The uncomfortable starting point for AI in medication adherence for Tourette syndrome is not a new algorithm. It is a small clinical number: in a 2019 study of 204 pediatric patients with Tourette syndrome in western China, only 40.7% reached “high adherence” on the eight-item Morisky Medication Adherence Scale while taking tiapride.[1] That finding is useful because it makes a familiar clinic problem measurable. It is also limited: tiapride is not FDA-approved, the cohort was geographically specific, and the result cannot be casually transferred to U.S. practice with aripiprazole, haloperidol, pimozide, alpha-2 agonists, or other treatment patterns.
Still, the study catches something clinicians recognize. A child may arrive with tics still visible, a parent may report that the medication “didn’t really work,” and the visit has to move quickly through school trouble, sleep, anxiety, and dose changes. Whether the medication was taken consistently can become a delicate side question. If it is asked too bluntly, the visit can feel accusatory. If it is not asked clearly, poor response and inconsistent use are easily confused.
Nonadherence in Tourette syndrome is also clinically plausible before anyone invokes forgetfulness. The CDC’s Tourette syndrome treatment page states plainly that people may stop medications because of side effects, and it names weight gain, stiffness, and tardive dyskinesia among concerns relevant to antipsychotic treatment.[2] For a pediatric patient already managing visible tics, the burden is not abstract. A medication that quiets a tic but adds weight gain, sedation, stiffness, or fear of a movement disorder can become difficult to justify at home.

What AI can see, and what it cannot
The practical question is narrower than whether AI can “improve adherence.” In Tourette syndrome, the better question is which part of the adherence problem an AI system is trying to see. A missed dose is only the visible endpoint. Before that may come an adverse effect, a parent-child negotiation, embarrassment about taking medication, uncertainty about benefit, or a clinician’s decision to increase a dose when the real issue is intermittent use.
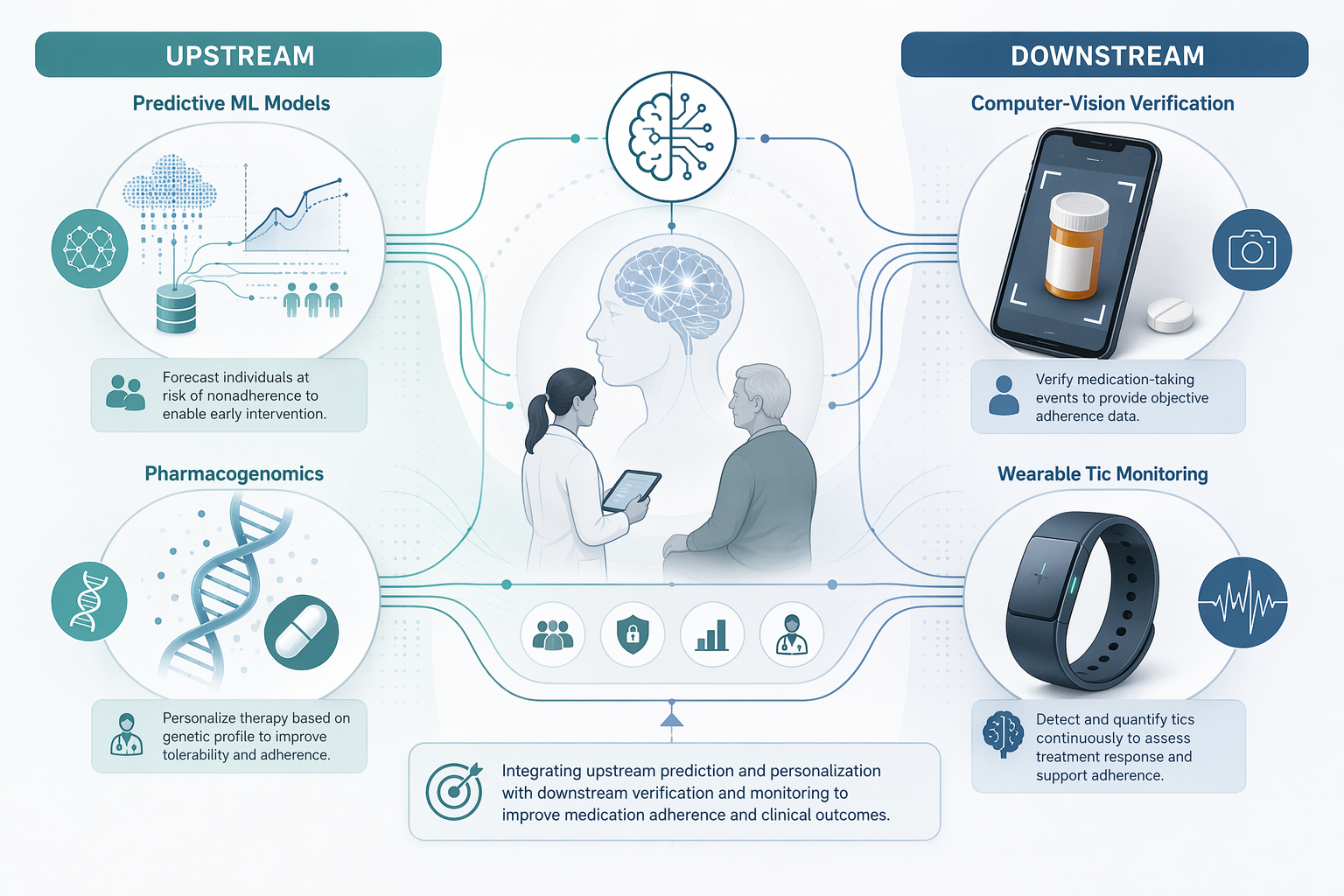
| Clinical job | What the tool may add | Evidence boundary |
|---|---|---|
| Forecasting adherence risk | Flags patients likely to struggle before repeated missed doses become established | Strongest evidence comes from non-TS adherence modeling; TS-specific prospective validation is absent |
| Side-effect-aware treatment selection | Uses pharmacogenomic and biomarker information to reduce avoidable adverse reactions | Mechanistically relevant, but not yet a validated TS adherence intervention |
| Computer-vision ingestion verification | Confirms medication-taking events when proof of ingestion is clinically justified | Promising in other conditions; ethically more sensitive in pediatric tic disorders |
| Tic and symptom monitoring between visits | Measures symptom patterns that office visits miss and may help interpret treatment response | TS-specific measurement tools are developing, but samples are small and external validation is limited |
This distinction matters because adherence technology can drift into surveillance language. A system designed to help a family explain why a drug became intolerable is different from a system designed mainly to prove that a child swallowed a pill. Both may have a place. They should not be treated as ethically or clinically interchangeable.
