The first problem with managing the health effects of wildfire smoke is not that hospitals lack concern. It is that many communities still lack a measured signal strong enough to change anyone’s next move. In the United States, 59% of counties have no regulatory air quality monitor, leaving more than 50 million people outside the routine monitoring infrastructure that usually anchors public warnings and response planning. Those gaps are not evenly distributed: counties with higher poverty rates and higher concentrations of Black and Hispanic residents are disproportionately more likely to be monitoring deserts.[1]
That matters before anyone starts talking about artificial intelligence. A county without a monitor can still have smoke, asthma, COPD, pregnancy risk, outdoor workers, schoolyards, and emergency departments. What it may not have is a timely local measurement that tells a school district to move recess indoors, a health department to target a neighborhood alert, or a clinic to start calling the patients who reliably deteriorate when particulate levels climb.
AI air quality monitoring tools are most useful when they are understood as a response to that infrastructure gap, not as a gadget category. Low-cost sensor networks, when placed densely and calibrated carefully, can give public agencies and health systems a more local picture of wildfire smoke than sparse regulatory monitors alone. The clinical question is then narrower and harder: when the local air signal changes, who acts?
Why Better Smoke Measurement Has Clinical Stakes
Wildfire smoke is often discussed as another form of PM2.5 exposure, but that can understate the operational urgency. Stanford experts have described wildfire smoke as about 10 times more toxic per unit mass than ambient PM2.5 from fossil fuel combustion.[2] The practical implication is not that every brief exposure becomes an emergency. It is that modest increases can matter more than the number on a generic particulate dashboard may suggest.
Population studies have made the stakes difficult to dismiss. Ma and colleagues estimated approximately 11,415 excess nonaccidental deaths per year in the United States from long-term wildfire smoke PM2.5 exposure; 72.5% of those deaths were attributed to cardiovascular, mental, endocrine, and digestive diseases, not only respiratory causes.[3] A 2024 review by Gould and colleagues reported that each 1 μg/m³ increase in wildfire PM2.5 was associated with a same-day 0.15% increase in all-cause mortality, a 0.25% increase in respiratory hospitalizations, and a 0.36% increase in respiratory emergency department visits.[4]
Those figures do not say that a sensor network by itself prevents deaths or admissions. They say the exposure signal is clinically relevant enough to deserve workflow attention. If smoke can change respiratory ED volume on the same day, then air quality data arriving too late, too far away, or too generically is not just an environmental information problem. It is a missed operations signal.
