An ambient AI scribe still looks, in mid-2026, like an administrative tool in the United States. It listens to a clinical encounter, drafts documentation, and leaves the clinician to review and sign. On that description, it generally sits outside FDA medical-device oversight. The difficulty is that many products no longer stop at passive transcription. They summarize, structure, infer, suggest codes, and in some implementations begin to resemble clinical or financial interpreters of the visit.
That boundary is not being treated the same way everywhere. A recent npj Digital Medicine perspective contrasts the U.S. position with NHS England guidance that subjects summarization-capable tools to regulatory scrutiny, precisely because a summary can change what a clinician sees, signs, and later defends.[1] The contrast matters: if summarization is treated as a regulatory signal in one mature health system, U.S. health systems should be careful about treating the same function as mere clerical convenience.
The relief these tools can bring is real. Documentation burden has been a corrosive force in clinical practice, and a well-designed ambient AI scribe can remove some of the typing, clicking, and after-hours note completion that distracts from the patient in the room. But a cleaner note is not automatically a safer governance model. The legal question is not whether the tool saves time. It is whether the health system can explain, after a disputed encounter, who created each part of the record, who reviewed it, what source material existed, what was retained, what was deleted, and whether the product crossed from recording into interpretation.
For the clinical outcomes debate, the evidence remains separate from the regulatory question. ClinicalMind has covered that gap in Ambient Intelligence in Healthcare: The Evidence Gap Between Vendor Claims and Clinical Reality. This piece takes the narrower compliance question: how should health systems govern a tool that is not currently regulated as a device, but is steadily moving toward functions that regulators, plaintiffs, payers, and patients may not view as administrative?
Where the Administrative Label Starts to Strain
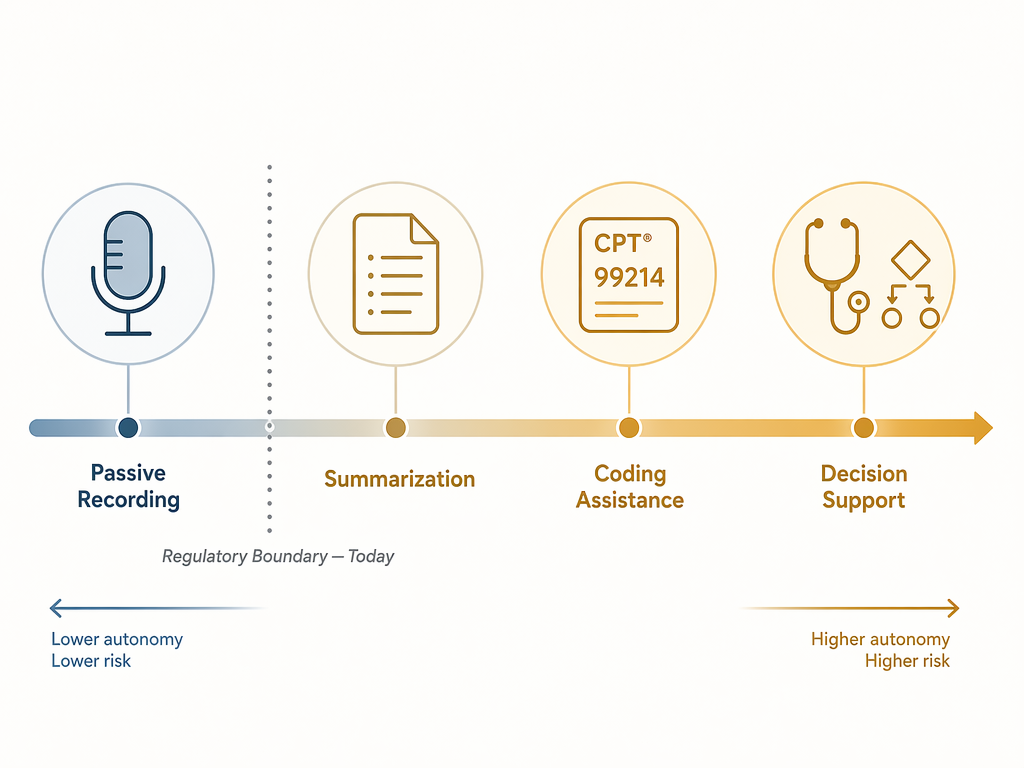
A passive recorder captures words. A transcription service converts speech to text. An ambient AI scribe usually does more: it identifies the likely structure of a note, compresses dialogue into findings, selects what seems clinically relevant, and places information under headings a clinician may later rely on. That is already more than a stenographic act.
Summarization is the first serious boundary problem. A summary omits, weights, and rephrases. If a patient says three things about chest discomfort and the generated note preserves only the least concerning version, the error may appear in the chart as a clinician-reviewed fact. If a negative statement is converted into an affirmative one, the defect is no longer a formatting problem. It has become a clinical record problem.
Coding assistance is the second pressure point. A suggested evaluation and management level, diagnosis code, or procedural code can turn a documentation tool into a reimbursement-risk tool. The issue is not only overbilling. A product may also encourage note elements that support a code without reflecting the clinical substance of the encounter. When the suggestion affects claims submission, the health system should assume compliance, audit, and payer scrutiny will follow.