Forecasting risk before the missed dose
Predictive adherence models are attractive in Tourette syndrome because they intervene before the follow-up visit turns into a debate about whether the medication “failed.” The best use case is not a generic reminder notification. It is a risk signal that tells the clinician which patient is likely to struggle and why: prior inconsistent refills, adverse-effect vulnerability, family complexity, comorbid anxiety or ADHD, symptom fluctuation, or early reports that the treatment feels worse than the tic.
The precision-medicine literature reviewed in 2026 describes machine-learning approaches that have reached AUC values around 0.83–0.87 for medication adherence forecasting, along with interpretable methods such as SHAP to identify influential variables.[3] That level of discrimination is not trivial. It suggests these models can separate higher-risk from lower-risk patients better than chance and may be useful for triage, especially when clinicians have limited time.
But AUC is not a care plan. A model may rank risk accurately and still fail if the clinic has no acceptable action to take. In Tourette syndrome, a usable forecast would need to change a decision: scheduling an earlier side-effect check, choosing a drug with a more tolerable profile for that child, involving caregivers differently, or avoiding a premature dose escalation. The model would also need to be tested in the population where it is used, because adherence behavior in pediatric tic disorders is not the same clinical object as adherence behavior in hypertension, diabetes, or schizophrenia.
A systematic review of AI tools for patient adherence support shows the field moving beyond simple reminders toward risk prediction, tailored messaging, and decision support, but it does not establish that these approaches have been prospectively validated for Tourette syndrome.[4] That is the evidence boundary clinicians should keep in view: useful methods exist, but TS-specific clinical validity remains unproven.
Personalizing the first prescription may matter more than reminding the patient later
The most important adherence intervention may happen before the first missed dose. If a medication is intolerable, reminders only make the problem more punctual. For Tourette syndrome, AI-assisted precision medicine is therefore more interesting when it helps clinicians anticipate side effects or drug response than when it merely automates nudges.
The 2026 precision-medicine review highlights pharmacogenomic and biomarker approaches relevant to neuropsychiatric treatment selection, including CYP2D6 and COMT genotyping and SHAP-identified biomarkers such as beta-2-microglobulin and 25-hydroxyvitamin D.[3] The same research direction includes the possibility that pharmacogenomic-guided selection could reduce adverse reactions by more than 30%, although that should be read as a precision-medicine signal rather than as proof that a Tourette-specific adherence program already works.[3]
The clinical appeal is straightforward. If a child is more likely to experience adverse effects from a particular medication or dose, a clinician may be able to choose differently at the start, monitor earlier, or explain the tradeoff more honestly. That could reduce the kind of silent discontinuation that later appears in the chart as poor response.
