A wearable-to-EHR integration with AI can sound clean until the data starts moving. A heart rate sample does not leap from an Apple Watch, Garmin, Oura Ring, or Fitbit into a clinician’s workflow because a platform advertises FHIR support. It leaves a consumer device, usually passes through a phone or vendor cloud, reaches an ingestion endpoint, gets associated with a patient identity, is normalized against some expected schema, is checked for quality, is mapped into clinical data structures, is filtered for relevance, and only then appears somewhere a clinician might actually see it.
That route is the real integration problem. The hard part is not proving that wearable data can be collected. It is deciding which version of that data becomes part of care, how it is represented, what gets suppressed, what creates an exception, and who is expected to respond when the system says something changed.

The route from device to chart is already visible
A useful starting point is the Garmin-to-FHIR prototype published in Frontiers in Digital Health in October 2025. The project used Garmin Vívoactive 4 data, moved it through the Fitrockr SDK, and loaded transformed data into a Kodjin FHIR server. Steps, heart rate, heart rate variability, sleep, and stress scores were represented as FHIR Observation resources, with Patient resources also created in the server environment.[1]
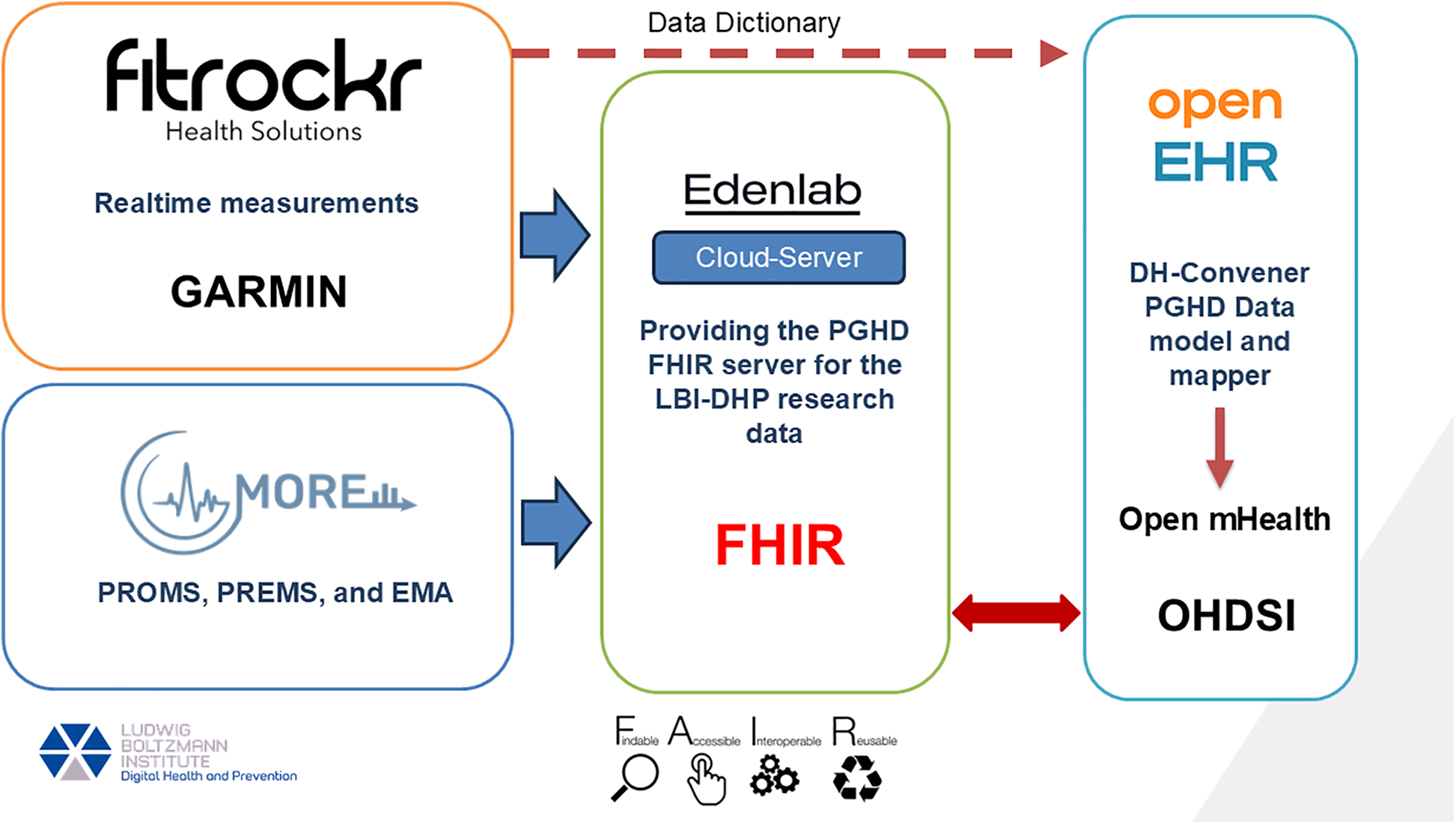
That prototype matters because it shows the full direction of travel. Device data is not dropped into the EHR as a native Garmin payload. It is mediated. The wearable output is collected, transformed, and expressed in a standard clinical exchange format before it reaches the server that could sit near an EHR integration layer.
