurable operational benefit that translates directly to patient outcomes.
AI for Intracranial Hemorrhage: Flagging the Missed Finding
At Assuta Hospital in Tel Aviv, an AI system flagged a post-operative brain bleed in an outpatient that clinical staff had assumed was normal. The AI's alert enabled timely intervention in a case that might otherwise have deteriorated before the next scheduled follow-up. This example highlights AI's role not as a replacement for radiologist interpretation, but as a safety net for subtle or unexpected findings.
AI CT Image Reconstruction: Reducing Radiation Dose
Philips has deployed AI-enabled camera technology that automatically detects anatomical landmarks for patient positioning in CT, reducing radiation dose and image noise. This is an example of AI operating at the acquisition stage — before any image is interpreted — to improve the quality and safety of the input data itself.
Cardiology: AI in ECG, Echocardiography, and Remote Monitoring (8.8% of Clearances)
Cardiology accounts for 8.8% of FDA AI clearances in 2025 — 26 devices — making it the second-largest specialty for AI deployment. The applications span electrocardiography, echocardiography, cardiac monitoring, and procedural planning.
AI-ECG for Low Ejection Fraction Detection
A Mayo Clinic cardiology study demonstrated that an AI algorithm applied to routine ECG tracings could identify patients at risk of left ventricular dysfunction — a weak heart pump — even when those individuals had no noticeable symptoms. This is significant because low ejection fraction is often asymptomatic until it progresses to heart failure, and ECG is a cheap, widely available screening tool. The AI essentially extracts a signal from a standard test that would otherwise require an echocardiogram to detect.
AI Cardiac Monitoring for Atrial Fibrillation
Philips' Cardiologs platform uses cloud-based AI to assist with detection of atrial fibrillation from remote ECG recordings. This is a deployment example of AI in ambulatory monitoring, where the volume of data from long-duration Holter or patch monitors exceeds what human readers can efficiently review. The AI flags likely arrhythmia episodes for clinician confirmation, reducing the time spent scanning normal tracings.
AI Echocardiography: Automated Measurements
AI-based automatic measurements in echocardiography deliver fast and reproducible echo quantification, according to Philips. Tools from companies like Us2.ai and Philips itself automate the measurement of ejection fraction, chamber dimensions, and valve gradients — tasks that are time-consuming and subject to inter-operator variability when performed manually. The reproducibility advantage is particularly relevant for serial studies where consistent measurements are needed to track disease progression or treatment response.
| Cardiology AI Application | Key Metric | Source |
|---|---|---|
| AI-ECG for low EF detection | Identifies asymptomatic LV dysfunction from routine ECG | Mayo Clinic study |
| AI cardiac monitoring (Cardiologs) | AFib detection from remote ECG recordings | Philips |
| AI echocardiography measurements | Fast, reproducible echo quantification | Philips, Us2.ai |
Neurology: Stroke Triage, Hemorrhage Detection, and EEG Analysis (4.7% of Clearances)
Neurology accounts for 4.7% of 2025 AI clearances — 14 devices — with applications concentrated in stroke imaging, hemorrhage detection, and EEG analysis. The clinical urgency of stroke care makes this specialty a natural fit for AI tools that can accelerate diagnosis and triage.
AI Stroke Triage for Large Vessel Occlusion
The Lexington Medical Center deployment described in the radiology section is equally relevant here: AI for large vessel occlusion (LVO) detection on CT angiography delivers results in under 60 seconds, enabling rapid mobilization of neurointerventional teams. Aidoc and Brainomix are among the companies with FDA-cleared tools for this indication. The clinical impact is straightforward — every minute saved between imaging and groin puncture in thrombectomy cases correlates with improved functional outcomes.
AI for Cerebral Hemorrhage Detection
The Assuta Hospital case — where AI flagged a post-operative brain bleed that staff had assumed was normal — illustrates the safety-net function of AI in neurology as well as radiology. Intracranial hemorrhage can be subtle on non-contrast CT, especially in post-surgical patients where expected post-operative changes may obscure new bleeding. AI tools trained to detect even small hemorrhages can serve as a second reader that does not fatigue.
