Amazon Health AI is easiest to misread if it is treated as another consumer chatbot with a medical vocabulary. The more important claim is architectural: Amazon describes a consumer-facing health agent built on Amazon Bedrock, separated into core agents, clinical sub-agents, auditor agents, and sentinel agents, rather than a single model answering health questions in isolation.[1] That distinction matters because most clinical harm in this category does not begin with a bad sentence. It begins when a plausible answer is accepted as a safe next step.
It is also not Amazon Connect Health. Connect Health is the provider-facing AWS product line aimed at contact centers, documentation, coding, and administrative workflow. Amazon Health AI, by contrast, is the consumer-facing agent that can respond to health questions, navigate care options, and connect users into Amazon’s clinical and pharmacy ecosystem.[1] Mixing the two makes the safety discussion muddy: a tool that helps a call center summarize an encounter carries a different risk profile from a tool that may decide whether a symptom needs urgent attention.
The Safety Claim Starts With Separation of Duties
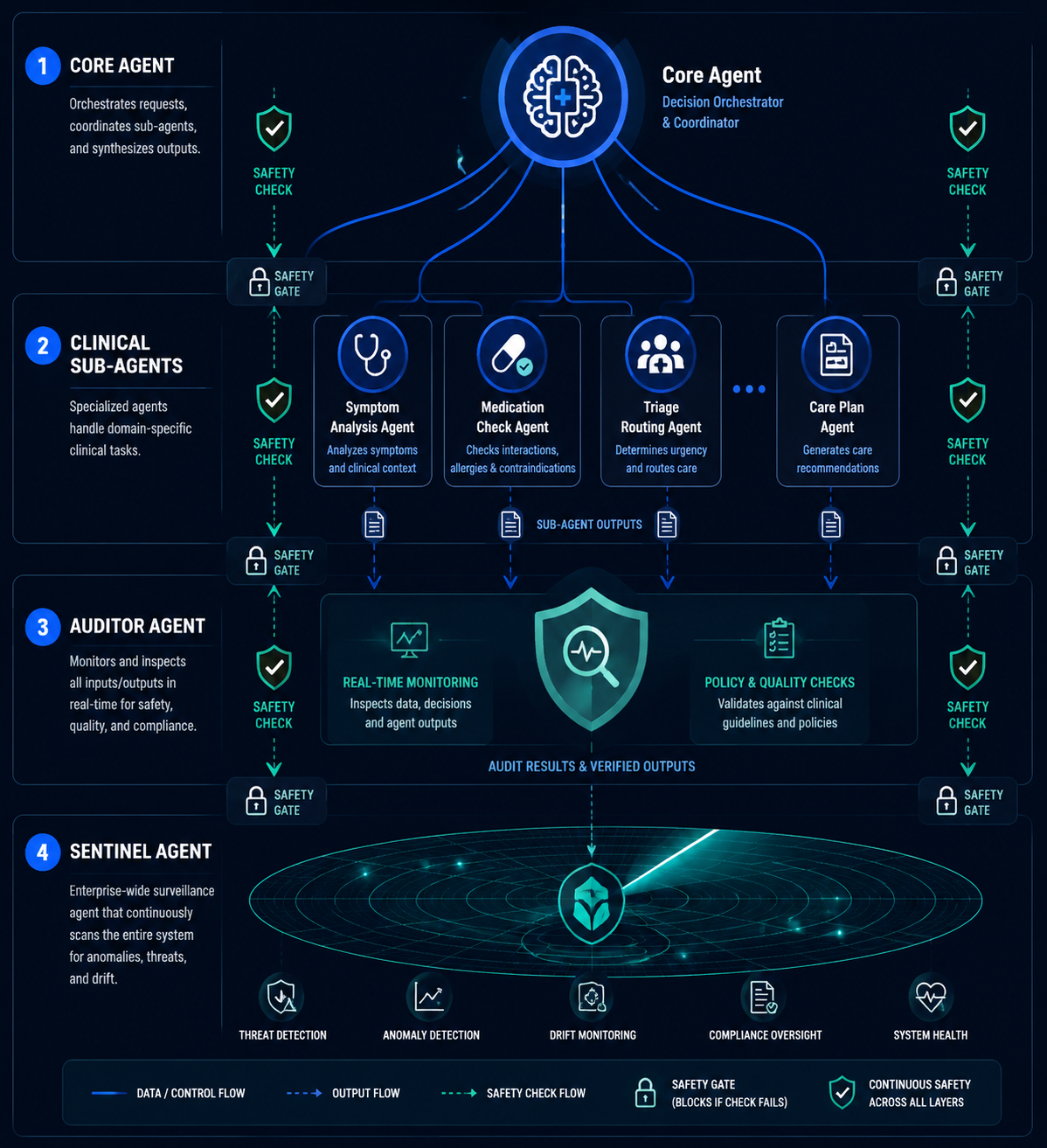
The design Amazon has described gives different agents different jobs. The core agent handles the consumer-facing interaction. Clinical sub-agents take on narrower tasks such as symptom interpretation, medication-related checks, or triage routing. Auditor agents monitor outputs in real time. Sentinel agents operate independently as system-level surveillance, watching for safety issues across the broader workflow.[1][2]
That may sound like engineering decoration, but in clinical workflow it is a meaningful design choice. A single-model assistant has to recognize the patient’s intent, generate the medical response, judge whether the response is safe, and decide whether a human should be pulled in. Amazon’s stated approach tries to avoid putting all of those responsibilities inside one conversational turn. If the patient says something that sounds like chest pain, self-harm, neurologic deficit, severe allergic reaction, medication toxicity, or another potentially time-sensitive problem, the safety burden should not depend only on the fluency of the answer.
