AI in medical research is now visible in the machinery, not just the conference slides. NIH AI/ML funding rose 233% on an inflation-adjusted basis from FY2019 to FY2023, reaching $2.3 billion, or 4.7% of the total NIH budget.[1] In private markets, AI companies captured 55% of all health tech funding in 2025, up from 29% in 2022, while the average health AI deal size rose 42% to $29.3 million.[2] More than 173 AI-originated drug programs are now reported in clinical development.[3] Regulators, meanwhile, have moved from watching AI claims to qualifying tools and writing credibility expectations for their use in drug development and trials.[5][7]
That is enough to retire the idea that AI medical research is still mainly experimental deployment. It is not enough to declare that drug development has been solved. The strongest evidence sits in early discovery, protocol work, recruitment, selected trial analytics, and regulatory scaffolding. The decisive evidence still has to come from pivotal trials, standardized data flows, and approvals that survive the same scrutiny as any other medical product.

The Budget Signal Is Real, But Not Permanent
Public research funding matters because it changes what laboratories, data cores, biostatistics groups, and clinical centers are asked to build. The NIH AI/ML increase through FY2023 is not a small pilot-line item; at $2.3 billion, it made AI and machine learning a measurable part of the federal biomedical research portfolio.[1] That kind of allocation tends to leave institutional residue: shared datasets, model evaluation teams, computational infrastructure, grant-review norms, and training programs that remain after individual projects end.
The caveat is timing. The NIH data cited here ends in FY2023, and current projections anticipate NIH budget contraction for FY2026. A four-year funding surge shows that AI became a serious biomedical research priority; it does not guarantee a straight-line expansion. If the federal budget tightens, the field will learn which AI programs are treated as core infrastructure and which were easier to fund when the line was rising.
Venture capital is a different signal. It shows appetite, not validation. Still, the shift from 29% of health tech funding going to AI companies in 2022 to 55% in 2025 suggests that investors are no longer treating AI as a side feature in health technology.[2] The larger average deal size points in the same direction: companies are raising money to build platforms, datasets, trial networks, and regulated products, not just demos.[2]
Drug Discovery Has the Cleanest Acceleration Story
The most concentrated evidence for AI’s impact is in the movement from target selection and molecule design into clinical development. Pipeline tracking reports more than 173 AI-originated drug programs in clinical development, with AI-discovered molecules showing 80–90% Phase I success rates versus an approximately 52% historical industry average.[3] That comparison is attention-worthy, but it needs a slow reading. Phase I mostly asks whether a candidate can be given to humans within an acceptable safety and pharmacokinetic frame. It is not a proof of efficacy, and the AI-originated sample remains small.[3]
The early-discovery compression is easier to credit because it concerns work AI is structurally suited to affect: search, design, prediction, prioritization, and iteration before a full clinical program begins. A BCG/Wellcome Trust estimate cited by Drug Target Review says AI-enabled workflows compress early discovery timelines by 30–40%, reducing preclinical candidate development to 13–18 months.[4] That does not remove toxicology, manufacturing, site activation, enrollment, or clinical follow-up. It does change the front end of the queue.

Insilico Medicine’s rentosertib is the case that makes the discussion less abstract. The program reportedly moved from AI discovery to preclinical development in 30 months, compared with roughly six years in a traditional process, and positive Phase IIa results were published in Nature Medicine in June 2025.[4] It is the kind of example that matters because it attaches AI not to a slide-deck promise but to a named compound, a disease program, a development timeline, and a peer-reviewed clinical milestone.
