The useful question for AI in orthopedic surgery recovery prediction is not whether a model can produce an impressive score. It is whether software can identify, early enough to matter, the patient who is likely to stay longer than expected, recover function more slowly, need closer monitoring, or miss a rehabilitation milestone after an operation. In the published literature, those are related but not interchangeable targets. A model that predicts prolonged length of stay is working with a cleaner endpoint than one that tries to forecast pain, gait, adherence, or a one-year functional score.
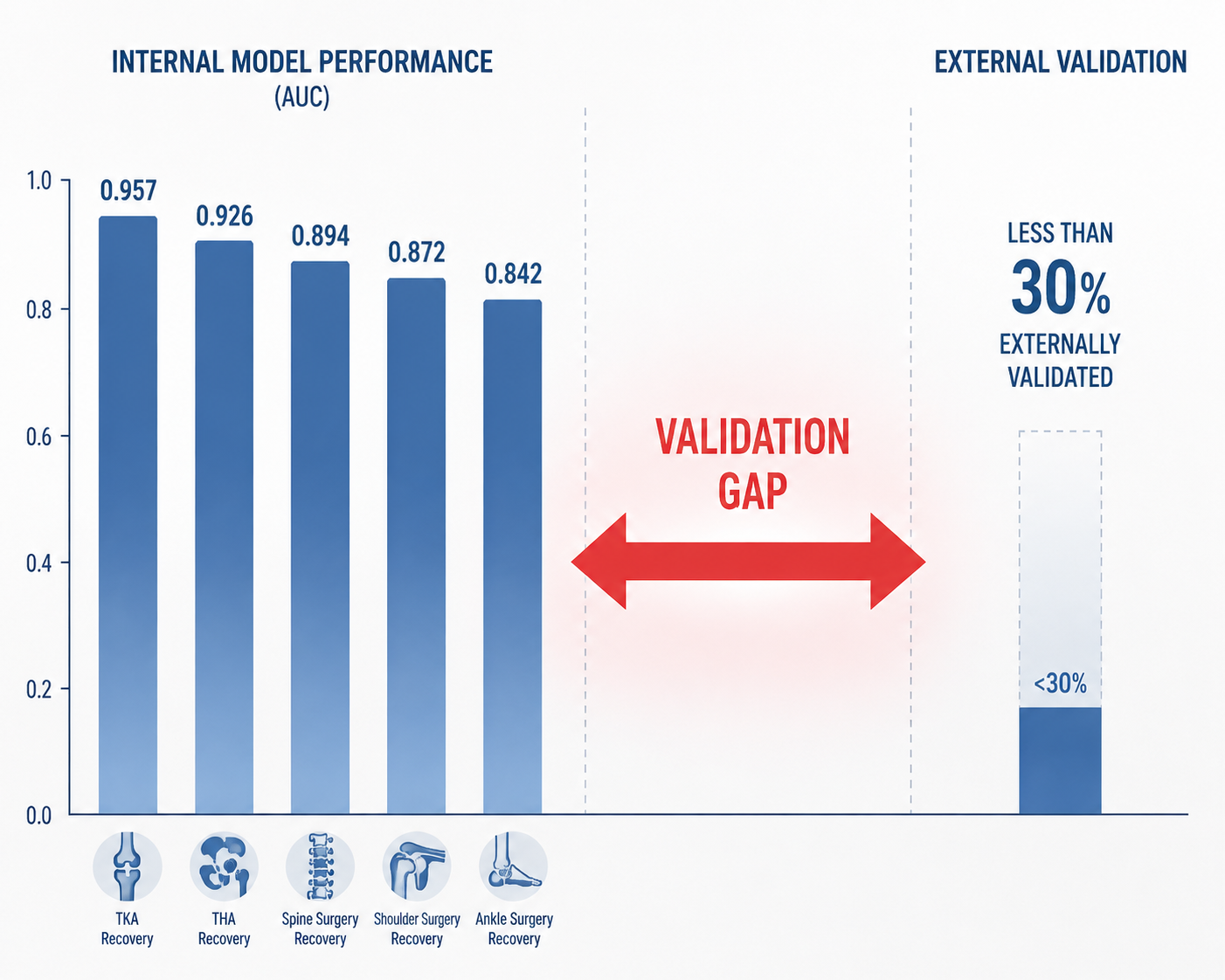
That distinction matters because the headline results can look stronger than the evidence base underneath them. Across the studies available here, reported discrimination reaches from an AUC of 0.842 in knee arthroplasty transfusion prediction to 0.957 in a small hip fracture recovery study. But in arthroplasty AI models, a 2023 systematic review found that fewer than 30% had undergone external validation, and only 9 of 30 machine-learning studies outperformed traditional logistic regression.[1] Those two facts sit uncomfortably close together: high internal performance, limited transportability.