| Layer | Stated role | Clinical question it is meant to answer |
|---|---|---|
| Core agent | Maintains the consumer-facing conversation | What is the user asking, and what response is being prepared? |
| Clinical sub-agents | Handle specialized health tasks | Does this symptom, medication issue, or routing decision require a more specific clinical pathway? |
| Auditor agents | Evaluate outputs in real time | Is the response safe enough to show, or should it be blocked, corrected, or escalated? |
| Sentinel agents | Monitor the system independently | Is there a broader safety pattern, failure mode, or surveillance signal that the active conversation layer may miss? |
The auditor layer is the part that deserves the closest reading. Amazon and coverage of the launch describe an LLM-as-a-judge pattern, where one model continuously evaluates another model’s clinical outputs.[2] In ordinary software review, this would be a checking service. In a health assistant, it becomes a clinical safety gate: the system is supposed to notice when an answer is too reassuring, too vague, or too confident for the facts the user supplied.
The sentinel layer is different. It is not just checking the next sentence. It is described as continuous surveillance that operates independently of the user-facing exchange.[1] In practice, that kind of layer could matter when the unsafe behavior is not obvious in one answer but becomes visible across repeated interactions: a class of symptoms being consistently downplayed, a medication warning being missed, or a routing rule behaving badly after a model or configuration change.
The useful question is not whether this architecture sounds safer than a plain chatbot. It does. The useful question is whether each layer has been tested against the failure modes it claims to catch, and whether those results are available to anyone outside Amazon and its partners.
Safety Is Also a Handoff Problem
Amazon’s more consequential move is not only that Health AI answers questions. It can route people into care. Public descriptions say the agent can escalate emergencies to 911, connect users to One Medical appointments, route prescriptions through Amazon Pharmacy, and refer patients onward to partner systems including Rush and Cleveland Clinic.[1][3]

That integration changes the clinical meaning of the product. A health information bot that says “talk to a doctor” leaves the burden on the patient. A system that can schedule with One Medical or route a prescription has the chance to close the loop. That is not a small operational advantage. In real care delivery, the dangerous gap is often between advice and completion: the patient who accepts reassurance, the patient who delays because the next step is unclear, the patient who cannot find an appointment, the patient who receives a recommendation but no route to act on it.
Operational closure, however, cuts both ways. If the AI over-escalates, clinicians inherit avoidable demand. If it under-escalates, the patient inherits risk. If it routes a prescription workflow cleanly but misses a contraindication or a symptom that should have changed the plan, the downstream system may look efficient while the clinical tail becomes messier. The cleaner the handoff appears to the user, the more important it is to know what safety gate approved it.
Amazon and One Medical have said the system has processed hundreds of thousands of real interactions, with only a fraction requiring clinician escalation.[3] That is an important deployment signal, but it is not the same thing as an audited safety result. “Only a fraction escalated” could mean the agent resolved many low-risk questions appropriately. It could also hide the denominator that matters most: how many encounters should have escalated, according to an independent clinical review.
What Amazon Says It Tested Before Launch
Amazon’s strongest evidence claim is pre-launch testing. The company and One Medical leadership have described a development process using thousands of synthetic clinical conversations, clinician-calibrated safety benchmarks, and a requirement that the AI meet or exceed clinician-level performance on safety-critical decisions before deployment.[4]
Taken at face value, that is the right category of testing. Synthetic conversations can stress a system with edge cases that are hard to collect prospectively: vague abdominal pain, mixed medication histories, symptoms that change halfway through the encounter, a user who minimizes danger, a caregiver asking for someone else, or a patient who says one alarming thing inside a mostly routine request. Clinician-calibrated rubrics are also preferable to generic answer-quality scoring because the key outcome is not whether the response sounds helpful. It is whether the next step is safe.
The missing pieces are the pieces a hospital safety committee, regulator, or serious purchaser would ask for first. Amazon has not published the test set, the rubric, the denominator of safety-critical cases, the definition of clinician-level performance, the composition of the clinician panel, inter-rater agreement, subgroup performance, escalation thresholds, or post-deployment audit results for Amazon Health AI specifically. As of July 2026, there is no independent peer-reviewed study of Amazon Health AI’s triage accuracy or safety performance.