It is also not the finish line. As of mid-2026, no AI-discovered drug has achieved full FDA approval, and the first such approval is still projected for the 2026–2028 window.[3] The same pipeline tracking expects 15–20 AI-originated programs to enter pivotal trials in 2026.[3] Those entries will be important, but they are tests, not trophies. Phase III is where the model’s early advantage meets larger populations, longer timelines, comparator arms, operational variability, and endpoints that may not cooperate with elegant preclinical logic.
| Measurement | What It Supports | What It Does Not Yet Prove |
|---|---|---|
| 30–40% early discovery timeline compression | AI can accelerate candidate identification and preclinical prioritization | Total drug-development timelines will fall by the same proportion |
| 80–90% Phase I success for AI-discovered molecules | Early safety and human-entry signals are promising | Phase III efficacy or approval probability is established |
| Rentosertib Phase IIa publication | A named AI-discovered program has reached a meaningful clinical milestone | An AI-discovered drug has achieved full FDA approval |
| 15–20 projected pivotal-trial entries in 2026 | The pipeline is approaching decisive clinical tests | Those trials will succeed |
That distinction is where a lot of AI drug-discovery commentary still gets loose. A better molecule-design workflow can be valuable before it produces an approved drug. It can reduce dead-end chemistry, help teams prioritize mechanisms, and move stronger candidates into humans faster. But the industry’s hardest attrition has never been confined to the first design sprint. Biology still extracts its fee later.
Clinical Trials Are Becoming the Integration Layer
If drug discovery is where AI gets its cleanest acceleration story, clinical trials are where infrastructure integration becomes most visible. A trial protocol has to be written, reviewed, budgeted, opened, recruited, monitored, analyzed, amended, and submitted. Every one of those steps creates delay. AI does not need to cure a disease on its own to change the cost and cadence of research operations.
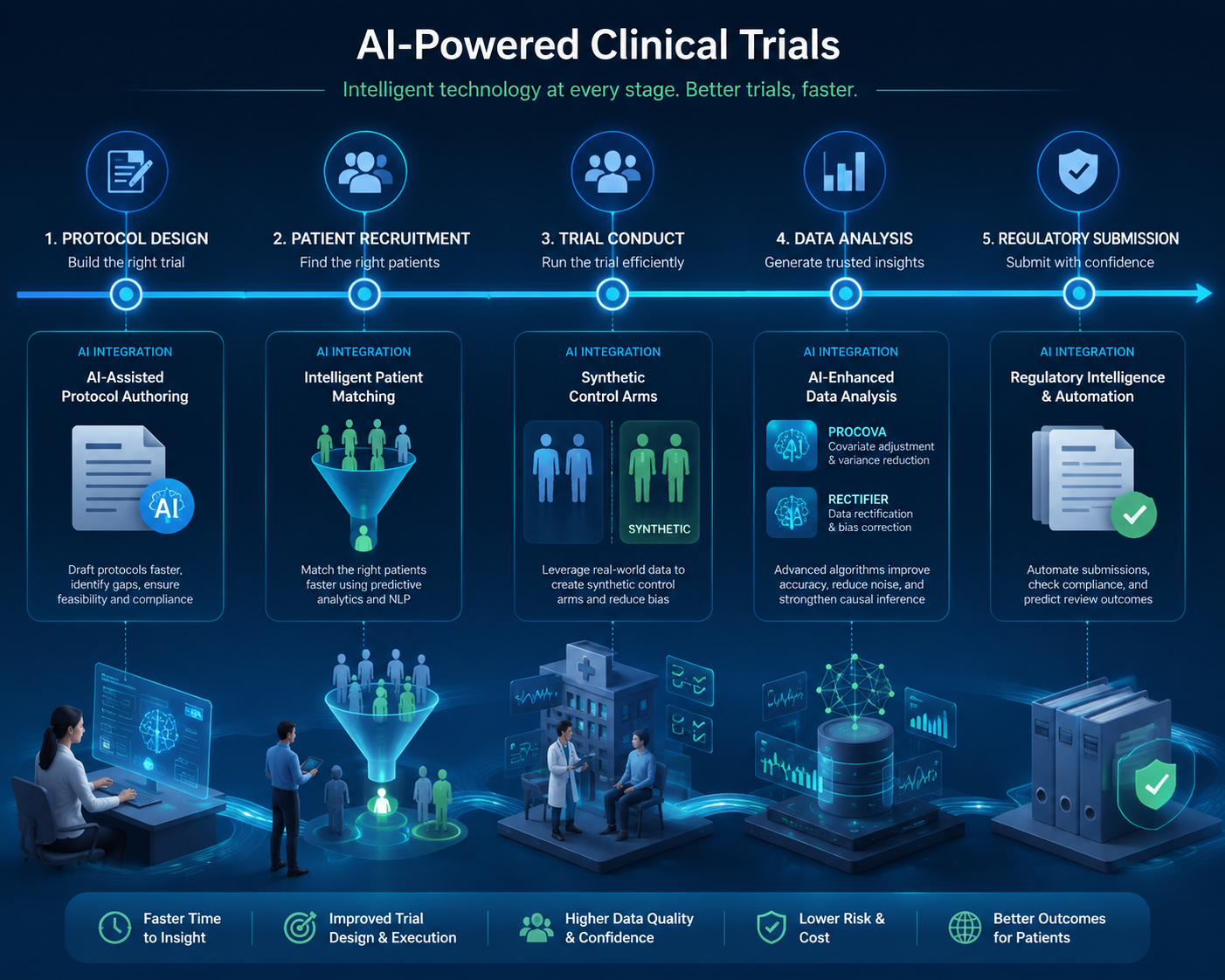
Protocol authoring is one of the lower-drama changes, and it may be one of the more scalable. The Stanford HAI 2026 AI Index cites evidence that large language model-assisted medical writing reduces protocol authoring time by approximately 30%.[5] That measurement does not say the protocol is better. It says a labor-intensive document process can move faster. In a research organization managing dozens or hundreds of studies, that is not a cosmetic gain.
