For a hospital, a better hurricane forecast is not better because a model score improved. It is better if it changes the hour when incident command opens, when transport contracts are activated, when dialysis patients are called, when oxygen vendors are checked, when blood supply is moved, and when county health officials decide whether a protective action zone is too wide or too narrow.
That is the practical meaning of recent AI improvements to NHC disturbance forecasts for health safety. The strongest evidence is not yet a peer-reviewed chain from a named AI model to fewer deaths or fewer storm injuries. It is a set of measurable forecast gains that matter to health operations: earlier identification of tropical disturbances, longer useful lead time for track forecasts, closer predicted tracks, deeper probabilistic ensembles, and faster model runs. Those gains make health safety benefits strongly plausible, but they should not be described as proven mortality reductions.

The Decision Window Starts Before There Is a Hurricane
The word "disturbance" matters. A mature hurricane forecast helps decide what to do with a named storm. A disturbance forecast helps decide when the quiet planning period is over. That is a different problem for hospitals, because the first commitments often happen before the threat is administratively obvious to everyone in the system.
The National Hurricane Center has described AI as part of its hurricane forecasting work, while also emphasizing that human forecasters still interpret model output and issue official forecasts and warnings [1]. That division of labor is important. An AI model can add signal earlier or run many scenarios faster; it does not call an ambulance contractor, cancel elective procedures, or decide whether a medically fragile patient should be moved before roads degrade.
At the disturbance stage, the most directly relevant tool in the current evidence base is the University of Miami Rosenstiel School's AI wave tracker. The system became operational at NHC in 2025, uses a convolutional neural network, and was trained on 40 years of reanalysis data from 1981 through 2023 to detect tropical easterly waves before cyclone formation [2]. That does not mean every wave becomes a hospital threat. It means one part of the pre-cyclone watch floor is more automated and potentially more consistent.
For health agencies, that earlier disturbance signal is useful only if it is treated as a trigger for readiness, not as a trigger for overreaction. It can justify checking generator fuel, confirming evacuation vendors, reviewing high-risk patient lists, and asking long-term care partners whether staffing plans are still realistic. It should not by itself empty a hospital or widen a county evacuation zone.
What the AI Gains Actually Measure
Most of the best public evidence for AI forecast improvement concerns tropical cyclone track and intensity forecasting after a system has formed, not the earliest disturbance stage. That distinction prevents a common overclaim. The disturbance tools can help detect and monitor precursor waves; the larger quantified gains come from AI models that forecast the behavior of tropical cyclones and hurricanes once there is a storm to track.
| Forecast improvement | Reported performance | Health planning consequence |
|---|---|---|
| Earlier useful track guidance | Google DeepMind reported that its 5-day track prediction matched the European ensemble system's 3.5-day performance. | A hospital may gain planning time before evacuation, staffing, and supply decisions become compressed. |
| Closer medium-range tracks | Google DeepMind reported an average 5-day track error about 140 km closer than the physics-based ENS comparison. | Counties can be more careful about which facilities and zones enter the highest-cost response posture. |
| Larger probabilistic ensembles | NOAA and Google described AI-GEFS as producing 1,000-member ensembles. | Emergency managers can compare probabilities instead of treating one track line as the plan. |
| Faster model production | NOAA and Google described AI-GEFS as extending useful skill by 18-24 hours while using 0.3% of computing resources, with runs around 40 minutes rather than hours on supercomputers. | Forecasters and health officials can refresh uncertainty estimates faster during the period when decisions are still reversible. |
Google DeepMind has reported two numbers that are especially relevant to health planning: a 1.5-day lead-time gain at the 5-day range, and an average 5-day track prediction about 140 km closer than a physics-based ensemble comparison [3]. These are model-performance figures, not hospital outcome figures. Still, they point to the kind of delta that matters: more time before landfall and less geographic uncertainty around who is likely to be in the impact corridor.