What Counts as Recovery Prediction?
Orthopedic recovery is a sequence of clinical and operational events, not a single endpoint. A hospital may care first about length of stay, discharge destination, transfusion, complications, or readmission. A surgeon may care about pain, mobility, implant-related complications, and whether the patient is tracking toward the expected functional result. A rehabilitation team may care about gait recovery, adherence, walking speed, or the ability to progress exercises safely.
Those outcomes do not have the same evidence burden. Predicting transfusion from preoperative variables, for example, is closer to perioperative risk stratification than to recovery in the patient-centered sense. Predicting prolonged length of stay is recovery-adjacent and operationally important, but it does not prove that a model can forecast pain relief or independent mobility. Predicting one-year function after hip fracture repair moves closer to the patient’s lived recovery, but the measurement is harder, follow-up is more fragile, and rehabilitation behavior becomes part of the signal.
The strongest way to read this literature is therefore by asking four questions at once: what outcome was predicted, in which procedure population, with what validation, and compared with what simpler baseline. A model can be scientifically interesting and still not be ready to drive discharge planning, rehab intensity, remote monitoring, or care-management staffing.
The Best Current Example: Prolonged Length of Stay
Rezvani et al.’s 2026 npj Health Systems study is the most substantial recovery-adjacent model in this set because it starts with scale, reports calibration, and uses a national surgical data source rather than a small local cohort. The authors trained an Optuna-optimized XGBoost model to predict prolonged length of stay after orthopedic surgery using 212,812 NSQIP cases and 65 features, reporting an AUC of 0.853 on a hold-out test set.[2]
Length of stay is not the same as functional recovery, but it is a consequential recovery-adjacent endpoint. It affects bed capacity, discharge timing, care coordination, and the patient’s transition into home health, inpatient rehab, skilled nursing, or routine outpatient follow-up. It is also an endpoint clinicians can act on before the patient has fully declared their postoperative course.
The model’s methodological details make the result more informative than a bare AUC. The study reported a Brier score of 0.1092, indicating well-calibrated probability estimates, and used SHAP analysis to identify case type, ASA class, anesthesia type, and preoperative hematocrit as key drivers.[2] Calibration is not a decorative statistic in this setting. A poorly calibrated model can rank patients correctly but still overstate or understate absolute risk, which is exactly where discharge planners and perioperative teams can be misled.