From Sparse Monitors to Calibrated Sensor Networks
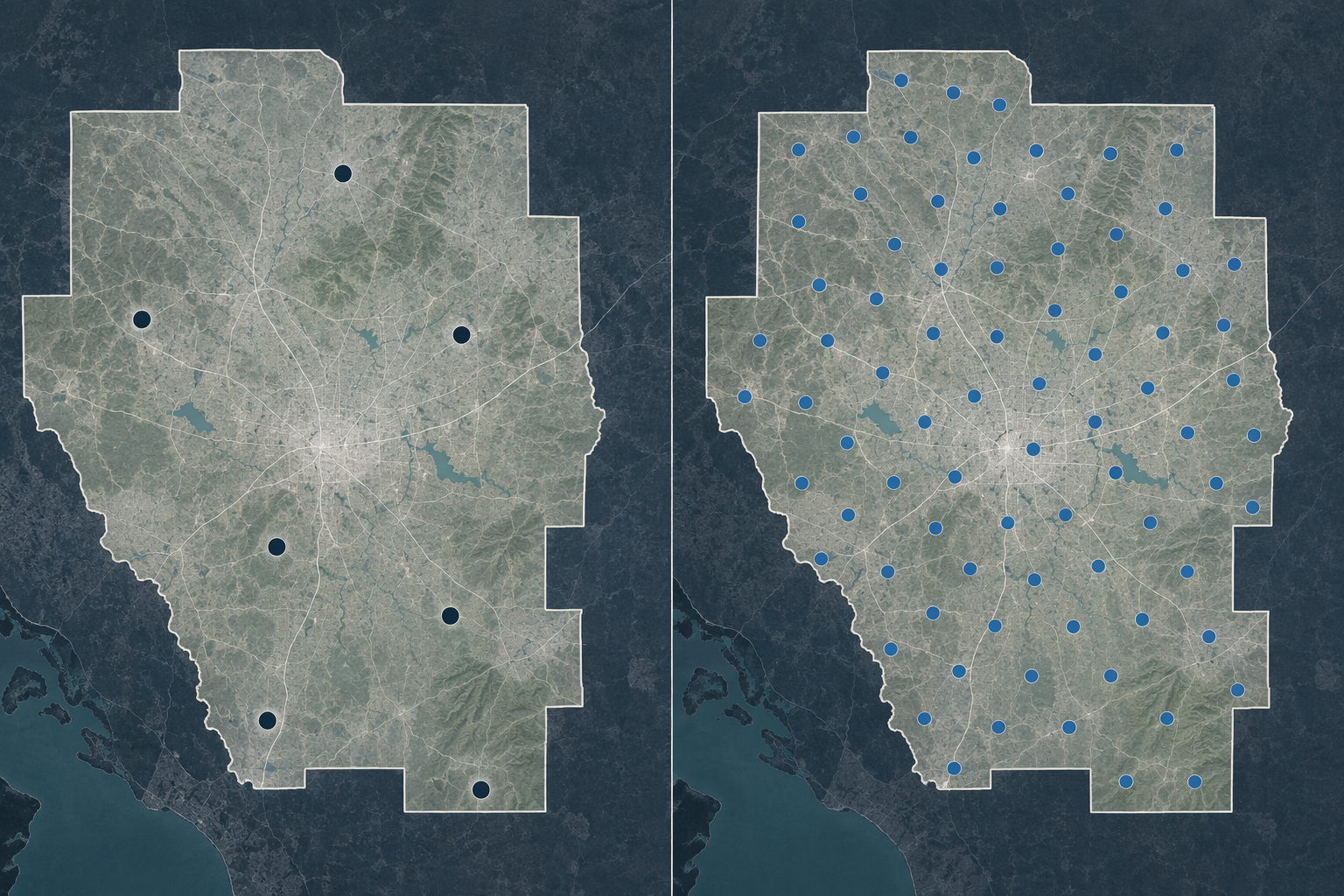
Regulatory monitors are still the backbone of official air quality surveillance. They are maintained to high standards, but they are expensive and sparse. That design works poorly when smoke plumes move unevenly across neighborhoods, valleys, school campuses, and commuting corridors. A single county-level value can be directionally correct and still fail the people deciding whether a specific clinic should extend hours or a specific school should cancel outdoor activity.
Low-cost sensors change the coverage equation. They can be deployed on campuses, rooftops, municipal facilities, and community sites at a density that regulatory networks usually cannot match. AI enters less glamorously than many product descriptions imply: the useful work is calibration, correction, quality control, and fusion with other data streams so that lower-cost measurements become stable enough for public decisions.
The distinction matters because not all sensor readings deserve the same confidence. Crowdsourced networks can provide valuable spatial visibility, but data quality varies when devices differ in siting, maintenance, humidity response, aging, and calibration. During a wildfire event, that variability is not an academic inconvenience. It can determine whether a public health team treats a local spike as a real exposure problem or as an instrument artifact.
This is where EPA-relevant testing and transparent calibration become more than vendor talking points. Clarity has reported that its Global V2.1 calibration model, tested through EPA-related evaluation, can match regulatory monitor accuracy within acceptable margins even during wildfire events.[5] That does not make every commercial claim equivalent, and it does not remove the need for local validation. It does mean some low-cost networks are moving from rough community awareness tools toward infrastructure that agencies can plausibly use in operational response.
| Monitoring Layer | What It Adds | Operational Caution |
|---|---|---|
| Regulatory monitors | High-confidence official measurements | Sparse coverage leaves many counties and neighborhoods without local data |
| Low-cost sensor networks | Dense local visibility across campuses, neighborhoods, and public facilities | Accuracy depends on siting, maintenance, calibration, and quality control |
| AI-calibrated networks | Correction and data fusion that can make dense networks more decision-ready | Clinical use still requires predefined thresholds, owners, and audit trails |
What “Hyperlocal” Looks Like When It Serves a Decision
Hyperlocal air quality data earns its keep only when it reaches someone who can do something with it. Two Southern California deployments show the difference between simply displaying more dots on a map and building a response surface for institutions that already have duties of care.
