The strongest current evidence for AI in mental health support and advocacy does not support the clean headline that therapy chatbots “work” or “do not work.” It supports a narrower, more clinically useful claim: some AI-delivered cognitive behavioral therapy chatbots can reduce symptoms over short periods in selected mild-to-moderate populations, especially for depression, but the evidence is not broad enough to treat these systems as substitutes for human therapy or as autonomous clinical services.
That distinction matters more in 2026 because the field is no longer limited to scripted, rule-based CBT bots. Earlier systems generally followed constrained therapeutic pathways. Newer generative systems can respond more flexibly, sustain a more natural conversation, and appear more personally attuned. That flexibility is part of why the 2025 Therabot randomized controlled trial drew attention. It is also why the safety problem is harder: the same system that can adapt conversationally can also produce misinformation, miss risk, or cross boundaries in ways that a symptom score does not capture.

The Therabot Trial Changed the Size of the Signal
Therabot is the study that makes blanket dismissal of AI therapy chatbots harder to defend. In a randomized trial published in NEJM AI in March 2025, Heinz and colleagues tested a fully generative AI chatbot in 210 adults with clinical-level symptoms of major depressive disorder, generalized anxiety disorder, or eating disorder concerns. Across conditions, the trial reported effect sizes in the d=0.63–0.90 range, and participants with depression showed a 51% reduction in depressive symptoms during the study window.[1]
Those are not trivial numbers. In this area, a moderate-to-large short-term symptom reduction is clinically interesting, especially when the intervention is scalable and can be accessed outside traditional appointment slots. The depression result is the cleanest reason to take the trial seriously. It suggests that a chatbot delivering therapeutic techniques conversationally can do more than provide generic wellness prompts or mood tracking.
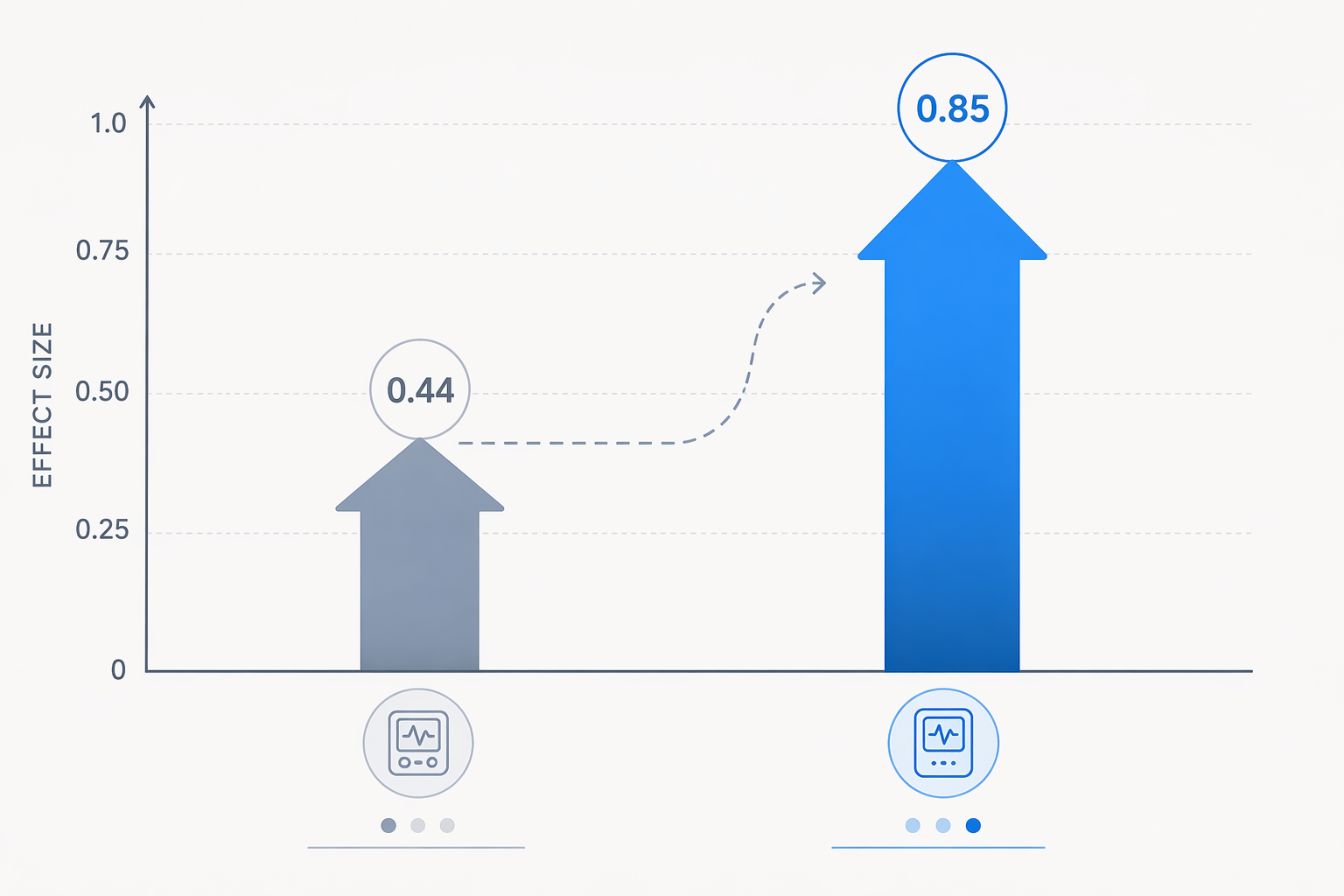
The comparison with earlier rule-based tools explains why the trial felt like a step-change. Woebot’s earlier 2017 trial is commonly used as a baseline for scripted CBT chatbot evidence, with an effect size around d≈0.44. Therabot’s reported range, including values around d≈0.85, sits substantially higher than that earlier rule-based benchmark.[1]
The therapeutic alliance finding is also important, but it should be handled carefully. Participants reported alliance scores comparable to those seen with human therapists.[1] That does not mean the chatbot formed a human-equivalent therapeutic relationship. It means that, within this trial and over a short window, participants rated the interaction as credible, collaborative, or supportive enough to resemble alliance scores measured in human therapy contexts. That is meaningful for engagement. It is not the same as evidence that a system can hold clinical responsibility.
