Wildfire smoke is usually measured outside, while many of the people most vulnerable to it are inside: in care facilities, clinics, apartments, schools, and homes with very different ventilation and filtration. That mismatch matters clinically. In a British Columbia study of care facilities, Coker et al. found that a 10 μg/m³ increase in machine-learning-predicted indoor PM2.5 during wildfire periods was associated with a 10.1% increase in salbutamol dispensations, while four outdoor PM2.5 metrics produced smaller 3.6–6.1% increases with non-overlapping confidence intervals.[1]
That is the important point here: not that an algorithm can draw a better smoke map, but that a better exposure estimate changes the apparent respiratory burden. Salbutamol is a rescue medication, so the signal is not just a modeled pollutant curve. It is a count of people needing short-acting bronchodilator relief after the exposure has already passed through a building envelope, an HVAC system, and whatever protection or leakage that particular place provides.

The old proxy was convenient, not clinically neutral
PM2.5 refers to fine particulate matter small enough to penetrate deep into the respiratory tract. During wildfire episodes, outdoor monitors and outdoor-modeled PM2.5 are indispensable: they make regional surveillance possible, support alerts, and allow epidemiologists to link air quality to health records at scale. But using outdoor concentration as the exposure for everyone quietly assumes that indoor exposure is either close enough or unknowable.
For respiratory epidemiology, that assumption is not harmless. A patient with asthma or COPD does not inhale the value at the nearest outdoor monitor. They inhale air that has entered a building, mixed with indoor sources, passed through filters or gaps, and changed with window use, air conditioning, maintenance, regional climate, and socioeconomic conditions. In a care facility, those differences can be systematic rather than random.
Coker et al. tested what happens when the exposure term is moved closer to the air people are likely breathing indoors. Their study trained machine learning models using data from 44 care facilities across British Columbia in 2022–2023, then linked predicted PM2.5 to salbutamol dispensations during wildfire periods.[1]
| Exposure metric | Respiratory outcome association |
|---|---|
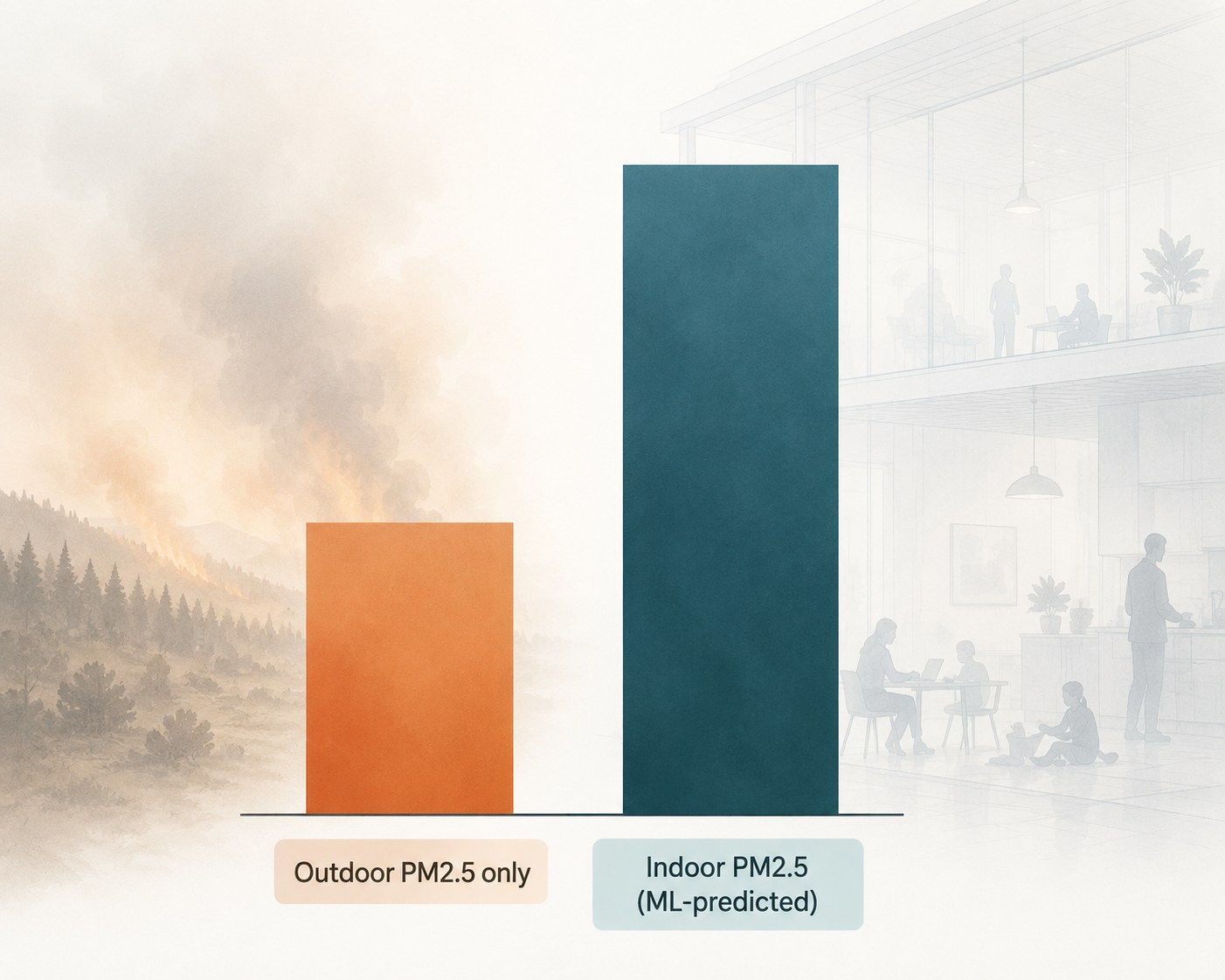
| ML-predicted indoor PM2.5 | 10.1% increase in salbutamol dispensations per 10 μg/m³ increase |
| Outdoor PM2.5 metrics | 3.6–6.1% increases in salbutamol dispensations per 10 μg/m³ increase |
The rough doubling is striking, but it should be read carefully. It is not a universal conversion factor for every wildfire study. It is evidence that, in this setting, outdoor-only exposure assessment materially diluted the estimated association between smoke-related PM2.5 and rescue inhaler use.
What the machine learning model actually corrected
The useful part of the AI here is unglamorous exposure work. Coker et al. used an ensemble of random forest, quantile random forest, and extreme gradient boosting tree models to predict indoor and outdoor PM2.5. The models were trained on low-cost sensor data from care facilities, outdoor sensor information, building characteristics, meteorology, and area-level deprivation indicators.[1]