Recruitment is higher stakes because it controls whether a well-designed study becomes an actual study. The AI Index cites Nature Digital Medicine evidence that AI-driven recruitment strategies can reduce trial costs by about 70% and shorten enrollment timelines by up to 40%.[5] Those figures should be read as evidence that matching, outreach, and screening can be materially improved in some settings, not as a guarantee that every hard-to-enroll population suddenly becomes reachable. Recruitment still depends on inclusion criteria, site access, patient trust, transportation, competing studies, and whether the clinical question matters to the people being asked to participate.
Synthetic control arms sit closer to the statistical core of trial design. Mass General Brigham’s 2026 predictions cite the potential for synthetic control arms to reduce needed control patients by 20–50%.[6] Used well, that can matter ethically and operationally: fewer participants assigned to control, smaller trial footprints, and faster reads in settings where external data are credible. Used poorly, it can import bias from historical or real-world datasets that were never collected to answer the trial’s question.
The regulatory qualifications are more important than they may look. In December 2025, FDA qualified its first AI-based tool for use within clinical trials: a NASH/MASH liver biopsy scoring tool.[5] That is not a general blessing for AI scoring. It is a specific qualification in a specific context. But it changes the tone of the conversation. The question becomes not whether an AI tool is impressive, but whether it is reliable enough for a defined role in a regulated trial.
Unlearn.AI’s PROCOVA methodology shows another path into trial operations. The ARISE State of Clinical AI Report 2026 says the European Medicines Agency qualified PROCOVA for use as a primary analysis in Phase 2 and 3 trials, with FDA CDER confirming alignment.[7] The point is not that synthetic or prognostic borrowing should become routine everywhere. The point is that regulators are beginning to evaluate AI-enabled trial methods as analyzable components of a protocol, rather than leaving them in the category of sponsor enthusiasm.
Screening tools are a more concrete operational example. Mass General Brigham’s RECTIFIER tool screens heart failure trial patients with reported accuracy of 97.9–100% at $0.11 per patient.[6] The cost figure is almost startling because screening is usually where sites burn coordinator time on patients who may never randomize. If a tool can reliably narrow that worklist, the benefit lands directly on trial staff and participants: fewer wasted chart reviews, fewer dead-end calls, faster identification of eligible patients.
Sponsor-level cadence is the broadest signal. Novartis reported a 10–15% reduction in overall trial duration from AI deployment, according to the Stanford HAI AI Index.[5] A sponsor-reported operational metric is not the same as an independently reproduced trial endpoint. It does, however, describe the kind of change that large R&D organizations actually care about: cycle time across portfolios, not just model performance in a benchmark dataset.