The Los Angeles Unified School District built one of the largest school-based air quality sensor networks in the country and expanded it after the January 2025 wildfires to include PM10 and NO2 detection.[5] A school-based network has a different value proposition from a consumer sensor on a private porch. It places measurements near children, staff, buses, playgrounds, and facilities teams. It can inform whether outdoor activity continues, whether buildings shift operations, and where district leaders need a more granular view than a regional AQI value.
South Coast AQMD’s gridded AQI map blends regulatory and sensor data to provide more localized reporting that can inform school closure decisions, outdoor activity restrictions, and targeted public health warnings.[5] The point is not that a gridded map is inherently clinical. It becomes clinically adjacent when public warnings are specific enough for health systems to identify which service areas, clinics, and patient panels are likely to feel the impact first.
A vague regional alert tells everyone to be careful. A reliable local signal can tell a pediatric practice which ZIP codes to prioritize for asthma outreach, a county team which shelters need filtration messaging, and a hospital command center which catchment areas may send more respiratory patients over the next shift. That is the meaningful version of hyperlocal: not a sharper map for its own sake, but a narrower queue of decisions.
Where AI Air Quality Data Enters Clinical Operations
The translation pathway from wildfire smoke measurement to clinical action is not automatic. It has to be designed. Real-time AQI or PM2.5 data must be linked to patient panels, risk tiers, staffing rules, communication templates, pharmacy processes, and surge triggers before the smoke event begins. Otherwise the dashboard becomes another screen someone checks while the emergency department fills.

Gould and colleagues described practical health system responses to wildfire smoke, including identifying high-risk patients, pre-filling rescue medications, expanding telemedicine access, and planning for surges.[4] Those actions are not interchangeable. Each one requires a different owner and a different tolerance for uncertainty.
- Patient stratification: respiratory clinics and population health teams can flag patients with asthma, COPD, heart failure, pregnancy, older age, or prior smoke-related utilization before a smoke event peaks.
- Medication readiness: pharmacies and clinicians can prepare rescue inhaler workflows where appropriate, with review steps that preserve clinical judgment rather than turning an AQI threshold into individual medical advice.
- Telemedicine expansion: ambulatory leaders can open additional remote slots when local smoke makes travel risky or when early respiratory symptoms are likely to rise.
- Surge planning: hospital operations teams can adjust staffing, respiratory therapy availability, call center scripts, and discharge coordination when high-exposure areas overlap with vulnerable patient populations.
The same environmental measurement can therefore trigger several workflows, but it should not trigger them all in the same way. A school closure threshold, a pharmacy outreach threshold, and an ED staffing threshold may draw from the same sensor network while requiring different lead times, approvals, and documentation. Treating them as one generic “smoke response” is how useful data gets flattened into an alert no one owns.
For health systems, the most defensible starting point is population-level decision support. AI-calibrated monitors can indicate that a service area is entering a higher-exposure condition. They cannot, on the evidence available here, determine that a specific patient will have an exacerbation tomorrow. That distinction matters legally, clinically, and ethically. Environmental forecasting is becoming operationally capable, while individual-level health-impact prediction remains a separate and less mature category; as covered in ClinicalMind’s piece on AI health-impact prediction for wildfire smoke and flooding, no FDA-cleared or CE-marked AI device exists for predicting individual health impacts from wildfire smoke.
A Threshold Is Not a Workflow
A clinically useful threshold has at least four parts: the environmental measure, the population affected, the action to be taken, and the accountable team. “AQI is unhealthy” is information. “When calibrated local PM2.5 exceeds the agreed level for this service area, the pulmonary clinic reviews the pre-identified high-risk asthma panel and opens same-day telemedicine slots” is a workflow.
