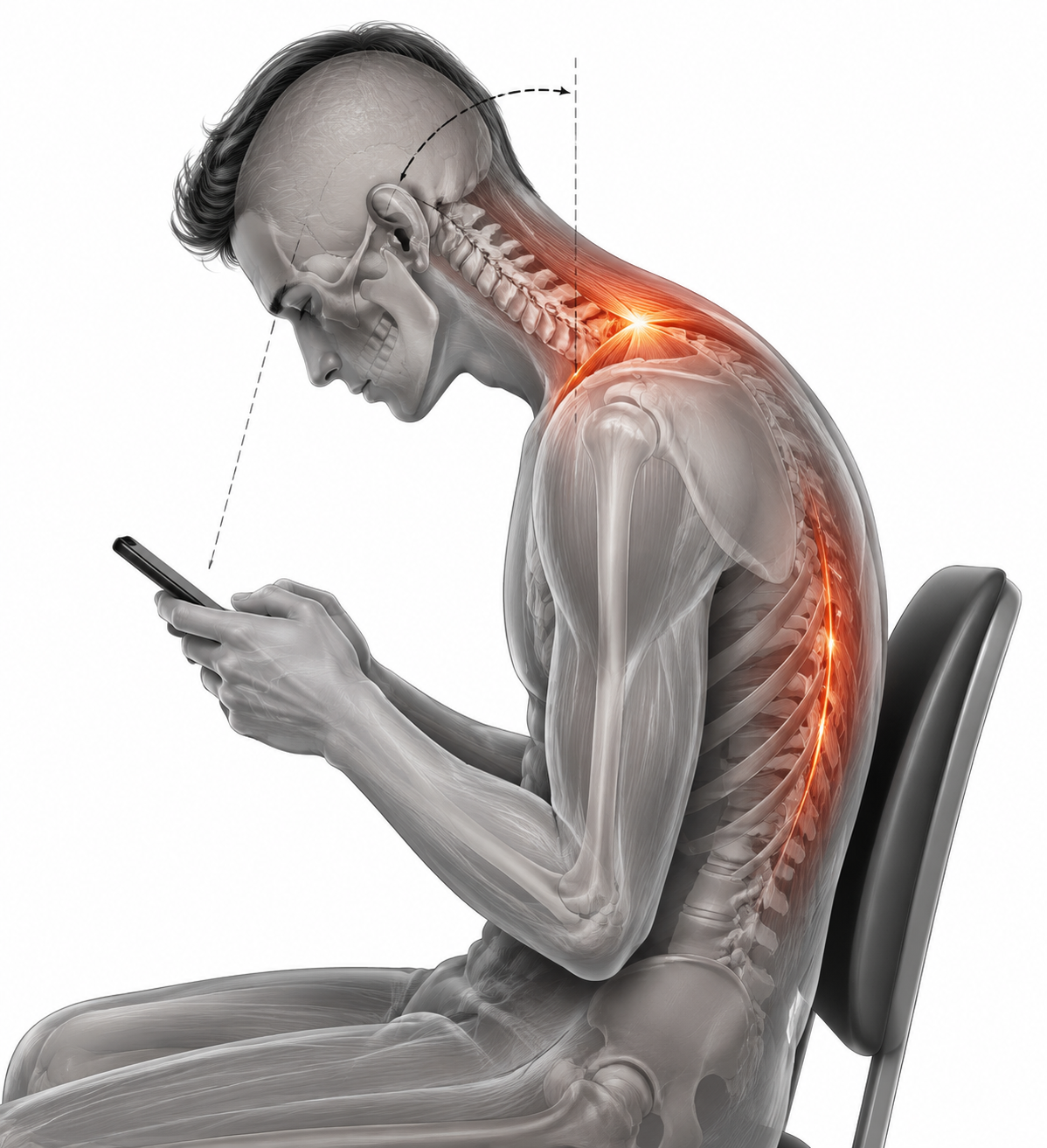
The clinically interesting moment in smartphone-related repetitive strain injury is often quiet: the head drops, the neck shifts forward, the shoulders accept a little more load, and the hands keep working. Nothing dramatic has happened yet. But the position is repeatable, and repeatable loading is exactly where many neck, shoulder, and forearm complaints begin to gather momentum.