NOAA and Google have also described AI-GEFS as a 1,000-member probabilistic ensemble system with 18-24 hours of extended useful skill, using 0.3% of the computing resources and producing output in about 40 minutes rather than hours on supercomputers [4]. The value is not just speed for its own sake. In a hospital emergency operations center, a faster ensemble can mean one more meaningful update before a noon executive briefing, a county call, or the moment when an evacuation decision becomes practically irreversible.
Public summaries of the NHC 2025 verification discussion reported that Google DeepMind's GDMI slightly outperformed NHC's official forecast at short ranges for both track and intensity [5]. That is notable, but it should be held carefully. Official forecasts are not raw model contests; they include human synthesis, consistency, communication judgment, and knowledge of hazards the model may not represent well.
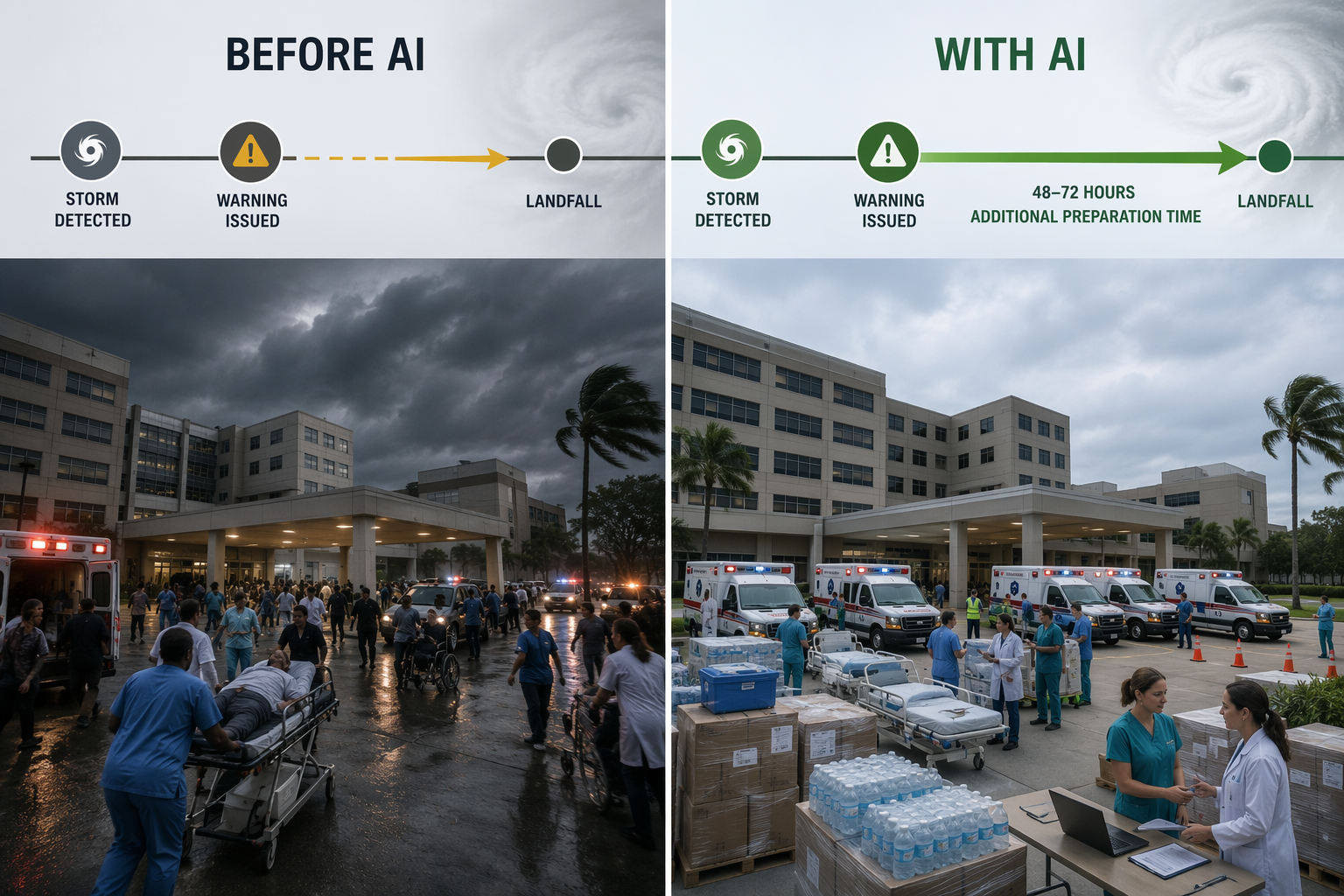
Lead Time Is Only Valuable If Someone Can Use It
Hospital evacuation is not a switch. It is a sequence of constraints. Ambulances and buses may be shared across counties. Receiving facilities need bed availability and staffing. Pharmacy, lab, blood bank, oxygen, dialysis, and medical records workflows have to move with patients. Some patients can leave early; some deteriorate if moved unnecessarily; some cannot be moved safely once winds, flooding, or road closures begin.
