The useful question about AI in severe weather warning systems is no longer whether a model can draw an impressive storm map. For hospitals, the question is whether a credible signal arrives early enough to change a schedule, open an incident command conversation, check oxygen and pharmacy constraints, adjust transport plans, or warn an emergency department that tomorrow’s staffing template was built for the wrong day.
That is where the field has become interesting. AI weather systems are beginning to produce severe-weather and environmental-health signals on timelines that match hospital operations better than bedside medicine: several days for convective hazards, two weeks in one heat-mortality forecasting example, and short-range environmental forecasts that can matter to respiratory services. The uncomfortable part is that most of this evidence still lives on the weather side of the bridge. A forecast of hail, damaging wind, extreme heat, or air pollution is not yet a validated forecast of ED arrivals, admissions, ICU strain, staffing failure, or ambulance diversion.

Lead Time Is the Clinical Feature
Hospitals do not need every atmospheric detail to be perfect before they can use a warning. They need enough lead time, enough reliability, and enough local relevance to justify a proportional action. A three-day signal can influence staffing and elective load. A week-long signal can change bed huddles, supply checks, and mutual-aid discussions. A two-week signal, if tied to health outcomes, can begin to look like a planning horizon rather than a weather bulletin.
The weather models are moving into that operational window. In May 2026, NSF NCAR described AI weather model emulators that estimate probabilities for tornadoes, hail, and damaging winds at 3–8 day lead times, with forecasts running in minutes rather than the hours typically required for traditional model workflows.[1] That matters because a forecast that arrives after the staffing office has already locked the schedule is clinically interesting but operationally late.
NOAA’s Weather Program Office describes the CSU Machine Learning Probabilities system, or CSU-MLP, as operational at the Storm Prediction Center since 2024, producing 4–8 day severe-weather outlooks and helping forecasters improve confidence in storm prediction.[2] The important word for a hospital is not “machine learning.” It is “outlook.” An outlook is not an activation order, but it can justify asking whether the weekend respiratory therapist schedule, ambulance offload plan, or bed-capacity assumption is still defensible.
The broader AI-weather landscape is also pushing environmental forecasting beyond single-hazard maps. Microsoft’s Aurora foundation model was trained on more than 1 million hours of atmospheric data, beat existing models across 91% of forecasting targets in Nature-reported results, and can predict air pollution 5 days ahead.[3] That does not prove a hospital surge model. It does mean that air quality, temperature, and severe-weather signals are becoming available in forms that clinical informatics teams can plausibly ingest before the surge is already visible in the waiting room.
The Evidence Gap Starts After the Weather Forecast
The translational problem is easy to underestimate because the first half of the chain is becoming so capable. A severe-weather probability can be technically strong and still fail to answer the hospital question. The ED charge nurse does not staff to a convective outlook. The command center does not open beds for a heat index. They act when a hazard forecast is linked to a plausible health burden, then translated into capacity strain and a threshold for action.
That bridge remains thin. A 2026 systematic review of 134 studies on heatwaves, health impacts, and AI-based preparedness found that only a small subset linked AI hazard forecasts to hospital surge planning, identifying the translation from hazard prediction to surge planning as a primary research frontier.[4] This is the constraint that should keep hospital leaders from treating even impressive AI weather forecasts as turnkey clinical surge predictors.