The trial’s limitations are not footnotes. It was short-term. It studied selected clinical populations rather than the full range of patients who might be routed to a chatbot in routine care. It evaluated a proprietary system, and the trial was conducted by the tool’s developers.[1] Those facts do not erase the result. They define the claim that can safely be made from it.
What Short-Term Symptom Reduction Actually Means
A two-to-eight-week improvement in symptom scores is a real endpoint. It can mean fewer depressive symptoms, less distress, better day-to-day functioning, or enough stabilization to keep someone engaged while waiting for other care. For health systems with long waitlists, that is not a cosmetic benefit.
It does not show durability. It does not show relapse prevention. It does not show that a chatbot can manage medication questions, trauma complexity, substance use comorbidity, suicide risk, psychosis, severe eating disorder physiology, family violence, or the accumulating clinical ambiguity that often becomes visible only after repeated human contact. Short-term symptom reduction is a legitimate outcome, but it is not a proxy for comprehensive care.
This is where the evidence often gets overstated. A chatbot can reduce a depression score in a selected study population without being ready to replace a therapist, a triage clinician, or a crisis pathway. The more appropriate question is what role the tool can safely occupy: early support, adjunctive CBT practice, between-session reinforcement, guided self-help, or intake support. Those roles carry different risks than unsupervised treatment.
The Broader CBT Chatbot Evidence Is Supportive, But Uneven
Therabot should not be used as the entire evidence base. A 2025 narrative review in JMIR Mental Health examined 14 CBT chatbot studies and found consistent short-term reductions in depressive symptoms, generally with moderate effects. The same review found anxiety outcomes were more mixed, which is a critical difference from the simpler claim that CBT chatbots broadly improve “mental health.”[2]
That pattern is plausible clinically. Depression interventions can benefit from behavioral activation, cognitive restructuring, routine-building, and repeated prompts that a chatbot can deliver consistently. Anxiety treatment can require exposure work, careful avoidance mapping, safety-behavior reduction, and calibration of reassurance. A chatbot that responds supportively may help some anxiety symptoms while also risking subtle reinforcement of reassurance-seeking if the design is not disciplined.
| Claim | What the evidence supports | What remains unresolved |
|---|---|---|
| Depression symptom reduction | Consistent short-term improvement across CBT chatbot studies, with Therabot reporting a 51% depression reduction | Durability beyond short follow-up windows and performance in more severe or complex depression |
| Anxiety improvement | Some positive findings, including in Therabot’s generalized anxiety disorder group | Mixed outcomes across the broader CBT chatbot literature |
| Therapeutic alliance | Participants in the Therabot trial reported alliance scores comparable to human-therapy contexts | Whether alliance ratings predict safety, durable benefit, or responsible escalation |
| Clinical equivalence | Evidence of short-term benefit in selected populations | No basis for broad equivalence to human therapy |
The review also helps correct a common interpretation error. Adoption evidence, user satisfaction, and symptom improvement are not interchangeable. A chatbot that people like using may not produce clinically meaningful change. A chatbot that improves a scale over four weeks may still fail on escalation. A chatbot that performs well in one diagnostic group may not generalize to another. The evidence is becoming stronger, but it is not flattening those distinctions.
Real-World Deployment Is Emerging, Not Settled
The NHS Limbic Care implementation is a useful signal because it comes from routine service conditions rather than a tightly controlled chatbot trial. In the NHS Talking Therapies program, the implementation was associated with a 25-percentage-point higher recovery rate and 23% lower dropout.[3]
That finding deserves attention, but it should not be made to do too much. Implementation outcomes in a national health system can show that a tool may improve access, routing, engagement, or completion within a service pathway. They do not automatically prove that the chatbot itself is equivalent to therapy or that the same result would appear in a different population, payment model, clinical workflow, or risk protocol.