The threshold also needs a stop rule. If smoke clears, who closes the outreach queue? If the sensor network flags a spike that is later corrected, who reviews whether messages or staffing changes were appropriate? If an alert goes to a school district, who confirms that indoor air conditions are actually safer than outdoor conditions? These questions are dull until they are missing.
This is where hospitals and public health agencies need auditability more than excitement. A smoke-response protocol should make it possible to reconstruct which data source triggered action, which patient group was included, who approved messages, and whether the action reached the intended population. Without that record, equity claims and quality improvement claims both become hard to test.
The Equity Paradox After the Network Is Built
Dense sensor networks can reduce the monitoring gap, but they can also reproduce it in a different form. If sensors cluster around wealthier households, better-resourced schools, and agencies with grant-writing capacity, the communities most exposed to smoke may remain undermeasured. Existing ClinicalMind coverage of AI sensor equity gaps in wildfire smoke monitoring notes that consumer sensor ownership can track wealth, including one California study in which sensor owners lived in homes valued about 21% above the median.
The operational fix is not to dismiss low-cost networks. It is to treat placement as part of the intervention. Public agencies and health systems should care where sensors are absent, not only where the map looks dense. A gridded display that still leaves farmworker housing, tribal areas, older rental stock, or unincorporated communities thinly covered may look modern while preserving the old burden of proof: residents feel the smoke first and get measured later.
Outdoor networks also do not measure the dose that matters most for every patient. People spend time indoors, buildings differ sharply in filtration and leakage, and a neighborhood outdoor reading may not describe exposure inside a classroom, apartment, shelter, or clinic. ClinicalMind’s analysis of why outdoor wildfire smoke monitors miss the real health impact covers this limitation in more detail, including evidence that indoor exposure metrics may explain asthma medication demand differently than outdoor metrics.
For clinical operations, that means outdoor AI air quality monitoring should be used as a community exposure signal, not as a patient-specific exposure measurement. It can help decide where to open outreach, where to prepare staffing, and where to coordinate with schools or public health partners. It should not be mistaken for proof of what any individual inhaled.
What Evidence Still Has to Prove
The evidence has moved far enough to make AI-calibrated low-cost monitoring operationally relevant, not speculative. The monitoring gap is large and inequitable. Wildfire smoke exposure carries measurable health risks. Calibrated sensor networks can add local visibility, and some platforms have reported performance close enough to regulatory monitors to be relevant during smoke events. School districts and air districts are already using dense networks to support more specific decisions.[1][2][3][4][5]
But adoption is not effectiveness. A hospital can connect local AQI feeds to an incident command dashboard, add thresholds to an EHR work queue, and create patient outreach scripts without yet knowing whether that integration reduces admissions, ED visits, or disparities. ClinicalMind has made the same point in its review of AI wildfire smoke forecasts and clinical readiness: the ability to forecast or monitor a hazardous exposure is ahead of evidence that deployment reduces hospital admissions.
AI-calibrated low-cost networks are now credible enough to close important monitoring gaps and support population-level clinical operations. What remains unproven is whether health systems can turn better smoke data into timely, equitable, auditable action before patients arrive in crisis.
References
- Roque et al., PNAS 2025, PNAS
- Assessing wildfire health risks, Stanford, 2025, https://news.stanford.edu/stories/2025/01/assessing-wildfire-health-risks
- Long-term exposure to wildfire-related PM2.5 and mortality: A nationwide cohort study in the contiguous United States, PNAS, 2024, https://www.pnas.org/doi/10.1073/pnas.2403960121
- Wildfire Smoke Exposure and Health: A Review of the Evidence, Annual Review of Medicine, 2024, https://pmc.ncbi.nlm.nih.gov/articles/PMC12183787/
- Webinar Recap: How Next-Generation Air Quality Monitoring Infrastructure Is Powering Wildfire Resilience, Clarity, 2026, https://www.clarity.io/blog/webinar-recap-how-next-generation-air-quality-monitoring-infrastructure-is-powering-wildfire-resilience
Comments
Join the discussion with an anonymous comment.