Regulators Are Turning AI Into an Assessed Component
Regulatory activity now spans devices, drug development, and trial methods. FDA authorized 258 AI medical devices in 2025, a sign that AI has already entered clinical product pipelines at scale.[5] But the evidence base behind many authorized AI devices remains uneven: among those with clinical studies, only 2.4% were supported by randomized trial data, according to the Stanford HAI 2026 AI Index.[5] That figure is useful mainly as a warning against treating authorization volume as equivalent to clinical proof.
For drug development, the more relevant shift is credibility assessment. FDA issued draft guidance in January 2025 on AI credibility assessment, and guiding principles for AI in drug development followed in January 2026, as summarized in the ARISE report.[7] These documents do not freeze the technology. They begin to define what sponsors must show when an AI model influences a decision: the context of use, the consequences of error, the quality of the data, the evaluation method, and the degree of human oversight.
That is the right regulatory direction because AI in medical research is not one thing. A model drafting a protocol synopsis carries different risk from a model identifying a patient for trial outreach. A tool scoring a biopsy for an endpoint carries different risk from a model prioritizing molecules before IND-enabling studies. The regulatory problem is not whether to approve or reject AI in the abstract. It is how to make each use case auditable enough that sponsors, investigators, patients, and agencies understand what role the model played.
The Bottleneck Is Still the Data Beneath the Model
The least fashionable constraint is still the most durable one. Harvard Medical School’s insight piece cites 68% of executives naming poor data quality as the primary reason AI initiatives fail.[8] The Stanford HAI AI Index also notes continuing challenges in data standardization, labeling consistency, and cross-institutional interoperability.[5] These are not side issues for AI medical research. They decide whether a model trained in one environment can be trusted in another.
Poor data quality is not only missing fields or messy codes. It can mean inconsistent endpoint labeling, different imaging protocols across sites, unrecorded changes in standard of care, demographic gaps, shifting laboratory methods, or real-world datasets that capture billing behavior better than biology. A model may look strong because it learned the habits of one institution. The failure may not appear until a sponsor tries to deploy it across trial sites, health systems, or countries.
This is also where the infrastructure phase becomes expensive. Building usable medical research data is not a one-time extraction job. It requires governance, provenance, labeling standards, consent frameworks, privacy controls, monitoring for drift, and people who understand both the clinical workflow and the statistical consequences of what is missing. AI can automate parts of the stack, but it cannot make weak source data clinically meaningful by assertion.
The Q3 2026 Benchmark
By Q3 2026, the practical benchmark is clear. AI medical research has infrastructure: federal funding lines, venture-backed companies, clinical pipelines, protocol-writing tools, recruitment systems, synthetic-control methods, qualified trial tools, and regulatory guidance. The field has enough measured operational gains to be taken seriously even before the first full AI-discovered drug approval arrives.
It has not earned the right to treat early acceleration as late-stage success. Phase I performance, faster preclinical candidate development, and shorter trial operations are meaningful signals, but pivotal-trial outcomes remain the harder test. The first full AI-discovered drug approval is still forecast rather than achieved, and the data-quality problem remains large enough to break otherwise plausible initiatives.[3][8] The infrastructure phase is real. The proof burden has simply moved downstream.
References
- NIH funding for artificial intelligence and machine learning in biomedical research: A cross-sectional study, JMIR,
- State of Health AI 2026, Bessemer Venture Partners,
- AI Drug Development Pipeline, IntuitionLabs / Axis Intelligence,
- AI in drug discovery: predictions for 2026, Drug Target Review,
- 2026 AI Index Report: Medicine, Stanford HAI,
- 2026 predictions about artificial intelligence, Mass General Brigham,
- State of Clinical AI Report 2026, ARISE,
- AI in clinical research: opportunities, limitations, and what comes next, Harvard Medical School,
Comments
Join the discussion with an anonymous comment.