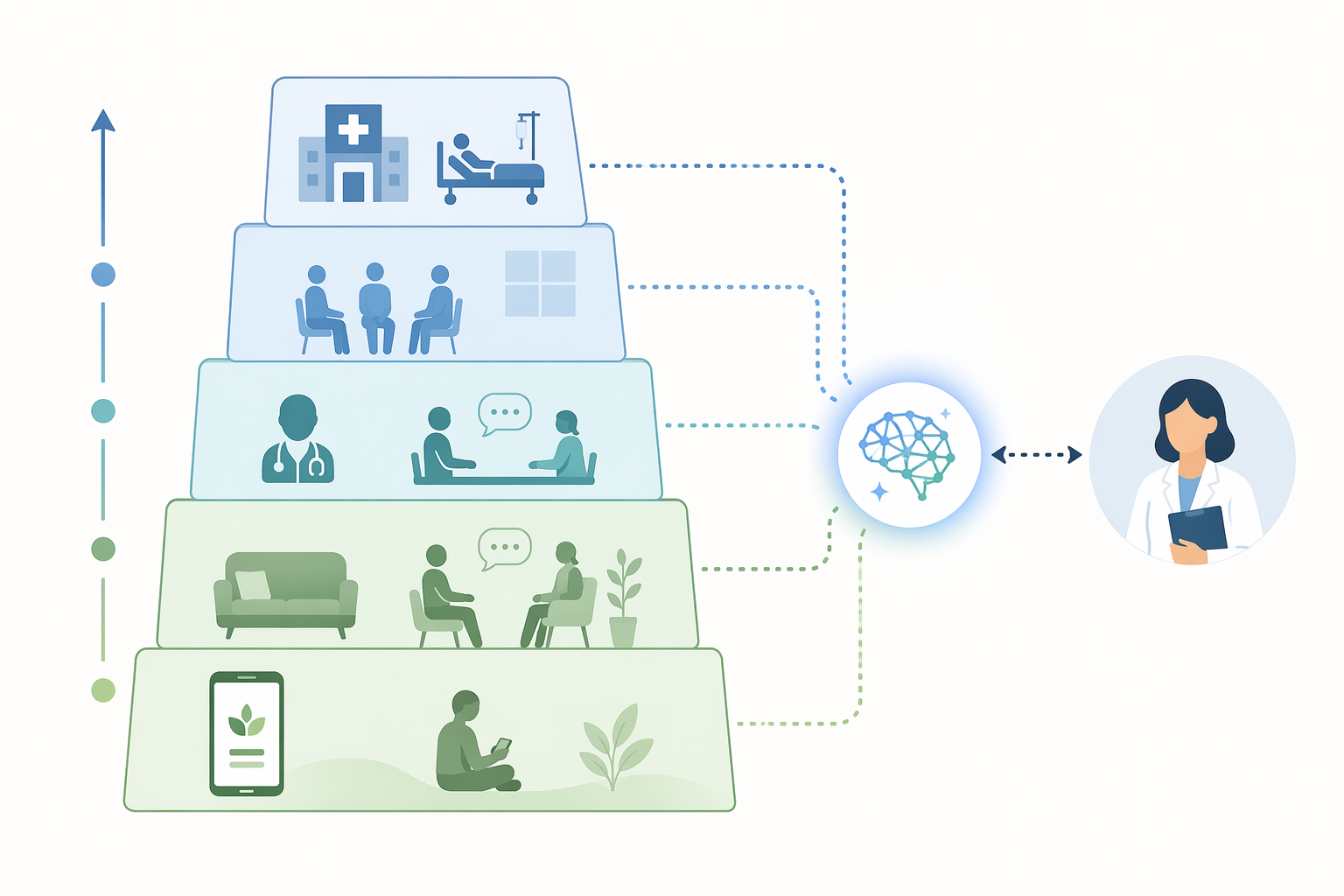
“Placement” sounds tidy until it reaches a counseling center. In practice, AI for student placement in mental health programs is not usually deciding whether a student has a diagnosis, and it is not replacing the clinician who carries responsibility for risk. It is more often an AI-assisted triage layer inside a stepped-care workflow: a student enters through an intake form or digital assessment, the system recommends a level of care, and a human service has to decide whether that recommendation is safe enough to act on.