A 1.5-day improvement at the 5-day range therefore matters most in the 48-72 hour operational window. That is when a hospital can still stage resources without yet executing the most disruptive steps. If the threat sharpens, the facility has not lost a day. If the threat shifts away, leadership may avoid a full evacuation posture that would have been expensive, risky, and hard to unwind.
The gain is not simply "more warning." More warning can create noise if it arrives as a single alarming line on a map. The more useful version is earlier warning paired with probability: how many plausible tracks bring hurricane-force winds near the facility, how quickly that probability is changing, and whether the risk is concentrated enough to justify moving patients before the county-wide response peaks.
That is where large ensembles change the conversation. A 1,000-member system can support a more explicit discussion of uncertainty than a small set of deterministic tracks. A hospital does not need a false promise that the model knows the future. It needs to know whether it is planning for a low-probability extreme, a rising central scenario, or a broad cone that still justifies conservative preparations.
Track Precision Can Reduce the Wrong Kind of Evacuation
Health safety is not maximized by moving the largest possible number of patients. Unnecessary evacuation has its own clinical risks: medication disruption, transport delays, falls, missed dialysis, staff fatigue, family separation, and receiving-facility crowding. A forecast that narrows the likely impact corridor can help officials protect the facilities that truly need early action without pushing every nearby hospital into the same posture.
The reported 140 km improvement in 5-day track error is not small in that context [3]. At the scale of a coastline, 140 km can separate one hospital referral region from another, or change which inland shelters, dialysis centers, oxygen suppliers, and EMS staging areas sit inside the most likely wind corridor. It does not eliminate the need for surge, rainfall, and access-route planning, but it can reduce the number of places forced to plan as if the worst track is the central track.
County health officers feel this difference quickly. A broader warning footprint can mean more hospitals asking for transport support, more nursing homes requesting evacuation assistance, more medically vulnerable residents entering call lists, and more competition for fuel and generators. A narrower, better-supported risk area can preserve capacity for the places most likely to need it.
There is economic evidence for the value of forecast improvement, though not AI-specific health-outcome proof. An NBER Digest summary of Molina and Rudik's Working Paper 32548 reported that improvements in hurricane forecasts from 2007 through 2020 reduced costs by about $5 billion per hurricane, a 19% reduction, and that a one-standard-deviation improvement in wind-speed accuracy reduced county-level spending by about $30 million per county per hurricane [6]. The same evidence is useful for understanding avoidable spending and over-response; it should not be converted into a claim that AI models have already prevented a quantified number of deaths.
The Disturbance Stage Changes the First Call, Not the Final Order
The University of Miami wave tracker is important because it reaches into the period before a storm has a name. It can help forecasters and planners notice tropical easterly waves earlier and more systematically [2]. For a health system, that can shift the first call from "we will wait until formation" to "we will quietly verify readiness while uncertainty is still high."
That distinction keeps the response proportional. At the disturbance stage, the sensible actions are low-regret: check contact trees, review generator maintenance status, confirm fuel contracts, identify patients who would be hard to move, and ask supply chain teams whether deliveries are vulnerable later in the week. The decision is not yet to move patients. It is to stop pretending the calendar is normal.
As the system develops, the AI track and ensemble tools become more relevant. If probabilities consolidate near the hospital's service area, the earlier readiness work turns into faster execution. If probabilities shift away, the hospital has spent staff attention on readiness checks rather than on a full, disruptive evacuation that may not have been necessary.