The reported performance was respectable for a problem that is inherently noisy. The ensemble predicted indoor PM2.5 with an RMSE of 3.29 μg/m³ and R² of 0.71, and outdoor PM2.5 with an RMSE of 3.80 μg/m³ and R² of 0.78.[1] Those numbers do not make indoor exposure directly observed, but they show that the model captured enough structure to be epidemiologically useful.
One of the most telling details is that adding Canadian Index of Multiple Deprivation variables improved indoor PM2.5 prediction. The indoor model’s RMSE improved from 3.29 to 2.91 μg/m³, and R² increased from 0.706 to 0.769 when these area-level deprivation indicators were included.[1] That is not just a modeling footnote. It suggests that the indoor smoke environment is partly organized by social and infrastructural conditions, not only by outdoor concentration.
This is where machine learning earns its keep. A conventional regression model can adjust for deprivation as a covariate, but it may still leave the exposure itself mismeasured. In this study, deprivation information helped estimate the indoor pollutant concentration before the health model asked whether PM2.5 was associated with salbutamol use. That distinction matters. It moves deprivation from being only a statistical adjustment to being part of the exposure-generating environment.
Buildings changed the dose-response question
The indoor/outdoor ratio, often shortened to I/O ratio, is the hinge of the study. It compares indoor PM2.5 with outdoor PM2.5. If the ratio is close to 1, indoor concentrations are similar to outdoor levels. If it is lower, the building is reducing infiltration or otherwise lowering indoor concentrations relative to outside air. If it is higher, indoor levels exceed outdoor levels.
Coker et al. found that median I/O ratios dropped from 0.97 outside wildfire season to 0.82–0.83 during wildfire seasons.[1] That drop is exactly the kind of detail that gets lost when outdoor PM2.5 is treated as the exposure. During smoky periods, buildings did not simply mirror outside air. They modified it.
At first glance, a lower I/O ratio during wildfire smoke might sound reassuring: less outdoor smoke is getting inside. But for health-effect estimation, it also means the outdoor value is a poor stand-in for the concentration experienced indoors. If the same outdoor smoke event produces different indoor concentrations across facilities, then outdoor-only exposure collapses meaningful variation. That can attenuate the estimated relationship between smoke and respiratory medication use.
The regional differences sharpen the point. The study reported a median I/O ratio of 0.66 in Interior Health and 1.15 in Vancouver Coastal. The authors linked this variation with air-conditioning prevalence, noting 84% prevalence in Kelowna versus 16% in Victoria.[1] In plain terms, protection from outdoor smoke was not evenly distributed by geography. Some facilities appear to have had building systems and regional infrastructure that changed the indoor exposure more substantially than others.