That distinction matters because “the right care level” is not a single destination. For one student, it may be guided digital self-help with monitoring. For another, weekly therapy. For another, psychiatric consultation, intensive outpatient care, or emergency evaluation. The useful question is not whether AI can sort students neatly. It is whether AI can reduce delay without quietly moving risk into a lower-intensity lane.
What the strongest direct study actually showed
The most relevant direct evidence comes from a prospective Queen’s University and OPTT study of an AI-assisted triage and online psychotherapy initiative in an ambulatory psychiatric setting. The study included 101 patients and reported three operationally important findings: wait times fell by 71.43%, AI recommendations agreed with psychiatrists on care-level and disorder-specific pathway recommendations 71.29% of the time, and 63% of patients placed into low-intensity AI pathways required no further psychiatric consultation after a final psychiatric assessment [1].
Those numbers are not cosmetic. A shorter wait time means fewer students sitting in the queue while symptoms worsen or academic deadlines keep moving. A low-intensity placement that does not later require psychiatric consultation suggests that at least some students can be routed away from scarce specialist appointments without obvious downstream correction. Concordance above 70% with psychiatrists is also meaningful, especially in a system where human clinicians themselves may disagree on borderline care levels.
| Study measure | Reported result | Why it matters operationally |
|---|---|---|
| Wait-time reduction | 71.43% | Suggests AI-assisted triage may move students into an initial care pathway faster |
| Agreement with psychiatrists | 71.29% | Shows moderate-to-strong concordance on care level and pathway recommendations |
| Low-intensity placements needing no further psychiatric consultation | 63% | Suggests some lower-acuity students may be safely diverted from specialist queues after review |
The limitation is just as important as the result. The Queen’s University/OPTT study was small, with n=101, and the sample was predominantly white, female, and Canadian [1]. That does not make the findings unusable. It does mean they should not be treated as validated performance across U.S. campuses with different racial, socioeconomic, linguistic, insurance, disability, and help-seeking patterns.
There is also a source-transparency issue. The study is more substantive than a product announcement, but available materials identify OPTT Inc. co-founders among the study authors. That makes the evidence worth reading, not automatically dismissing. It also makes independent replication more important before a campus treats the reported concordance as a general benchmark.
Agreement is not the same as safety
A 71.29% agreement rate answers one question: how often did the AI and psychiatrists land in the same place in this study? It does not fully answer several questions counseling centers have to live with after deployment: where did the disagreements occur, which groups were most affected, and how often did the system place a higher-risk student into a lower-intensity pathway?
The last question is the one that changes governance. If an AI tool over-classifies moderate distress as severe, the system may consume too many psychiatric appointments. That is inefficient and may crowd out students who need urgent care. If it under-classifies severe distress as moderate, the student may enter a pathway with less monitoring than they need. The operational cost is then no longer just scheduling pressure; it is clinical exposure.
This is why AI placement should be evaluated by error type, not just by average agreement. A campus director needs to know whether the model is safer with anxiety presentations than eating-disorder presentations, whether suicidal ideation is reliably escalated, whether international students are routed differently from domestic students with similar severity, and whether students who write less fluently in English receive lower acuity estimates. The available direct evidence does not yet settle those subgroup questions.
Campus deployments show the use case is no longer theoretical
U.S. universities are already experimenting with AI-supported matching and triage. Heartland Forward describes Wayhaven deployments at Butler University and the University of Houston, and TimelyCare’s broader student telehealth platform at the University of Oklahoma, the University of Texas, and the University of Illinois [2]. These examples do not carry the same evidentiary weight as independent clinical validation, but they show that campus AI placement is moving from concept into service design.
Wayhaven is the more clinically revealing example because its reported data include a conservative severity bias: the system tends to under-classify severe cases as moderate, requiring clinician override [2]. The word “conservative” can sound reassuring in a technical report, but in triage it needs translation. A severe case labeled moderate is not conservative for the student, the clinician, or the institution unless the workflow requires human review before that recommendation affects access.
That finding points toward a practical design rule: severe-risk review cannot be optional. If a platform’s own materials indicate under-classification of severe cases, then mandatory clinician review, escalation thresholds, and override documentation are not add-ons. They are the safety architecture.