It should also be read at the right scale. A successful Garmin Vívoactive 4 pathway is not the same as a governed clinical program that accepts several consumer brands, multiple firmware versions, patient-owned phones, intermittent sync behavior, consent changes, and clinicians with no appetite for another unmanaged queue. The prototype proves technical feasibility. It does not make production complexity disappear.
Reference architectures from wearable integration vendors describe a similar layered route: device, mobile gateway, cloud ingestion, normalization and validation, FHIR mapping, AI triage or alert filtering, and then an EHR-adjacent dashboard or clinician-facing surface.[2][3] The consistency is useful, even when the sources are commercial. The pattern keeps reappearing because there is no responsible shortcut from consumer telemetry to the clinical record.
Where the clean diagram starts to fail
The first failure point is identity and access. Each wearable ecosystem has its own account model, permissions, token behavior, cloud APIs, and device-to-phone synchronization assumptions. A patient may authorize access once, revoke it later, replace a device, leave a phone offline, or use two apps that report overlapping measures. Before a clinical system can worry about interpretation, the ingestion layer has to know whether today’s payload belongs to the right patient, whether permission still exists, and whether a missing segment means the patient deteriorated or the device simply stopped syncing.
The second failure point is schema mismatch. One brand may expose sleep as stages, another as a score, another as intervals with confidence flags. Heart rate may arrive as samples, zones, daily summaries, resting estimates, or workout-specific series. Stress and readiness metrics are especially awkward because they often combine proprietary calculations with device-specific assumptions. Calling all of these “wearable data” hides the fact that they are not the same clinical object.
The third failure point is time. Continuous or near-continuous data is not a lab result. It has sampling intervals, gaps, bursts, summary windows, and device-specific aggregation logic. A heart rate value during sleep, during exercise, after device removal, or during poor sensor contact can mean different things. If the integration pipeline strips away context too early, the EHR receives a number that looks precise but has lost the conditions that made it interpretable.
A June 2026 Sahha market analysis estimated that integrating three to five wearable brands can require up to 12 months because of differences in data formats, authentication systems, and metric definitions.[4] That is a vendor estimate, not an independently verified benchmark. Still, it is directionally believable to anyone who has watched an interface team spend weeks on one “simple” field that turns out to be differently defined by every source system.
Normalization is not a formatting chore
Middleware earns its place in the architecture at the normalization layer. This is where native device outputs are turned into a smaller set of internally consistent clinical data objects. It is tempting to describe that work as mapping fields. In practice, it is closer to adjudication.