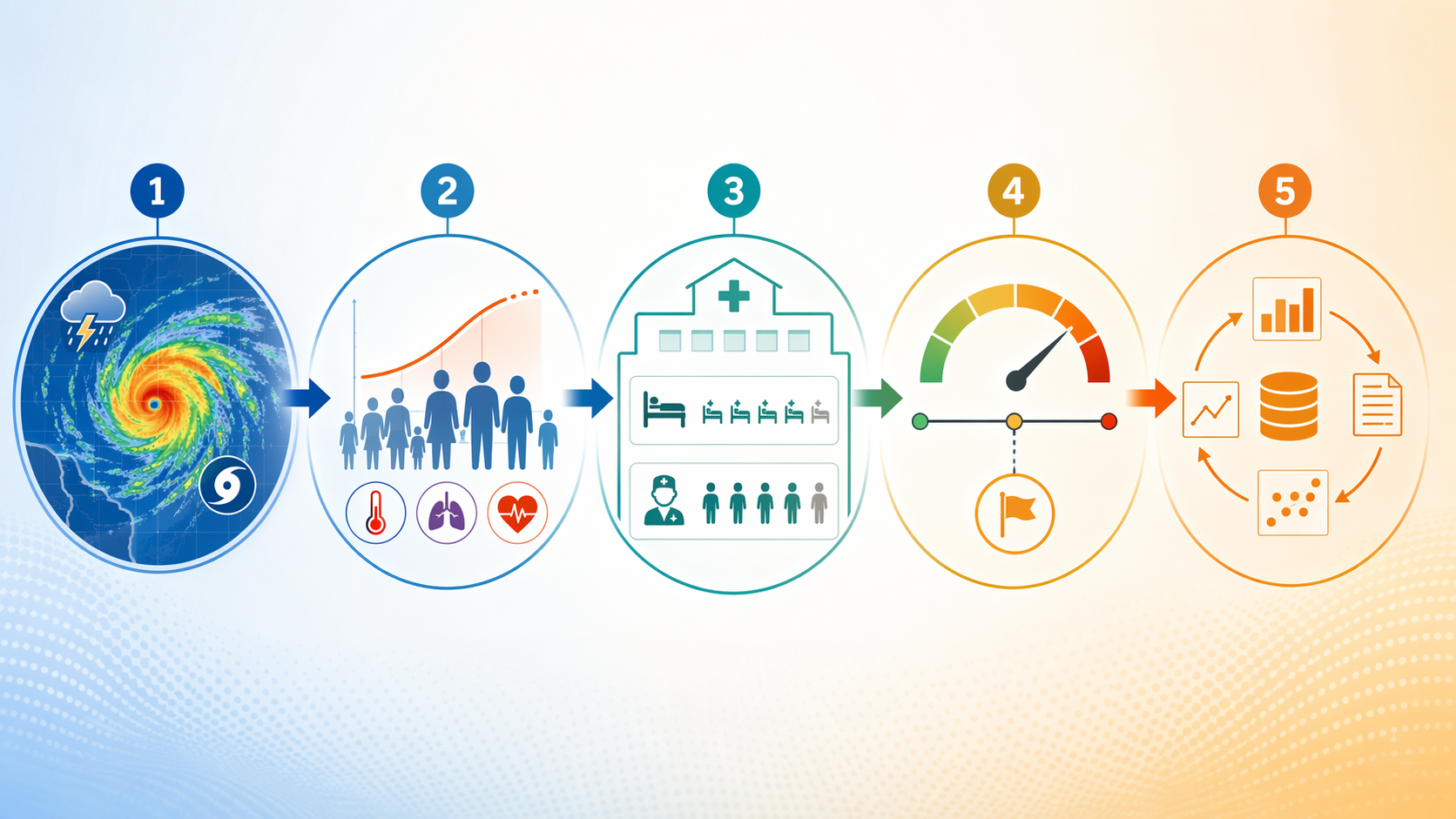
| Translational step | Operational question | Evidence standard |
|---|---|---|
| Forecast hazard | What severe-weather or environmental exposure is likely, where, and when? | Meteorological model performance, calibration, and lead time |
| Estimate health impact | Which populations are likely to experience excess morbidity or mortality? | Exposure-response models linked to local demographics and vulnerability |
| Map to capacity | Which hospital services will feel the load first? | Historical encounters, admissions, staffing, bed, pharmacy, EMS, and transfer data |
| Define thresholds | What probability or expected volume justifies action? | Predefined operating thresholds with accountable owners |
| Validate outcomes | Did the alert improve readiness without excessive false activation? | Retrospective and prospective comparison against real operational outcomes |
The table is deliberately mundane. That is the point. The most valuable hospital use of AI weather forecasting may not look like a dramatic bedside alert. It may look like a Tuesday morning decision to move a staffing request forward, protect inpatient discharge capacity, or warn respiratory leadership that a weather-linked signal deserves attention before the daily census proves it.
Heat Shows What the Bridge Can Look Like
Heat is the clearest example because the hazard-to-health relationship has a measurable exposure-response structure. Holmberg and colleagues, described in a 2025 PNAS commentary, demonstrated that heat-related mortality can be forecast up to 14 days in advance by coupling AI meteorological models with nonlinear temperature-mortality exposure-response functions.[5] The clinical lesson is not simply that heat is dangerous. It is that the forecast becomes more useful when the model estimates what the heat may do to people, not only what the thermometer may read.