That kind of heterogeneity is exactly why outdoor-only PM2.5 can be epidemiologically tidy and clinically misleading. Two facilities can share a regional smoke episode and still deliver different inhaled exposures to residents and staff. A model that treats the outdoor concentration as the exposure for both facilities may be precise about the wrong air.
Why the salbutamol result carries clinical weight
Salbutamol dispensations are not a perfect measure of symptoms. They are influenced by prescribing patterns, medication access, facility routines, and whether a person’s respiratory worsening is recognized and treated. But they are a concrete respiratory outcome, closer to clinical strain than an exposure map alone. A rise in dispensations during wildfire periods points to increased need for rescue bronchodilator therapy among people already vulnerable enough to be living in monitored care settings.
The contrast between indoor and outdoor estimates is therefore hard to dismiss as a technical curiosity. In the same study setting, the exposure metric that better approximated indoor air produced a 10.1% increase in salbutamol dispensations per 10 μg/m³ increase, while outdoor metrics produced 3.6–6.1% increases.[1] The non-overlapping confidence intervals are important because they suggest the difference was not merely a matter of noisy point estimates.
This also reframes what an “underestimate” means. It is not only that public health burden calculations may be too low. It is that the exposure-response relationship can be flattened before clinicians, health systems, and policymakers ever see it. If the exposure assigned to patients does not resemble the exposure that triggered medication use, the downstream estimate of harm becomes smaller by construction.
The broader smoke-risk context makes the measurement problem less academic
Accurate exposure assessment matters more when the pollutant source is especially harmful. Stanford researchers reported in 2025 that wildfire smoke is estimated to be about 10 times more toxic than PM2.5 from fossil fuel combustion, and they emphasized that there is no safe level of exposure.[2] That finding does not prove the British Columbia salbutamol association; it explains why underestimating wildfire-smoke exposure can have meaningful clinical consequences.
The supporting literature is still thin. Coker et al. note that only one prior study, Dong et al. 2020 in Chinese cities, similarly found that indoor time-weighted PM2.5 approximately doubled mortality effect estimates compared with outdoor-only models.[1] That is useful corroboration, not a settled evidence base. The strength of the BC study is that it shows the same general problem in a care-facility wildfire context with respiratory medication as the outcome.
Where this evidence should not be overextended
The study’s specificity is part of its value and part of its limit. The data came from 44 care facilities in British Columbia, primarily in three of the province’s five health authorities.[1] Care facilities have occupancy patterns, ventilation systems, maintenance practices, resident vulnerabilities, and medication routines that differ from single-family homes, schools, offices, and hospitals. A model trained in this context should not be treated as automatically portable to every indoor environment.
The indoor PM2.5 values were also predicted, not directly measured for every exposure assignment. That is an improvement over assuming outdoor PM2.5 equals personal exposure, but it is not the same as continuous direct indoor monitoring across all buildings. The right interpretation is methodological progress under real-world constraints, not complete elimination of exposure error.
The air-conditioning signal also cuts both ways. It helps explain regional I/O variation, which makes the model more believable. But it also means estimates may change as buildings are retrofitted, filtration improves, heat adaptation increases air-conditioning use, or residents change behavior during smoke events. Indoor exposure is a moving target because buildings and people respond to smoke.
Those caveats do not weaken the central result. They define where it can be used responsibly. The BC findings support the conclusion that outdoor-only PM2.5 models can understate respiratory effects during wildfire periods, especially when indoor exposure varies by building and region. They do not support a blanket claim that every wildfire-smoke health estimate should simply be doubled.
A better standard for environmental health AI
The most useful AI in this study did not diagnose asthma, predict an emergency department surge, or produce a new clinical score. It repaired a basic measurement problem: the exposure variable was outside, while the people were inside. By predicting indoor PM2.5 at population scale, the model changed the estimated association between wildfire smoke and rescue inhaler dispensations.
That should raise the bar for wildfire-smoke epidemiology. Outdoor PM2.5 will remain necessary, especially for surveillance and historical studies. But when the health outcome comes from people who spend most of the smoke episode indoors, outdoor-only exposure is no longer an innocent simplification. It is a source of misclassification that can make the respiratory burden look smaller than it is.
For clinical applications of environmental health AI, this is a more durable lesson than a headline about prediction accuracy. Health burden estimates are only as good as the exposure environment they actually model.
References
- Machine Learning-Based Indoor and Outdoor PM2.5 Exposure Assessment during Wildfire Smoke Events in British Columbia, Canada, ACS EST Air, 2024.
- Assessing wildfire health risks, Stanford University, 2025.
Comments
Join the discussion with an anonymous comment.