This is also where overclaiming is easiest. CYP2D6 and COMT are not adherence measures. Biomarkers are not family preferences. A pharmacogenomic recommendation can reduce one source of treatment burden while leaving others untouched: stigma, cost, pill-taking routines, school-day logistics, or disagreement between a parent and child about whether tic reduction is worth the side effect profile. Precision medicine becomes an adherence tool only when it changes tolerability, perceived benefit, or follow-up decisions in a way patients and families can actually live with.
Verification is powerful, but pediatric tics make the ethics sharper
Computer-vision adherence platforms occupy a different clinical space. Instead of forecasting risk or personalizing treatment, they try to verify that medication was taken. Pharmacy Times reported AiCure data showing 89.7% adherence in the platform group compared with 71.9% in the control group, a result that helps explain why computer-vision verification attracts attention in adherence research.[5]
For some clinical scenarios, verification may be appropriate. If a medication has meaningful risk, if a trial depends on accurate exposure data, or if a family explicitly wants help documenting use without relying on memory, smartphone-based confirmation can be useful. It may also protect patients from unnecessary medication changes when the real issue is missed doses.
Tourette syndrome adds a complication that should not be brushed aside. A child with visible tics may already feel watched by classmates, relatives, and clinicians. Asking that child to record ingestion can feel less like support and more like another layer of scrutiny unless consent, data handling, and clinical purpose are handled carefully. The question is not whether verification technology can work in general; it is whether it is acceptable, proportionate, and clinically necessary for this patient and this decision.
The evidence boundary is again important. AiCure and similar adherence tools have not been prospectively validated in a Tourette syndrome population. Evidence from schizophrenia, diabetes, hypertension, or trial adherence cannot be treated as direct proof for pediatric tic disorders. At most, it shows that ingestion verification is technically and operationally plausible in other settings, and that TS-specific acceptability and outcome studies would be worth doing.
Tic monitoring is adjacent to adherence, not the same thing
Wearables and video-based tic detectors do not prove medication adherence. They measure symptoms. That makes them adjacent to the adherence problem rather than a substitute for adherence assessment. Their value is that they may show what ordinary visits miss: tic frequency outside the office, temporal patterns across the day, response after a dose change, or mismatch between reported improvement and observed tic burden.
A 2026 review of digital health and AI in Tourette syndrome describes a rapidly developing measurement layer, including wearable sensors, video detection, digital therapeutics, and neuromodulation tools.[6] The same review context includes small studies such as Cernera et al.’s sEMG-plus-accelerometry work, which reported 96.7% accuracy distinguishing tics from voluntary movements in a sample of 17 participants, and video-based facial tic detection studies by Wu et al. and Brügge et al. reporting approximately 95% and 88% accuracy, respectively, in small samples.[6]
Those numbers are encouraging, but they need careful handling. A system that recognizes facial motor tics in a constrained video dataset may not capture subtle tics, complex motor tics, vocal tics, suppressibility, premonitory urges, or the social context in which a tic becomes disabling. Small samples can also inflate apparent performance, especially when external validation is limited. For adherence work, the risk is mistaking better tic measurement for a complete explanation of medication-taking behavior.
Even with those limits, symptom monitoring could change a clinic visit in a useful way. If tic frequency worsens during a week when a family reports full adherence, the clinician may look harder at dose, drug choice, comorbidity, sleep, or stress. If tic burden improves when use is consistent but adverse effects become intolerable, the conversation shifts from “try harder to take it” to “is this benefit worth this burden?” That is a better clinical question.
Neupulse and digital behavioral care show why measurement alone is not enough
Neupulse is a useful example because it is not primarily an adherence product. In a Nottingham-led double-blind randomized controlled trial with 121 participants, the wrist-worn device was associated with more than 25% reduction in tic frequency and more than 35% reduction in tic severity; it later received a conditional NICE recommendation, though final NHS-use status and marking requirements remain unresolved as of Q3 2026.[7] This sits beside, rather than inside, medication adherence. If a non-drug device reduces tic burden, the medication decision may change: dose, need, side-effect tolerance, and family preference can all be reconsidered.
The same is true for digital behavioral therapy. The ORBIT platform and online exposure and response prevention matter because behavioral access is uneven; the research brief notes that fewer than 20% of young people in the UK access behavioral therapy. Digital therapeutics may reduce reliance on medication for some patients, but that is not the same as improving adherence to medication. It may instead reduce the need to ask a child to persist with a drug whose adverse effects outweigh its benefit.