TimelyCare matters in a different way. Its use at several universities shows how AI matching may be embedded inside a larger telehealth infrastructure rather than purchased as a stand-alone triage engine [2]. That can make access easier for students, but it can also make responsibility less visible: the intake interface, matching logic, telehealth vendor, campus counseling center, and outside referral network may all touch the student before anyone has a full clinical picture.

Digital-first care has supporting evidence, but it does not validate AI triage by itself
The strongest adjacent support for stepped care comes from UCLA’s population-based randomized controlled trial of a digital cognitive-behavioral guided self-help intervention for anxiety, depression, and eating disorders in college students. The 2026 study included more than 1,000 students and reported that guided digital CBT self-help outperformed passive referrals to campus clinics [3].
That result supports a premise many counseling centers already suspect: for some students, an immediate guided digital intervention may be more useful than being handed a referral and left to navigate availability, motivation, stigma, and scheduling. It also gives stepped-care models a stronger clinical footing. Lower-intensity care is not automatically inferior care when it is matched well, delivered promptly, and monitored.
But the UCLA finding should not be stretched beyond what it tests. It does not prove that an AI system can correctly decide which student belongs in guided self-help, therapy, psychiatry, or intensive care. It says that a digital guided self-help pathway can outperform passive referral under the conditions studied [3]. The placement problem remains: who gets sent there, who is excluded, and who checks whether the student is improving.
The students most at risk may already be using AI
A Mass General Brigham study adds a useful relevance signal: students with the highest distress were found to use AI for mental health at elevated rates [4]. That does not establish that AI use caused distress, reduced distress, or substituted for care. It does suggest that the students campus clinicians worry about most may also be the students most exposed to algorithmic mental health guidance outside formal clinical workflows.
For counseling centers, that context matters. A student may arrive after already asking a general AI chatbot whether their symptoms are serious, whether they need therapy, or whether they should tell anyone about self-harm thoughts. A campus placement system has to be safer than that informal environment. It has to explain its role, route risk upward, and make clear that a care-level recommendation is not a diagnosis or a final clinical decision.
What supervised placement should require
The current evidence supports AI as decision support inside a supervised stepped-care workflow. It does not support autonomous placement. A counseling center using these systems should be able to describe, in ordinary clinical language, where the AI recommendation enters the workflow and where human judgment can stop it.
- Human override: clinicians must be able to change the recommended care level without treating the algorithm as the default authority.
- Mandatory escalation: suicide risk, psychosis, severe eating-disorder symptoms, acute safety concerns, and other high-risk signals should trigger human review before low- or moderate-intensity placement.
- Subgroup validation: performance should be assessed across race, gender, language, disability, international status, and other locally relevant student groups before broad reliance.
- Source transparency: campuses should distinguish peer-reviewed evidence, vendor-adjacent studies, self-published data, press-release summaries, and independent replications.
- Student communication: students should be told when AI contributes to triage and should understand that placement recommendations are reviewed within a clinical workflow.
One more boundary should be stated plainly: no FDA-cleared or CE-marked AI placement system specifically for student mental health was identified in the available materials. That does not prevent research or operational use where legally appropriate, but it makes local governance, documentation, and clinical accountability more important, not less.
A conditional answer
AI can help match students to mental health care levels when the task is defined narrowly: decision support for triage, embedded in stepped care, reviewed by clinicians, and measured against local student outcomes. The Queen’s University/OPTT results make the case worth taking seriously, especially on wait times and psychiatrist concordance [1]. The Wayhaven materials make the oversight problem impossible to ignore, especially where severe cases may be under-classified as moderate [2].
The safest conclusion is not a yes-or-no verdict. Current evidence supports supervised AI-assisted placement as a way to improve access and preserve higher-intensity resources for students who need them most. It does not yet justify autonomous routing, untested generalization across campuses, or procurement claims that treat matching as a solved problem.
References
- Evaluation of an Artificial Intelligence and Online Psychotherapy Initiative to Improve Access and Efficiency in an Ambulatory Psychiatric Setting — Queen's University/OPTT prospective study.
- New Possibilities: College Campuses Leverage Artificial Intelligence for Mental Health Support — Heartland Forward.
- Population-based RCT of a digital cognitive-behavioral guided self-help intervention for anxiety, depression, and eating disorders in college students — Nature Human Behaviour, 2026.
- Study Finds Students with Highest Distress Use AI for Mental Health at Elevated Rates — Mass General Brigham.
Comments
Join the discussion with an anonymous comment.