That absence does not prove the system is unsafe. It does mean the public evidence is still mostly a vendor and partner account of how safety was engineered. Architecture can make a claim credible enough to examine. It cannot, by itself, verify the claim.
The Undertriage Problem Amazon Is Trying to Avoid
The category-level reason to care about these guardrails is undertriage. A Mount Sinai study in Nature Medicine evaluating ChatGPT Health found 52% emergency undertriage in the tested scenarios.[5] That finding is not evidence about Amazon Health AI. It evaluated a different system. But it is a sharp warning about the failure mode that consumer health agents must be able to prevent: a tool can sound medically fluent while recommending a level of care that is too low for the situation.
Amazon’s design appears aimed directly at that risk. Emergency escalation to 911, uncertainty-driven escalation to human One Medical providers, real-time output review, and independent sentinel monitoring all make sense as countermeasures.[1][2] The open question is whether they work under adversarial, ambiguous, and ordinary messy patient behavior. People do not present symptoms like board exam stems. They omit the medication that matters, answer “not really” to a red-flag question, or ask for reassurance because they have already decided they do not want to go to the emergency department.
A credible external evaluation would not need to show perfection. It would need to show how often the system escalates correctly, how often it fails to escalate, how often it over-escalates, and how those decisions compare with clinicians using a prespecified rubric. It would also need to report what happens after model updates, because a safety architecture that is valid in one release can drift in the next.
Trust Is Fragile Before the First Clinical Error
Consumer behavior is already ahead of consumer trust. KFF reported in March 2026 that 32% of U.S. adults had used AI for health information.[6] Pew Research reported in April 2026 that four in ten adults who used AI tools had uploaded personal medical data, while only 6% of U.S. adults said they trust AI health tools “a lot.”[7]
Those numbers do not say whether Amazon Health AI will be trusted. They do show the environment it enters: patients are willing to try these tools, some are willing to provide sensitive information, and very few grant deep trust. That combination is familiar in clinical informatics. Adoption can rise before governance catches up.
The data-access issue is not abstract. Reporting on Amazon Health AI has described integration with Health Information Exchanges through patient-authorized consent, under HIPAA.[8] If a patient authorizes access, an AI agent may be operating with a richer view of medical history than a generic chatbot ever had. That could improve relevance. It also raises a governance question that health information exchange networks are now having to confront: should AI agents access clinical exchange pathways in the same way treating clinicians do, and under what controls?
The Carequality debate belongs in that frame.[8] The issue is not whether patient-authorized exchange is inherently improper. The issue is whether authorization, identity, purpose of use, auditability, and downstream model behavior are specific enough when the actor touching the data is an AI-mediated service rather than a clinician sitting inside a traditional encounter.
The reported fictional disease injection issue, including the “bixonimania” example, should also be treated carefully.[8] It is not proof of an Amazon-specific clinical defect. It is a security and governance signal: if false or poisoned concepts can enter the information environment around AI health agents, safety monitoring has to include more than response review. It has to include provenance, retrieval controls, and a way to detect when the system is being steered by information that should never have clinical authority.
What Clinicians and Regulators Can Conclude in July 2026
Amazon Health AI deserves more precise scrutiny than generic chatbot anxiety. The product, as described, has a serious safety architecture: separation of duties across agents, output auditing, sentinel surveillance, emergency escalation, uncertainty-driven human handoff, and integration into actual care pathways. Those are the right kinds of design decisions for a consumer health system that may influence triage and access.
It also deserves less benefit of the doubt than the phrase “clinician-level” invites. Without a published rubric, methodology, test denominator, independent audit, or peer-reviewed evaluation, that claim remains internally asserted. A regulator or clinical governance group can acknowledge that Amazon built more than a medical FAQ bot while still refusing to treat the safety case as externally validated.
The strongest procurement question is therefore not “Is Amazon Health AI safe?” It is “Which safety claims have been independently tested, against which cases, with what escalation outcomes, and under what post-deployment monitoring?” Until those answers are public, the responsible conclusion is narrow: Amazon appears to have built a more safety-conscious consumer health AI architecture than a simple chatbot, and its vertical integration may reduce the gap between advice and care access, but the most important performance claims remain externally unverified as of July 2026.
Architecture can justify serious attention. Internal testing can justify cautious deployment. Independent validation is what turns a safety claim into evidence.
References
- Amazon announces new health AI features, About Amazon
- Amazon launches health AI agent with safety monitoring, CNBC
- Amazon Health AI routes patients to One Medical, Amazon Pharmacy and partner systems, Hit Consultant
- One Medical CMO discusses Amazon Health AI testing and clinician-calibrated safety benchmarks, MedCity News
- Conversational AI and emergency triage performance in healthcare, Nature Medicine
- KFF Health Tracking Poll March 2026: AI and health information, KFF
- Americans’ views of artificial intelligence in health and medicine, Pew Research Center
- Amazon Health AI, HIE consent and the Carequality data access debate, Second Opinion Media
Comments
Join the discussion with an anonymous comment.