AI-Powered EEG Analysis
AI analysis of EEG data for seizure detection is an emerging application. While the sources do not provide specific quantified outcomes for this use case, the underlying logic is similar to cardiac monitoring: long-duration EEG recordings generate enormous data volumes, and AI can flag abnormal patterns for neurologist review, reducing the time spent on normal recordings.
Gastroenterology and Pathology: AI in Endoscopy and Digital Pathology
Gastroenterology and urology together account for 2.4% of 2025 AI clearances — 7 devices — while pathology AI devices are tracked separately but represent a growing category. Both specialties share a common workflow pattern: visual inspection of tissue or endoscopic images where AI can act as a second reader to improve detection rates.
AI-Assisted Colonoscopy Polyp Detection
AI-assisted colonoscopy systems such as Medtronic's GI Genius and Iterative Scopes' SKOUT have received FDA clearance for polyp detection. These tools overlay real-time bounding boxes on the endoscopic video feed to highlight polyps that might be missed during withdrawal. The clinical endpoint is adenoma detection rate (ADR), a key quality metric in colonoscopy. Studies have shown that AI assistance improves ADR, though the magnitude varies by study design and baseline ADR of the endoscopist.
Digital Pathology AI for Cancer Diagnosis
In pathology, AI tools such as Paige Prostate and Ibex Galen have received FDA authorization for tasks including prostate cancer detection and breast cancer lymph node metastasis screening. These tools analyze digitized whole-slide images and flag regions of interest for pathologist review. The deployment stage varies: some tools are in broad clinical use at major academic centers, while others remain in pilot phases. The key limitation is that digital pathology requires whole-slide scanning infrastructure, which is not yet universal.
Emergency Medicine and Sepsis Prediction: AI Early Warning Systems
Emergency medicine and hospital-wide early warning systems represent a different category of AI deployment: instead of analyzing images, these tools process continuous vital sign data and laboratory results to predict clinical deterioration before it becomes apparent to clinicians.
AI Early Warning Systems: 35% Fewer Adverse Events, 86% Fewer Cardiac Arrests
Philips reports that AI-enabled early warning systems that automatically monitor vital signs and calculate early warning scores reduced serious adverse events in the general ward by 35% and cardiac arrests by more than 86%. These figures come from a hospital study, and while the vendor source warrants caution, the magnitude of the reduction is striking. The mechanism is straightforward: AI algorithms detect subtle changes in heart rate, respiratory rate, blood pressure, and oxygen saturation that precede clinical deterioration, and alert nursing staff before a code blue is called.
AI Sepsis Detection: Mortality Reduced from 20.54% to 15.27%
Sepsis remains one of the most challenging conditions to detect early. A 2025 study published in Nature Digital Medicine, cited by GlobalMed, found that AI sepsis detection reduced in-hospital mortality from 20.54% to 15.27% — an absolute reduction of 5.27 percentage points — with 88% accuracy. This is one of the strongest quantified outcomes for any clinical AI application, and it comes from a peer-reviewed source rather than a vendor publication.
- AI early warning systems: 35% reduction in serious adverse events, 86% reduction in cardiac arrests (Philips hospital study)
- AI sepsis detection: In-hospital mortality reduced from 20.54% to 15.27%, 88% accuracy (Nature Digital Medicine, 2025)
- AI for pulmonary embolism management: Real-time alerts and remote physician access at Emory Healthcare (Aidoc)
- AI for aortic dissection triage: Automated surgeon notification at HOAG Hospital (Aidoc)
Cross-Cutting Evidence Themes, Limitations, and What Clinicians Should Watch For
Across all specialties, several cross-cutting themes emerge from the evidence. These patterns are as important for clinicians to understand as the individual deployment examples.
Performance Benchmarks: Accuracy and Efficiency Gains
GlobalMed reports that AI diagnostic imaging achieves 92% accuracy compared to 78% for manual interpretation, with a 35% reduction in average diagnosis time. The estimated return on investment for diagnostic imaging AI ranges from 451% to 791% over five years, though these figures are consultancy-sourced and should be treated as estimates rather than verified benchmarks.