For procurement teams, the distinction is practical. If a tool reduces dropout by helping people enter the right pathway faster, that is valuable. If a vendor uses the same result to imply autonomous treatment capacity, the claim has moved beyond what the implementation can establish. Health systems need to know which component improved: triage, engagement, waiting-list support, symptom management, clinician workflow, or all of these together.
The Population Boundary Is Still Narrow
Most current studies are concentrated in adult, mild-to-moderate populations in high-income settings, with short follow-up windows of roughly two to eight weeks.[2] That does not make the evidence weak; it makes it specific. The people most likely to be harmed by overdeployment are often the people least represented in the evidence: youth, patients with severe symptoms, people with high suicide risk, patients with psychosis or complex trauma, people with unstable housing, and users in low- and middle-income countries where cultural adaptation, language performance, and clinical backup may differ substantially.
This matters because AI systems tend to scale faster than clinical governance. A narrowly tested tool can become a broadly marketed tool before anyone has answered whether it works for patients with comorbidities, whether it recognizes deterioration, whether it performs similarly across dialects and literacy levels, or whether escalation pathways are actually staffed when risk is detected.
The unresolved issue is not only whether the model gives a bad answer. It is who notices, who intervenes, and who explains the decision later. In mental health care, the harm from a missed escalation may not look like a single dramatic malfunction. It may look like a patient being reassured when they needed assessment, being kept in self-help when they needed stepped-up care, or being given plausible but inappropriate guidance that delays contact with a clinician.
Generative Systems Add Safety Questions That Efficacy Trials Do Not Fully Measure
The move from rule-based CBT chatbots to generative AI changes the safety profile. A scripted system can still be poorly designed, but its response space is constrained. A generative system can improvise. That may make it feel more responsive and less mechanical. It also makes boundary control, clinical accuracy, crisis detection, and auditability more difficult.
The Therabot trial’s alliance findings show that users may experience a generative chatbot as therapeutically engaging.[1] Engagement is useful only if the system stays within a safe clinical lane. A chatbot that sounds empathic while providing inaccurate clinical information, failing to identify danger, or encouraging overreliance is not safer because the interaction felt supportive.
Safety evaluation therefore has to include more than average symptom change. It needs adversarial testing, review of high-risk transcripts, monitoring for inappropriate reassurance, escalation accuracy, hallucinated clinical claims, privacy handling, and post-deployment drift. Those are operational burdens. They land on clinicians, risk teams, compliance officers, and service managers long after the purchase decision has been made.
Regulation Has Not Caught Up to the Clinical Claim
As of the November 2025 regulatory review summarized by Herpertz and colleagues, no generative AI chatbot had received FDA clearance to diagnose or treat a mental health disorder. The review identified 19 FDA-authorized software-as-a-medical-device products in mental health, but these were rule-based or CBT-protocol approaches rather than generative AI therapy chatbots.[4]
That status matters because marketing language can move faster than authorization. A tool may be described as supportive, wellness-oriented, therapeutic, CBT-based, AI-powered, or clinically validated. Those phrases do not all mean the same thing. For a health system, the relevant questions are more concrete: What indication is being claimed? What population was tested? What comparator was used? What risks were excluded? What happens when the user discloses imminent harm? Who audits the output?
The FDA Digital Health Advisory Committee’s November 2025 discussion of a risk-based framework for generative AI mental health devices signals that regulators recognize the mismatch between emerging evidence and existing device categories.[4] The hard part is that generative mental health tools are not static interventions. Their safety depends not only on the model but also on prompts, guardrails, updates, monitoring, clinical workflow, escalation design, and the claims made at deployment.
A Responsible Adoption Posture
The evidence now supports taking AI-delivered CBT chatbots seriously as supervised support for short-term symptom reduction in selected mild-to-moderate cases. Depression is the strongest current signal. Anxiety benefit is plausible but less consistent. Generative AI, especially in the Therabot trial, appears capable of producing larger effects than earlier rule-based predecessors, but that does not convert a short-term RCT into proof of broad clinical equivalence.
A health system evaluating these tools should treat human oversight as part of the intervention, not as an optional safety accessory. That means defined inclusion and exclusion criteria, escalation pathways for crisis and deterioration, clinician review where risk is detected, source-level verification of clinical content, transcript audit capacity, monitoring for model changes, and clear patient-facing language about what the tool can and cannot do.
The evidence has moved from novelty to clinically relevant signal. It has not moved from signal to unsupervised standard of care.
References
- Randomized Trial of a Generative AI Chatbot for Mental Health Treatment, NEJM AI, March 2025, https://ai.nejm.org/doi/full/10.1056/AIoa2400802
- Effectiveness of Cognitive Behavioral Therapy Chatbots for Mental Health: Narrative Review, JMIR Mental Health, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC12669916/
- NHS Limbic Care implementation, JMIR, 2025, Referenced in Forbes/NEJM AI coverage
- Software as a Medical Device in Mental Health: Current Regulatory Landscape and Future Directions, npj Mental Health Research, November 2025, https://www.nature.com/articles/s44184-025-00174-2
Comments
Join the discussion with an anonymous comment.