Hurricane Melissa Shows the Operational Promise, Not the Whole Proof
Hurricane Melissa is a useful illustration of what earlier AI-supported guidance can mean. Reporting in 2026 described the 2025 Category 5 storm as being predicted more than three days ahead, with DeepMind partly credited and Jamaican and Florida health systems receiving preparation time that was described as unheard of only a few years earlier [7].
As a case, Melissa helps make the planning issue concrete. Three or more days can change whether a hospital is still bargaining for transportation or already sequencing patient movement. It can change whether dialysis schedules are shifted before roads clog. It can change whether oxygen-dependent residents are identified while call centers still have staff.
But one storm does not establish a general health outcome effect. A stronger forecast can be underused by institutions with weak plans. A weaker forecast can still lead to good outcomes if officials act conservatively and communicate clearly. The case supports plausibility; it is not a substitute for systematic morbidity and mortality research.
Where Human Forecasters Still Carry the Safety Burden
The most dangerous way to use these tools is to treat model confidence as operational certainty. AI models can produce impressive track guidance while still giving limited visibility into the physical reasoning behind a forecast. NHC has described AI systems as tools that forecasters evaluate rather than replacements for the official forecast process [1].
That matters because hospital safety depends on hazards beyond the center track. Freshwater flooding, rainfall distribution, storm surge, tornadoes, power failure, road access, and post-storm heat all shape patient risk. A model that improves track timing may still be insufficient for deciding whether a hospital can shelter in place safely behind a flooded access road.
Intensity is another caution. The research base includes strong claims for some AI systems, but it also notes that the ECMWF AIFS showed no skill for intensity forecasting. For a hospital, intensity is not an academic detail. It affects generator duration assumptions, window and roof risk, ambulance movement, staffing lock-in, and whether a partial evacuation remains defensible.
Out-of-distribution extremes are the final planning problem. Hospitals do not get to plan only for storms that resemble the training record. A rare intensification pattern, an unusual rainfall setup, or a compound disaster can make the average model gain less useful at the moment when consequences are largest. Conservative planning remains necessary even when the forecast suite looks sharper than it did a decade ago.
What Health Systems Can Reasonably Take From the Evidence
The evidence supports a practical, bounded conclusion. AI is making NHC disturbance and hurricane forecasting more actionable for health systems by improving early disturbance detection, extending useful lead time, sharpening track guidance, expanding probabilistic ensembles, and reducing compute time. Those changes can help hospitals start readiness work earlier, avoid some unnecessary zone expansion, and preposition scarce resources with a clearer view of uncertainty.
The evidence does not yet support a stronger claim that these AI improvements have directly reduced hurricane morbidity or mortality in a measured, peer-reviewed way. That study still needs to be done, and it will need to separate forecast quality from emergency management capacity, public compliance, hospital infrastructure, social vulnerability, and the specific hazards each storm produced.
The useful standard is therefore operational. Did the forecast identify the risk early enough for a hospital to act before the transportation market collapsed? Did it narrow the likely impact area enough to avoid moving patients who could safely stay? Did the ensemble show uncertainty clearly enough for county officials to stage resources without pretending the answer was fixed? That is where AI improvements to NHC disturbance forecasts can matter for health safety now.
References
- AI in Hurricane Forecasting at the National Hurricane Center: A Q&A with NHC Science Operation Officer Wallace Hogsett - weather.gov
- New AI tool tracks early signs of hurricane formation - University of Miami Rosenstiel School, Aug 2025
- How we're supporting better tropical cyclone prediction with AI - Google DeepMind blog
- NOAA and Google team up to advance the use of AI hurricane and tropical weather forecast models - NOAA
- The future of forecasting: AI emerges as top hurricane model in 2025 - ClickOrlando, March 2026
- The Value of Improving Hurricane Forecasts - NBER Digest, Working Paper 32548
- Google AI is a hurricane genius and is here to stay - Palm Beach Post, June 2026
Comments
Join the discussion with an anonymous comment.