Ambient AI documentation — which uses natural language processing to generate clinical notes from patient encounters — has been deployed at 62.6% of Epic-using hospitals, saving 15,791 hours across 7,260 physicians. Of physicians using these tools, 84% reported improved patient communication and 82% reported improved physician satisfaction. These are operational metrics rather than clinical outcomes, but they address a well-documented source of clinician burnout.
| Cross-Cutting Metric | Value | Source |
|---|---|---|
| AI diagnostic imaging accuracy vs. manual | 92% vs. 78% | GlobalMed (consultancy-sourced) |
| Reduction in average diagnosis time | 35% | GlobalMed |
| ROI for diagnostic imaging AI (5-year) | 451–791% | GlobalMed (consultancy-sourced) |
| Ambient AI documentation adoption (Epic hospitals) | 62.6% | GlobalMed |
| Physician hours saved (ambient AI) | 15,791 hours across 7,260 physicians | GlobalMed |
| Physicians reporting improved communication | 84% | GlobalMed |
| Physicians reporting improved satisfaction | 82% | GlobalMed |
Critical Limitations: Error Rates, Bias, and Generalizability
The same evidence that shows AI's promise also reveals its vulnerabilities. A Healthcare AI Trends 2026 analysis, cited by GlobalMed, found that AI medical models produce severely harmful clinical recommendations in up to 22.2% of cases, with even top-performing models making 12 to 15 severe errors per 100 cases. This figure should be interpreted cautiously — the original study methodology should be reviewed — but it underscores a critical point: AI performance in controlled validation studies does not always translate to real-world clinical settings.
Dataset bias is a persistent concern. Skewed training datasets can cause AI systems to perform poorly on demographic groups that were underrepresented during development, potentially exacerbating health disparities in diagnosis and treatment. Many FDA-cleared devices have not been prospectively validated on diverse populations, and clinicians should ask vendors for performance data stratified by age, sex, race, and ethnicity before adopting a tool.
- Severe error rates: Up to 22.2% of AI recommendations may be severely harmful in some models (Healthcare AI Trends 2026; methodology should be reviewed)
- Dataset bias: Skewed training data can produce disparities in diagnosis and treatment across demographic groups
- Generalizability gaps: Performance in controlled studies may not replicate in real-world clinical settings with different equipment, protocols, and patient populations
- Vendor-published evidence: Many performance figures come from manufacturers rather than independent researchers
- Regulatory limitations: 510(k) clearance does not require prospective clinical trials; FDA clearance is not equivalent to proven clinical efficacy
Actionable Guidance for Clinicians Evaluating AI Tools
Based on the evidence reviewed across specialties, clinicians and health IT professionals can apply the following framework when evaluating an AI tool for adoption:
- Verify the regulatory status: Is the device FDA-cleared? What pathway (510(k), De Novo, PMA)? Does it have a PCCP for updates? Check the FDA's AI-enabled medical devices list.
- Examine the evidence base: Was the tool validated in a prospective, multi-center study? Was the study conducted by independent researchers or the vendor? Is the study population demographically similar to your patient population?
- Assess the deployment context: Has the tool been deployed in a clinical setting similar to yours? What integration method was used (EHR-embedded, standalone, PACS-integrated)? What were the documented failure modes?
- Understand the limitations: What are the known performance gaps? Has the tool been tested on the specific imaging protocols, equipment, or patient populations at your institution?
- Plan for monitoring: How will you track the tool's performance over time? Model drift — where AI performance degrades as clinical data distributions shift — is a documented risk that requires ongoing surveillance.
AI in healthcare has moved decisively beyond the proof-of-concept phase. With over 1,357 FDA-authorized devices, documented reductions in mortality and adverse events, and growing adoption across specialties, the technology is now a permanent part of the clinical landscape. But the evidence also makes clear that AI is not a uniform solution — its performance varies by specialty, by specific use case, by deployment context, and by patient population. The clinicians and health systems that will benefit most are those who approach AI with the same evidence-critical rigor they apply to any other clinical tool: asking for the data, examining the limitations, and monitoring the outcomes.
Comments
Join the discussion with an anonymous comment.