A normalization engine has to decide what kind of observation it is receiving, what unit is being used, what time interval the value represents, whether the source is a raw sample or a derived score, whether the value was measured or inferred, and whether the payload contains enough metadata to be trusted. It also has to preserve provenance. A sleep duration estimate from a consumer ring and a sleep measure from a formal sleep study should not collapse into the same undifferentiated bucket just because both contain hours.
| Pipeline point | What can go wrong | What middleware has to decide |
|---|---|---|
| Authentication | Tokens expire, consent changes, device accounts do not match patients | Whether data can still be accepted and attributed |
| Schema intake | Brands expose different objects for similar measures | Which internal concept the payload represents |
| Metric definition | A score or summary may be proprietary or device-specific | Whether it can be compared, trended, or only displayed with source context |
| Sampling behavior | Values arrive at different intervals with gaps or bursts | Which time window the observation actually describes |
| FHIR mapping | Native payloads do not match clinical exchange resources directly | Which Observation fields, codes, timestamps, units, and provenance should be populated |
| Exception handling | Missing data may reflect nonwear, sync failure, or clinical change | Whether to suppress, flag, or route the issue |
This is why direct wearable-to-EHR feeds are structurally brittle. If every device connector maps straight into a chart destination, each brand drags its own definitions into the clinical environment. The EHR then becomes the place where differences are discovered too late, often by the analyst investigating a clinician complaint or by the clinician staring at a value that does not behave like the last value from a different device.
FHIR helps, but only after this work has happened. A FHIR Observation resource can carry the measured concept, value, unit, timestamp, subject, device, and other useful context. It does not, by itself, decide whether a vendor’s “stress” score is clinically comparable to another vendor’s stress output, or whether a daily resting heart rate summary should be trended against five-minute samples. FHIR is the exchange structure. Middleware is where the interpretation and governance decisions are enforced before the structure is populated.
The Garmin prototype shows the right kind of boundary
The Garmin-to-FHIR prototype is helpful precisely because it does not pretend that Garmin data is already clinical data. The pathway uses Fitrockr as a data hub, transforms selected Garmin measures, and represents them in FHIR resources on a Kodjin server.[1] That middle movement is the important part. It is the difference between forwarding device exhaust and producing an object a clinical system can reason about.
Production programs have to make the same boundary more explicit. Which wearable measures are eligible for ingestion? Which are stored only for patient-facing context? Which are allowed to influence a clinician-facing summary? Which values are discarded because their source, interval, or confidence is inadequate? These are not cosmetic configuration choices. They decide whether a clinician sees a meaningful signal or inherits a loosely governed data lake with an EHR tab attached.
The EHR is the wrong shape for raw wearable streams
Most EHR workflows are organized around encounters, orders, results, medications, problems, notes, messages, and tasks. They are built for episodic documentation and clinician-entered or clinician-reviewed data. Wearables produce patient-generated streams outside the visit, outside the exam room, and often outside a clear clinical question.
That mismatch explains why “send it to the chart” is rarely a sufficient requirement. If a patient’s wearable reports heart rate throughout the day, the receiving system still has to decide whether the data belongs in flowsheets, a remote monitoring dashboard, a media-like external document, a FHIR repository, an analytics environment, or a summarized note. Each destination creates a different expectation for review, liability, retention, and patient communication.
An AMA international physician survey found that fewer than 6% of physicians had integrated consumer wearable data into their practice.[6] That figure should not be inflated into a sweeping claim about physician resistance. It is better evidence of the practical constraint: wearing a device is easy; making its output reviewable inside clinical operations is not.
AI’s operational job is triage, not magic
Once normalized data exists, the next problem is volume. A pipeline that successfully maps every incoming sample to FHIR can still fail clinically if it produces a review burden no one can absorb. This is where AI middleware has a narrower and more useful role than the usual “find insights” language suggests.
The AI layer should reduce continuous telemetry into reviewable changes: a sustained deviation from a patient’s baseline, a threshold-crossing pattern, a trend that aligns with a monitored condition, or a summary that says what changed since the last review. Healthcare IT Today’s June 2026 workflow discussion emphasized this need for FHIR-native, AI-summarized integration, where clinicians receive distilled summaries of what changed and warrants attention rather than raw patient-generated streams.[5]

A useful AI triage layer is therefore conservative about what it surfaces. It does not ask a clinician to inspect every sleep stage interval or every heart rate fluctuation. It detects whether a selected metric moved outside a defined range, whether the change persisted long enough to matter, whether the device data is complete enough to support the signal, and whether the finding belongs in a dashboard, a queue, a message, or no clinician-facing surface at all.
The word “selected” matters. A program monitoring recovery after a cardiac procedure may care about resting heart rate trends, activity recovery, and symptom-linked changes. A sleep-focused program may care about duration, regularity, and patient-reported context. The middleware should not treat every available device metric as clinically equivalent just because an API exposes it.