That is why the practical question around AI in treating smartphone-related repetitive strain injury should start with posture rather than with software. A systematic review by Eitivipart et al. found that smartphone use was associated with increased head tilt angle, forward head shift, and increased upper trapezius and erector spinae muscle activity across 12 moderate-quality biomechanical studies.[1] Those findings do not prove that every slouched phone session becomes RSI, but they identify plausible precursors that a preventive system would need to recognize.
The next question is whether a phone can see those precursors quickly enough to intervene while the posture is still happening. Heo et al. reported an on-device MediaPipe BlazePose system using 33 three-dimensional landmarks, with 97.2% keypoint accuracy and 28.6 ms inference time on consumer smartphones.[2] In the same prospective single-arm quasi-experimental study, the system achieved 95.8% pose classification accuracy compared with physiotherapist assessment, with an intraclass correlation coefficient of 0.94.[2]
Those are not decorative performance numbers. For posture correction, delay changes the clinical value of the feedback. A cue that arrives after the user has already shifted, locked the screen, or changed tasks is mostly a reminder. A cue that arrives while the head is drifting forward can become part of the motor task itself.
What the AI has to notice
Smartphone RSI is an imprecise everyday label, and it is worth keeping it imprecise rather than pretending it maps neatly onto one diagnosis. The complaints may appear in the neck, upper trapezius region, shoulder girdle, elbow, forearm, wrist, or thumb. The common thread is not a single tissue failure. It is sustained or repeated loading in positions that the body can tolerate for a while, until volume and recovery stop balancing each other.
For an AI posture tool, the most defensible targets are therefore not pain scores or diagnostic labels at first. They are observable postural features: head tilt, forward head translation, shoulder position, upper trunk alignment, and the relation among head, neck, shoulders, elbows, and hands. The Eitivipart review supports that focus because the measurable changes during smartphone use were in head and neck posture and cervical muscle activity, not in a confirmed downstream RSI diagnosis.[1]

That distinction matters. Detecting a forward head posture is not the same as treating a tendon disorder, cervical radiculopathy, nonspecific neck pain, or work-related upper limb disorder. It is an attempt to catch the mechanical setup that may contribute to symptoms before the person arrives in clinic describing vague tightness, fatigue, or aching that has been accumulating for weeks.
| Clinical feature | Why it matters | What pose estimation can plausibly track |
|---|---|---|
| Increased head tilt | Associated with smartphone use in moderate-quality biomechanical evidence | Relative head, neck, and trunk landmark angles |
| Forward head shift | Changes the load relationship through the cervical and upper thoracic region | Head position relative to shoulder and torso landmarks |
| Upper shoulder loading pattern | Smartphone use was associated with increased upper trapezius activity | Shoulder elevation and upper body posture as indirect visual markers |
| Sustained position | Duration and repetition may turn a tolerable position into a clinical complaint | Time spent outside predefined posture thresholds |
The last row is easy to underappreciate. A single image of a flexed neck rarely tells the whole story. The more useful signal is persistence: how often the posture appears, how long it is held, whether correction happens spontaneously, and whether the user returns to the same position within seconds. Computer vision is well suited to that kind of repeated observation, provided the camera view is usable and the model performs consistently across real settings.
Why on-device speed changes the intervention
A posture model that depends on remote processing may still be impressive, but it is less attractive for this use case. The phone is expected to operate in bedrooms, offices, buses, waiting rooms, gyms, and clinics. Sending posture video away from the device introduces privacy concerns and potential latency at exactly the points where the tool needs trust and timing.