Drug development can also change the adherence equation
AI tools are not the only way the adherence gap may narrow. Better-tolerated treatments would matter directly. Cincinnati Children’s reported phase 3 results for ecopipam in 216 participants, including a 50% relapse reduction, with publication in JAMA Neurology in May 2026.[8] Ecopipam is not yet FDA-approved, so it should not be treated as a current standard option. Its relevance here is simpler: adherence is easier when the treatment burden is lower.
That point should keep AI claims modest. If a patient stops medication because of weight gain, stiffness, sedation, or fear of tardive dyskinesia, an app cannot turn an intolerable regimen into an acceptable one. It can help clinicians detect the problem earlier, document patterns more clearly, and avoid confusing nonuse with nonresponse. It cannot remove the need for better treatment choices.
What a responsible pilot would actually test
A clinically serious AI adherence pilot in Tourette syndrome would not start by asking whether an app increases logins. It would ask whether the tool changes a decision that matters. The comparator should be usual care, not enthusiasm. The population should include pediatric TS patients receiving medications used in the relevant health system. Outcomes should distinguish adherence, tic severity, side effects, family burden, acceptability, and medication changes.
- For predictive models: test calibration, external validation, false-positive burden, and whether risk flags lead to earlier useful intervention.
- For pharmacogenomics: measure adverse effects and treatment continuation, not only genotype-actionability.
- For computer-vision verification: evaluate consent, child acceptability, privacy protections, and whether verification prevents inappropriate dose escalation.
- For wearables and video tools: separate tic detection accuracy from medication adherence and validate performance across motor, complex, and vocal tic presentations.
- For all tools: specify who reviews the alert, how quickly, and what clinical action is allowed.
The last item is often where adherence technology succeeds or fails. A risk score that no one reviews is decoration. A camera verification event that triggers blame damages trust. A wearable tic graph that leads automatically to a dose increase may harm a patient whose medication use has been inconsistent because the adverse effects were unacceptable. Workflow is not an implementation detail; it is part of clinical validity.
The Q3 2026 judgment
The adherence gap in Tourette syndrome is real, underrecognized, and clinically consequential. Yang et al.’s 40.7% high-adherence finding is not a universal prevalence estimate, but it is enough to make complacency difficult.[1] The CDC’s side-effect warning makes the behavior understandable rather than mysterious.[2]
AI can help close parts of that gap. Predictive models may identify patients likely to struggle. Pharmacogenomics and biomarker-informed selection may reduce avoidable adverse reactions. Computer-vision platforms may verify use when proof of ingestion is proportionate and wanted. Wearables and video tools may make tic patterns visible between visits, helping clinicians avoid confusing symptom fluctuation, drug nonresponse, and inconsistent medication use.
As of Q3 2026, however, no AI adherence platform has been prospectively validated in a Tourette syndrome population. The responsible position is readiness for targeted research and cautious workflow pilots, not broad clinical adoption. The best tools will not be the ones that watch children most closely. They will be the ones that help clinicians and families see treatment burden sooner, respond without accusation, and make medication decisions that a child can realistically sustain.
References
- Medication adherence and its associated factors among children with tic disorders in western China. PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC6848256/
- Treatment and Intervention for Tourette Syndrome. CDC. https://www.cdc.gov/tourette-syndrome/treatment/index.html
- AI-driven precision medicine. Frontiers in Computational Neuroscience. 2026. https://www.frontiersin.org/journals/computational-neuroscience/articles/10.3389/fncom.2026.1772244/full
- Systematic review of AI tools for patient adherence support. Frontiers in Digital Health. 2025. https://www.frontiersin.org/journals/digital-health/articles/10.3389/fdgth.2025.1523070/full
- AI-Driven Solutions Promote Medication Adherence. Pharmacy Times. 2024. https://www.pharmacytimes.com/view/ai-driven-solutions-promote-medication-adherence
- Digital health and AI in Tourette syndrome. Frontiers in Psychiatry. 2026. https://www.frontiersin.org/journals/psychiatry/articles/10.3389/fpsyt.2026.1765768/full
- Clinical trial for Tourette’s device. University of Nottingham. https://www.nottingham.ac.uk/news/clinical-trial-tourettes
- New med to manage Tourette syndrome shows promise in phase III clinical trial. Cincinnati Children’s. https://scienceblog.cincinnatichildrens.org/new-med-to-manage-tourette-syndrome-shows-promise-in-phase-iii-clinical-trial/
Comments
Join the discussion with an anonymous comment.