For a hypothetical example, imagine a remote follow-up program that accepts wearable heart rate and activity data. The AI layer might suppress isolated spikes during exercise, ignore days with insufficient wear time, compare resting values against the patient’s own recent baseline, and surface only a sustained change paired with reduced activity. The point is not that this example proves a clinical rule. It shows the kind of filtering work that has to occur before anyone creates a task for a nurse or drops a signal into a cardiologist’s view.
A dashboard is still a clinical handoff
The last mile of the pipeline is not the API call into the EHR. It is the surface where a human sees the result. An EHR-adjacent dashboard, in-basket message, flowsheet summary, remote monitoring queue, or encounter note excerpt all carry different workflow consequences. If the output lands in a queue, someone owns that queue. If it lands in the chart, someone may assume it was reviewed. If it appears as a high-priority alert, someone has to interrupt other work to resolve it.
That is why alert filtering cannot be an afterthought. The integration team can make the pipe work and still damage the clinical workflow if every normalized value becomes a visible event. AI summarization should be evaluated not only by whether it detects patterns, but also by whether it reduces unnecessary review, explains why a signal appeared, and preserves enough provenance for a clinician to trust or dismiss it.
Privacy and responsibility do not follow the data automatically
Consumer wearable data also carries a governance problem that is easy to underplay in architecture diagrams. The device manufacturer may not be a HIPAA covered entity. Data can exist in consumer accounts, phone apps, and vendor clouds before it ever reaches a healthcare organization’s controlled environment. Once a covered entity ingests selected data for care, the obligations around that copy become clearer, but the upstream path may still sit partly outside the healthcare privacy model.
Middleware cannot solve that entire privacy gap, but it can make the handoff more governable. It can enforce consent status, log provenance, restrict which measures are ingested, separate raw payload storage from clinical summaries, and prevent every available consumer metric from entering the care environment by default. The goal is not to pretend consumer data becomes clean because it crossed a healthcare boundary. The goal is to make each crossing explicit.
What the complete pipeline has to do
A clinically survivable wearable integration pipeline has several jobs, and they do not happen in the EHR alone. The device and app ecosystem captures the signal. The ingestion layer authenticates access and receives data. The normalization layer turns brand-specific payloads into internally consistent concepts. The validation layer checks completeness, timing, units, and provenance. The FHIR mapping layer represents selected outputs as resources such as Observation and Patient. The AI layer filters, summarizes, and prioritizes. The clinician-facing layer presents the result where it can be reviewed without becoming a raw telemetry inbox.
- Ingestion answers: is this data allowed, current, and attributable to the right patient?
- Normalization answers: what does this device-specific payload mean in a shared clinical data model?
- Validation answers: is the value complete, timed correctly, and reliable enough to use?
- FHIR mapping answers: how should the selected value be represented for exchange and downstream use?
- AI triage answers: does this pattern warrant clinician attention, summary display, monitoring, or suppression?
- Workflow delivery answers: who sees the output, where, with what priority, and with what expectation of response?
The Garmin-to-FHIR prototype gives a concrete example of the middle of that path: selected wearable measures can be transformed into FHIR resources and placed in a FHIR server.[1] The broader architecture adds the uncomfortable production questions around multiple brands, inconsistent metric definitions, intermittent sync, privacy boundaries, and clinical review.
Wearable data reaches the EHR safely only after it has been authenticated, normalized, validated, mapped to FHIR, and filtered into summaries or signals that match a real clinical workflow. Without that middleware layer, the integration may still move data. It just moves the burden downstream to the clinician who has to decide what, if anything, the stream means.
References
- Garmin-to-FHIR prototype, Frontiers in Digital Health, October 2025, link
- AI Wearable EHR Integration, ROOK, link
- Integrate Wearable Data EHR, Intellivon, link
- State of Wearable Health Data, Sahha, June 2026, link
- Integrating Patient-Generated Data Into Clinical Workflows, Healthcare IT Today, June 4, 2026, link
- International Physician Survey of Consumer Wearables, American Medical Association, link
Comments
Join the discussion with an anonymous comment.