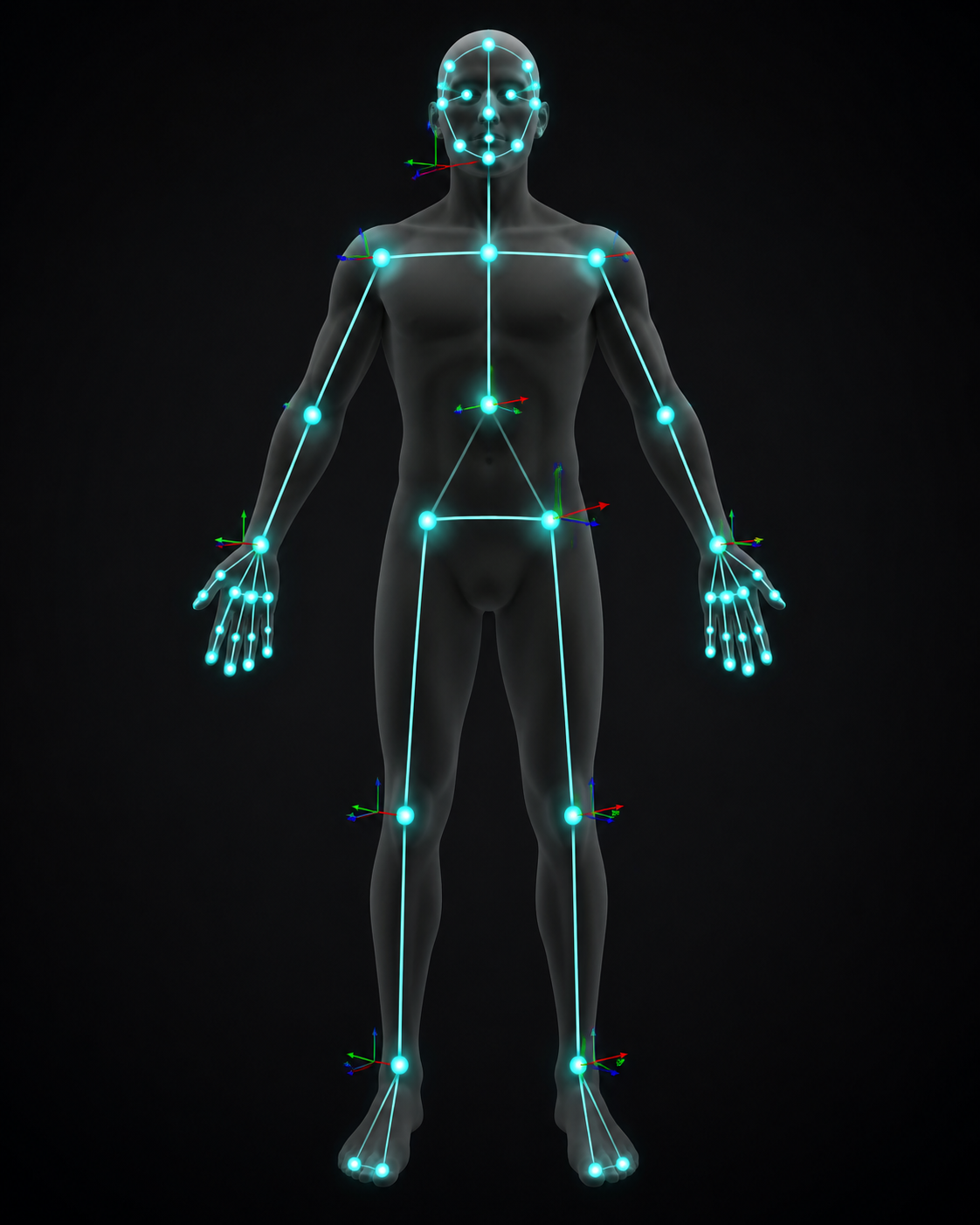
Heo et al.’s use of MediaPipe BlazePose is relevant here because the reported 33 three-dimensional landmarks allow the system to estimate whole-body joint relationships rather than only a rough face or shoulder box.[2] For smartphone posture, that means the system can look at the head, neck, shoulders, elbows, wrists, trunk, and their spatial relationships. It still cannot see muscle activation directly. It can, however, detect visible postural arrangements that have been linked to increased activity in the cervical and upper shoulder musculature.[1][2]
The reported 28.6 ms inference time is also clinically meaningful.[2] Real-time biofeedback depends on a short loop: detect the posture, decide whether it crosses a threshold, prompt the user, and allow an immediate correction. If that loop is smooth, the feedback can arrive as the person is still holding the phone, not after the session has ended.