A hospital still has to add its own layer. Mortality risk does not translate neatly into ED arrivals. Heat may increase dehydration, renal injury, cardiovascular stress, falls, behavioral health crises, medication-related complications, and demand for cooling resources. Some of that burden presents directly to acute care; some appears in EMS calls, skilled nursing transfers, outpatient deterioration, or delayed admissions. A health-system model that ignores those local pathways can be mathematically elegant and operationally vague.
The right use of a 14-day heat-mortality signal is therefore not to announce a fixed admission count. It is to open a planning window: review high-risk catchment areas, check whether weekend staffing is brittle, confirm cooling-center communications, look at dialysis and home-health coordination, and decide which threshold would trigger formal incident command attention. The forecast buys time; it does not remove judgment.
Respiratory Surge Prediction Is Closer to the Hospital Floor
Respiratory services offer another practical path because they already live with seasonal and environmental signals. Harvard Medicine Magazine reported in 2024 that Boston Children’s Hospital and Harvard researchers developed machine-learning models that predict pediatric respiratory surge “to the day” using environmental, behavioral, and infectious-disease data.[6] That kind of model is closer to the hospital floor because it does not stop at the weather layer. It combines environmental conditions with the signals that actually shape pediatric demand.
For an operations team, the key design choice is the outcome. A model trained to predict a broad respiratory surge may be useful for service-line awareness. A model trained to predict ED arrivals may help triage staffing. A model trained to predict admissions, ICU transfers, high-flow oxygen demand, or ventilator use may change inpatient capacity planning. These are not interchangeable endpoints. If the model is vague about which operational queue it predicts, the hospital will discover the gap during the surge.
This is where environmental AI can become clinically useful without pretending to be clinical decision support for an individual patient. A weather-linked respiratory signal can tell a hospital that a population-level load is becoming more likely. It should not tell a clinician how to treat a child at the bedside unless it has been validated for that purpose. Keeping that boundary clear protects both the model and the staff expected to act on it.
Personalized Alerts Prove Feasibility, Not Surge Validation
Consumer and payer deployments show that weather intelligence can be joined with clinical or demographic data at scale. Forbes reported in July 2025 that EmblemHealth launched an AI-personalized Weather Resilience Program for Medicare and Medicaid members, with reported satisfaction of 9 out of 10.[7] That is a meaningful implementation signal: weather alerts can be localized, personalized, and delivered through a health organization rather than a standalone weather app.
It is still adjacent evidence. Member satisfaction does not prove lower admissions, fewer ED visits, improved medication safety, or reduced mortality. It also does not prove that a hospital can infer capacity strain from alert distribution. A payer-facing alert system and a command-center surge model share data ingredients, but they answer different questions. One asks whether a person received a useful warning. The other asks whether a hospital should change operations before demand materializes.
Thresholds Matter More Than Dashboards
A forecast that never changes a decision becomes a dashboard ornament. The hospital needs thresholds: not because thresholds are perfect, but because someone has to know what level of probability, expected volume, or subsystem stress opens the next operating posture.
Gish and Rapaport proposed an agentic AI framework in npj Digital Medicine in 2026 that uses threshold-based planning, with AI agents continuously monitoring hospital subsystems as a complement to scenario-based contingency planning for unprecedented weather events.[8] That framing is useful because it starts from hospital operations rather than from the weather model alone. The object being monitored is not only the storm. It is the emergency department, inpatient beds, staffing, supply chain, respiratory capacity, and other subsystems that fail unevenly.
Threshold-based planning also forces a difficult conversation before the alert fires. What happens at a 20% probability of a severe convective event affecting the catchment area? What happens when a heat-health model suggests a high-risk window overlaps a holiday weekend? Which action is low-cost enough to trigger early, and which action requires stronger evidence? The answer will differ for staffing, pharmacy, EMS coordination, elective procedures, and incident command activation.
A practical pilot might start with modest, reversible actions: flag the risk in the bed meeting, ask staffing to identify contingency options, check respiratory supplies, review ambulance diversion status, and alert clinical leaders that the forecast is being watched. Higher-cost actions, such as canceling procedures or opening command structures, should require stronger thresholds and a record of prior performance. That discipline prevents both underreaction and forecast-driven theater.