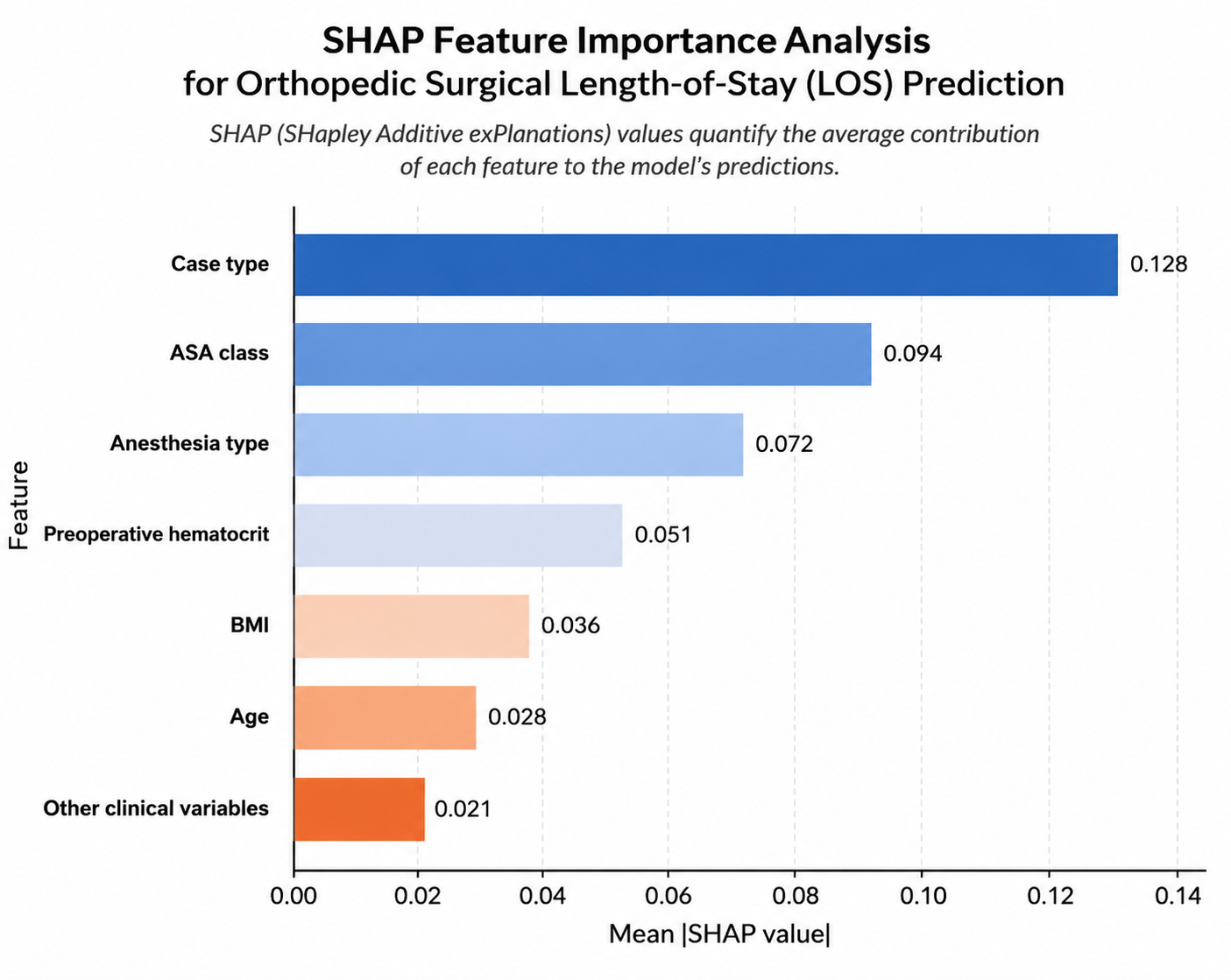
The feature pattern is also clinically plausible. Case type and ASA class carry information about operative burden and baseline medical risk. Anesthesia type and preoperative hematocrit connect the model to perioperative management and physiologic reserve. None of that proves causality, and SHAP values do not turn a prediction model into a mechanistic explanation. But they do make it easier for a clinical team to inspect whether the model is learning signals that belong in the orthopedic perioperative workflow rather than opaque artifacts of documentation.
The remaining caution is timing. The study was published on July 1, 2026, and the research brief does not identify independent replication yet.[2] A large national derivation source and hold-out testing are meaningful strengths; they are not the same as prospective testing across hospitals that differ in case mix, discharge norms, staffing, payer constraints, and post-acute care availability.
Function and Mobility Are Harder Targets
Hip and knee arthroplasty dominate the more operationally mature part of orthopedic AI, but functional recovery remains more difficult to predict than hospital utilization. Functional outcome is shaped by preoperative disability, pain expectations, surgical factors, rehab access, motivation, complications, social support, and measurement choice. A model can perform well on a selected dataset and still fail when the recovery pathway changes.