On-device processing also makes the intervention more plausible in routine environments. The camera data do not need to leave the phone for posture estimation, and the system can operate without an internet connection. That does not solve every privacy issue; users still need to know when the camera is active, how data are stored, and whether any logs are shared. But local inference removes one major barrier for a tool that is meant to observe ordinary body positions in ordinary private spaces.
Feedback has to be timely, tolerable, and specific
The case for AI posture correction is not that the phone knows more than a clinician. It is that the phone may be present during the hundreds of small repetitions the clinician never sees. A patient can demonstrate excellent posture in an appointment and still return to a sustained forward-head position during commuting, messaging, gaming, or late-night reading.
Köroglu et al. describe real-time multimodal biofeedback in postural management, including visual, auditory, and haptic cues, and connect these feedback loops with motor learning mechanisms.[3] That source is a critical narrative review rather than a systematic review, so it should be used as a framework for plausible clinical design, not as proof that any particular smartphone RSI intervention prevents injury.
The feedback itself should not behave like a generic wellness notification. A useful cue is tied to a correctable observation: the head has moved beyond a threshold, the shoulders have elevated, the phone has been held low for a sustained interval, or the user has returned to the same position repeatedly. The cue can then ask for one specific adjustment: raise the phone, bring the head back over the trunk, relax the shoulders, or take a brief movement break.
- Visual feedback can show a simple alignment overlay or color change when head and shoulder position moves outside a target range.
- Auditory feedback can work when the user is not looking at a correction screen, but it risks becoming socially intrusive.
- Haptic feedback can provide a private cue, though vibration fatigue is a real design concern.
- Session summaries can help clinicians and users review patterns, but they should not replace in-the-moment correction.
A hypothetical example makes the feedback loop clearer. A user begins reading on a phone with the device low in the lap. The model detects a sustained increase in head tilt and a forward head position relative to the shoulders. After a short threshold period, the phone vibrates once and displays a small cue to raise the device and bring the head back. If the user corrects, the cue disappears. If the same pattern returns repeatedly, the system may suggest a break or a different setup.
Nothing in that example requires the software to diagnose RSI. It requires the software to identify a visible, repeated, biomechanically relevant posture and deliver a cue that the user can act on immediately. That narrower job is where the current evidence is strongest.
Where the evidence is still thin
The largest gap is not computer vision performance. It is clinical outcome evidence. The available materials support a chain of plausibility: smartphone use is associated with certain postural and muscle activity changes; on-device pose estimation can detect body landmarks quickly and accurately; real-time feedback may support posture correction. The chain does not yet establish that AI-guided posture correction prevents or treats clinically diagnosed smartphone-related RSI.
No study in the supplied evidence specifically enrolled patients clinically diagnosed with smartphone-related RSI as the primary population. The Eitivipart review analyzed biomechanical studies of smartphone use, and all 12 included studies were rated moderate quality.[1] That is enough to justify concern about head and neck loading patterns. It is not enough to quantify RSI risk reduction from changing those patterns.
Heo et al. is also not a prevention trial for smartphone RSI. It was a prospective single-arm quasi-experimental validation study with 146 completers, a mean age of about 23.8 years, and a cohort that was 69.2% male.[2] Those details limit generalizability. Young adults may interact with phones differently than older adults, office workers with chronic symptoms, people with prior neck injury, or patients already diagnosed with upper-limb overuse conditions.