The Hard Parts Are Statistical and Organizational
Rare events are the first problem. Severe weather is uncommon by definition, and the hospital outcomes tied to it may be even rarer after stratifying by geography, service line, age group, and exposure. A model can look accurate overall while missing the cases that matter most. Accuracy on calm days does not help the charge nurse on the day the waiting room, ambulance bay, and inpatient bed board all deteriorate together.
Transferability is the second problem. A model trained in one climate, one health system, or one urban infrastructure pattern may not travel cleanly to another. Heat risk in a dense city with older housing, limited tree canopy, and high air-conditioning variability is not the same operational problem as heat risk in a different region with different housing stock and hospital access. Convective weather may stress EMS, trauma, power reliability, or outpatient access differently depending on local geography.
Explainability is the third. Hospital leaders can tolerate some model complexity, but they need to know why an alert is firing well enough to defend the action. “The model says so” is weak support for changing staffing or diverting ambulances. A useful system should show the contributing hazard, expected timing, affected population, uncertainty, prior performance, and the operational threshold being crossed.
Regulatory classification is another unresolved seam. These tools sit between meteorological forecasting, public health preparedness, hospital operations, and sometimes clinical risk communication. A population-level severe-weather activation tool is not the same as bedside diagnostic software, but it can still affect patient access, staffing, and resource allocation. That ambiguity argues for governance early in the pilot, not after the tool has become embedded in daily operations.
What a Defensible Hospital Pilot Would Measure
The first pilot should not claim to predict “surge” as a single outcome. Surge is a word hospitals use when several queues are already colliding. The model should choose specific operational endpoints: ED arrivals, EMS arrivals, left-without-being-seen risk, inpatient admissions, ICU demand, respiratory therapy workload, pharmacy demand, staff call-outs, transfer requests, or ambulance diversion hours. A forecast that helps one endpoint may be irrelevant to another.
- Define the hazard signal: convective risk, heat, air pollution, flooding exposure, or a combined environmental index.
- Define the clinical or operational endpoint: arrivals, admissions, staffing strain, bed occupancy, EMS offload, or service-line workload.
- Set lead-time windows separately: same-day response, 1–2 day staffing adjustment, 3–8 day planning outlook, or longer heat-health planning.
- Predefine actions by threshold: awareness only, staffing review, supply check, command notification, or formal activation.
- Track false positives and false negatives as operational events, not just statistical errors.
False positives are not harmless. They spend leadership attention, staff goodwill, and sometimes money. False negatives are not merely missed forecasts; they leave departments doing remedial work under pressure. The right evaluation therefore includes whether the alert changed decisions, whether those decisions were proportionate, and whether the hospital would make the same decision again with the same information.
Retrospective validation is the starting point: replay prior weather seasons against prior hospital outcomes and ask whether the proposed thresholds would have helped. Prospective silent trials are the next step: run the model without changing operations, compare alerts with actual demand, and tune thresholds. Only then should the system move into live decision support, and even then with named human owners for activation choices.
Promising, but Not Yet a Ready-Made Surge Predictor
AI weather forecasting has crossed an operationally meaningful line. Severe-weather probabilities several days out, rapid model runtimes, air-quality forecasts, heat-mortality modeling, and respiratory surge work all point in the same direction: hospitals can receive earlier environmental signals than they could reasonably act on in the past.
The clinical application is not automatic. Weather performance is not hospital surge validation. The translational chain still has to connect hazard forecast, health impact, local capacity, activation thresholds, and observed outcomes. That is enough to justify pilots and serious operational research. It is not enough to treat AI severe-weather forecasts as finished hospital surge prediction systems.
References
- Identifying severe weather hazards further in the future with AI, NCAR/UCAR News, May 2026.
- CSU machine learning model helps forecasters improve confidence in storm prediction, NOAA Weather Program Office.
- Microsoft’s Aurora AI foundation model goes beyond weather forecasting, Microsoft Source / Nature, 2025.
- Devi & Kotecha 2026 systematic review, Discover Public Health, 2026.
- Saldiva commentary on Holmberg et al. heat-related mortality forecasting, PNAS, 2025.
- Machine Learning Can Predict Weather and Human Health, Harvard Medicine Magazine, 2024.
- EmblemHealth Launches New AI-Personalized Weather Alert System, Forbes, July 2025.
- Gish & Rapaport agentic AI framework, npj Digital Medicine, 2026.
Comments
Join the discussion with an anonymous comment.