Stetter et al. show a useful direction for this problem rather than a finished clinical tool. In a 2025 Arthritis Research & Therapy study, researchers analyzed gait biomechanics in 109 hip osteoarthritis participants, including 63 postoperative patients and 56 controls, and identified three distinct recovery trajectory groups.[3] The immediate value is conceptual: recovery after hip arthroplasty may be better understood as a set of trajectories than as a single pass-fail endpoint.
That kind of clustering could eventually help rehabilitation teams decide who needs standard progression, closer gait-focused therapy, or a different follow-up cadence. But the study size is moderate, and the research brief identifies external validation as still needed.[3] Without validation in other centers and care pathways, the groups should be treated as a recovery-pattern signal, not as a transferable classification system.
Hip fracture repair adds another layer of complexity because the patients are often older, frailer, and more exposed to delirium, deconditioning, caregiver limitations, and rehabilitation access problems. Lin et al. reported a random forest model predicting one-year functional recovery after hip fracture surgery with an internal-validation AUC of 0.957, and postoperative rehabilitation compliance was the strongest predictor.[4]
That result is promising, but it should not set the emotional temperature for the field. The study included only 77 patients from a single Chinese hospital, used a telephone-administered Harris Hip Score modified to a 91-point scale, and had no external validation.[4] Rehabilitation compliance being the strongest predictor is clinically believable, but it also raises a practical deployment issue: if the most important signal is known only after surgery and depends on patient behavior, the model may be better suited to dynamic follow-up than to preoperative counseling alone.
Spine Surgery and Wearables: Interesting, Earlier-Stage Evidence
The spine surgery evidence in this research set is thinner and more exploratory. Washington University described a machine-learning method using Fitbit wearable data to better predict spine surgery outcomes.[5] Wearable data are appealing because recovery after spine surgery often unfolds outside the clinic: walking tolerance, sleep, activity recovery, and pain-related avoidance may change before a scheduled visit captures them.
But wearable prediction has its own transportability problems. Device adherence is not random. Patients who wear and sync devices consistently may differ from those who do not. Activity measures can reflect surgical recovery, but they can also reflect weather, work demands, caregiving, neighborhood walkability, baseline fitness, or pain medication effects. A spine recovery model built from wearable streams may be clinically useful eventually, especially for remote monitoring, but the evidence described here does not support treating it as a mature deployment category.
Why External Validation Changes the Interpretation
The central limitation in orthopedic recovery prediction is not that the models are weak. Many are not. The problem is that internal validation often answers a narrower question than clinicians need answered. It asks whether the model performs on data held back from the same broad context. It does not necessarily ask whether the model survives a different institution, a different surgeon mix, a different discharge culture, a different rehabilitation network, or a different documentation pattern.
Karlin et al.’s systematic review is therefore more than a methodological footnote. In arthroplasty AI studies, fewer than 30% of published models had external validation, and only 9 of 30 machine-learning studies outperformed logistic regression.[1] A model that does not beat a simpler baseline may still be useful if it is easier to integrate, better calibrated, or more interpretable for a particular workflow. But algorithmic novelty by itself is not evidence of clinical advantage.
The logistic-regression comparison is especially important because orthopedic service lines already use risk factors informally and sometimes formally: age, comorbidity, anemia, ASA class, procedure type, prior function, and social support all influence planning. A machine-learning model must either improve prediction enough to justify added complexity or make an existing risk estimate more usable at the point of care.
| Evidence Question | Why It Matters Clinically |
|---|---|
| Was the model externally validated? | Shows whether performance may transfer beyond the derivation setting. |
| Was calibration reported? | Determines whether predicted probabilities can support planning rather than only ranking. |
| Did it outperform logistic regression or another simple baseline? | Tests whether model complexity adds value. |
| Is the outcome actionable before the decision point? | Prevents models from predicting events too late to change care. |
| Is the workflow defined? | Connects prediction to discharge planning, rehab escalation, monitoring, or follow-up. |
This is where reported AUCs can become misleading if read too quickly. An AUC of 0.957 in 77 patients is not equivalent to an AUC of 0.853 in more than 200,000 surgical cases. The smaller result may identify a meaningful signal, but its uncertainty and portability are different. Likewise, a model trained on a national surgical registry may generalize better across case types, yet still need prospective evaluation before it is allowed to influence staffing, post-acute referrals, or patient messaging.