The lack of a control group matters as well. Without randomization or comparison against usual ergonomic advice, clinician-guided exercise, passive reminders, or no intervention, it is difficult to separate the effect of AI feedback from attention, novelty, motivation, or the user’s awareness of being monitored. A system can classify posture well and still fail to change symptoms durably.
Long-term evidence is also missing. The research brief identifies no efficacy data beyond 16 weeks for AI-guided postural correction in RSI prevention. That matters because repetitive strain problems are not usually solved by a few good corrections in one session. The clinical question is whether users tolerate the feedback over time, whether corrections persist when prompts are reduced, and whether symptom incidence, severity, function, or care-seeking changes in a meaningful way.
What a stronger clinical study would need to measure
A better trial would start by enrolling the right population. That could include people with early neck, shoulder, forearm, wrist, or thumb symptoms associated with heavy smartphone use, or a higher-risk group with defined exposure patterns. The diagnosis and inclusion criteria would need to be explicit, because “smartphone RSI” is too broad to carry the clinical endpoint by itself.
The comparator would also matter. AI biofeedback should not be tested only against nothing. Clinicians need to know whether it outperforms standard ergonomic education, scheduled break reminders, exercise instruction, or simple non-AI posture prompts. If the AI system’s main advantage is timing and specificity, the study design has to isolate that advantage.
- Posture outcomes should include time spent in forward head or high head-tilt positions, not just one-time classification accuracy.
- Clinical outcomes should include symptom frequency, pain intensity, functional limitation, and recurrence.
- Adherence outcomes should report how often users disable prompts, ignore cues, or abandon the tool.
- Safety outcomes should include discomfort, anxiety about monitoring, and unintended changes in movement behavior.
- Durability should be measured after the initial novelty period, not only during short-term supervised use.
The most useful endpoint would not be “the app detected posture.” It would be a measurable reduction in risky posture exposure paired with improved or preserved musculoskeletal outcomes over time. Detection is the mechanism. Prevention is the claim that still needs testing.
Regulatory and deployment reality
No FDA-cleared or CE-marked AI device specifically approved for treatment of smartphone-related RSI was identified in the supplied evidence. That does not prevent consumer posture tools from existing, but it affects how clinicians and health systems should describe them. At present, the defensible language is posture monitoring, ergonomic feedback, or preventive support, not approved treatment for smartphone RSI.
Clinical deployment would also need mundane safeguards: transparent camera permissions, local processing by default, clear data retention settings, accessible opt-out controls, and careful wording around risk. A tool that watches posture all day can become either useful feedback or one more source of friction, depending on how often it interrupts and how well the cue matches the user’s actual task.
For health IT teams, the appeal is scalability. One clinician cannot watch every phone session. A smartphone can, at least technically, estimate posture in real time on the same device that is contributing to the exposure. But scale does not remove the need for validation. It raises the cost of being wrong, irritating, or overconfident.
The claim that current evidence can support
On-device AI pose estimation appears technically capable of detecting the visible postural precursors linked to smartphone-related musculoskeletal loading. The performance reported by Heo et al. makes real-time feedback plausible on consumer phones, and the biomechanical findings summarized by Eitivipart et al. explain why head tilt, forward head shift, and upper shoulder loading are reasonable targets.[1][2]
The treatment claim should remain narrower. Current evidence does not yet show that AI posture correction prevents smartphone-related RSI, treats diagnosed RSI, or produces durable clinical benefit beyond the studied time windows and populations. The next step is not a louder promise; it is controlled research in symptomatic or high-risk users, with outcomes that measure pain, function, recurrence, adherence, and sustained behavior change.
References
- The effects of smartphone use on the status of the head and neck, electromyography activity of cervical muscles, and grip and pinch strength among healthy adults: a systematic review, PMC, 2018.
- Clinical validation of on-device AI real-time pose estimation and exercise prescription, PMC, 2026.
- Critical review of AI in postural management, PMC, 2026.
Comments
Join the discussion with an anonymous comment.