Prediction Becomes More Useful When It Is Tied to an Intervention
The gap between prediction and improved recovery is not philosophical. It is operational. If a model identifies a patient at high risk for slow recovery, someone has to decide what changes: earlier physical therapy contact, different discharge destination planning, remote monitoring, anemia optimization, closer nurse outreach, transportation support, or a lower threshold for clinic review.
Mehta et al.’s randomized trial is relevant because it moves closer to that intervention context. In a JAMA Network Open study of 242 hip and knee replacement patients, AI-supported remote monitoring was associated with a significant rehospitalization reduction compared with standard care.[6] The trial does not settle every question about recovery prediction models, but it demonstrates the kind of bridge the field needs: software-generated risk or monitoring signals embedded in a care pathway where clinicians can respond.
Commercial translation is also beginning to appear. Zimmer Biomet’s WalkAI has been described as an FDA-cleared AI tool that generates daily 90-day walking speed forecasts after hip or knee replacement.[7] That is directionally important because walking speed is closer to functional recovery than a hospital billing or utilization endpoint. Still, without confirmed FDA clearance identifiers from primary FDA databases in the materials reviewed here, regulatory claims should remain qualified and tied to the published description rather than expanded.
The more clinically mature version of this field will not be a dashboard that simply labels patients as high risk. It will be a workflow in which the predicted risk appears early enough, is calibrated well enough, and points to an action that someone is accountable for taking. Orthopedic recovery involves surgeons, inpatient nurses, physical therapists, case managers, outpatient rehab teams, caregivers, and patients. A prediction that does not change any handoff is mostly a research result.
What the Evidence Supports Now
The evidence is strongest in hip and knee arthroplasty and in recovery-adjacent outcomes such as length of stay, transfusion, rehospitalization, and monitored postoperative function. It is thinner for spine surgery and hip fracture repair, where datasets are smaller, recovery pathways are more heterogeneous, and functional outcomes are harder to standardize.
Rezvani et al. show what a stronger orthopedic prediction study can look like: large sample size, national surgical data, modern model optimization, hold-out testing, calibration reporting, and interpretable feature analysis.[2] Stetter et al. and Lin et al. show why the recovery question remains attractive: models and clustering methods may identify different functional trajectories, not merely perioperative complications.[3][4] Karlin et al. show why the field cannot grade itself by internal AUC alone.[1]
AI models for orthopedic surgical recovery prediction are scientifically promising and increasingly relevant to clinical operations, especially in arthroplasty and length-of-stay prediction. Their clinical readiness remains lower than headline performance implies until external validation, baseline superiority, calibration, and intervention-linked deployment are demonstrated consistently.
References
- Can Artificial Intelligence Predict Outcomes in Total Joint Arthroplasty? A Systematic Review. The Journal of Arthroplasty, 2023.
- Machine learning prediction of prolonged length of stay following orthopedic surgery. npj Health Systems, July 1, 2026.
- Identifying distinct recovery trajectories after total hip arthroplasty using gait biomechanics. Arthritis Research & Therapy, 2025.
- Prediction of functional recovery one year after hip fracture surgery using machine learning. Frontiers in Surgery, 2023.
- New machine learning method can better predict spine surgery outcomes. Washington University School of Medicine.
- Effect of Remote Monitoring on Discharge to Home, Return to Activity, and Rehospitalization After Hip and Knee Arthroplasty. JAMA Network Open, 2020.
- Zimmer Biomet steps up surgical tech with first AI-powered software tool. Fierce Biotech.
Comments
Join the discussion with an anonymous comment.