Decision support is the third and most obvious line. If the product flags a possible diagnosis, suggests a differential, recommends a next step, or identifies missing care, the system is no longer merely documenting what happened. It is influencing what may happen next. Current non-device status should be treated as a starting condition, not as a permanent safe harbor.
| Function | Why it matters for governance | Practical question before deployment |
|---|---|---|
| Passive recording | Creates source material that may contain protected health information, sensitive statements, and potential evidence. | What audio is captured, retained, deleted, or available for audit? |
| Transcription | Converts speech into text and can introduce recognition errors, especially with accents, overlapping speech, or noisy settings. | Who verifies the transcript and is the intermediate transcript retained? |
| Summarization | Selects, omits, and rephrases information that may later become part of the signed medical record. | Can the system show what source dialogue supports each generated statement? |
| Coding assistance | Affects reimbursement, audit exposure, and false-claim risk if suggestions are inaccurate or unsupported. | Are coding suggestions separated from clinical documentation and subject to billing review? |
| Clinical decision support | May influence diagnosis, treatment, referrals, or follow-up. | Has the tool crossed into functionality that requires a different regulatory and risk review? |
The Person Who Signs the Note Still Owns the Consequence
The most uncomfortable fact in the current market is simple: no vendor has been identified in the available reporting as accepting clinical liability for AI-generated documentation errors, while the signing clinician remains legally responsible for the note. MedCity News, citing an ABA discussion, also reports that no precedent case law yet resolves liability for AI documentation errors.[2] That is not proof that every contract says the same thing. It is a warning that health systems should not assume liability has been solved somewhere in the sales cycle.
The signing clinician is not a ceremonial reviewer. In malpractice, licensure, payer, and medical-record disputes, the signed note is treated as the clinician's representation of the encounter. If the AI-generated note says the abdomen was nontender, the medication list was reconciled, or return precautions were discussed, the question later will not be whether the model was busy. The question will be why the clinician signed it.
That does not mean every clinician must reread every sentence with forensic suspicion. It does mean the health system must define the review obligation in a way that matches the product's function. A tool that drafts a simple follow-up note may justify one review standard. A tool that summarizes complex symptoms, imports outside data, or suggests billing codes requires a more explicit review protocol.
- The contract should identify whether the vendor disclaims clinical responsibility, limits damages, indemnifies only for technical failures, or accepts any responsibility for generated content.
- The policy should state that the clinician's signature applies to the final note, not to unreviewed intermediate outputs.
- The workflow should distinguish clinical note review from coding review when the product suggests charge-related information.
- The audit plan should sample notes for clinically material omissions and additions, not only turnaround time or user satisfaction.
A familiar trap is to bury this in training: clinicians are told to review the output, and the organization treats that instruction as a control. Training is necessary, but it is not enough. If a clinic schedules visits so tightly that careful review is unrealistic, or if the interface makes source verification difficult, the health system has created a foreseeable failure mode while documenting that someone else should have caught it.
Consent Is Not a Preference Setting
Ambient AI scribes depend on capturing the visit as it happens. That makes patient consent a legal and ethical design issue, not a front-desk courtesy. The available literature describes fragmented consent requirements across states, with models ranging from notice to opt-in and opt-out approaches, while two-party consent jurisdictions add another layer of complexity for audio recording.[1] No single national script can safely answer that variability.
The harder cases arrive quickly. A patient may lack capacity. A minor may be accompanied by a parent for part of the visit and seen alone for another part. A behavioral health visit may include disclosures the patient would not expect to be processed by a third-party model. An interpreter may participate. A family member may speak in the room. A patient may agree to documentation assistance but not to retention of raw audio.
Consent language should say what the tool does in ordinary terms: whether the visit is recorded, whether audio is stored, whether a transcript is created, whether a vendor processes the information, whether the patient may decline without losing care, and whether the clinician will review the final note. It should not hide the operative facts behind a generic reference to artificial intelligence.
| Consent issue | Governance decision |
|---|---|
| Jurisdictional variation | Maintain state-specific consent rules rather than a single national default. |
| Two-party consent states | Confirm whether the audio capture workflow satisfies applicable recording laws before deployment. |
| Opt-in versus opt-out | Document which model applies by site, specialty, and visit type. |
| Patients unable to consent | Define when surrogate consent is required and when the tool must be disabled. |
| Sensitive encounters | Identify visit categories where ambient capture is restricted or requires heightened notice. |
The operational temptation is to make the default as frictionless as possible. That may be defensible in some settings. But frictionless is not the same as lawful, and it is not the same as trust-preserving. A patient who discovers after the fact that an encounter was captured and processed by a vendor will not be reassured by the argument that the tool was only administrative.
The Data Trail Matters Before There Is a Dispute
Data governance is where many ambient AI scribe programs look tidy on a slide and less tidy in discovery. The npj Digital Medicine perspective and AHA market discussion both identify unresolved questions around raw audio retention, intermediate transcripts, provenance, and cloud processing arrangements.[1][3] Those are not technical details to be delegated after procurement. They determine whether the organization can reconstruct what happened.
Raw audio is especially consequential. If retained, it may become discoverable, subject to access requests, or relevant to internal investigations. If deleted, the organization must know when, by whom, under what policy, and whether deletion is consistent with record-retention obligations and litigation holds. A vendor's promise that audio is not kept after note generation may be attractive, but the health system still needs to know whether any temporary copy, cache, derived transcript, quality sample, or model-improvement artifact exists.
Intermediate transcripts deserve the same attention. A final note may be polished and clinically plausible. The transcript may show that the model missed a qualifier, confused speakers, or omitted a concern. If the transcript exists long enough to support review, it may also exist long enough to become evidence. If it does not exist, the health system loses one way to test the accuracy of the generated note.
Provenance logging is the practical answer to many of these problems. The record should be able to show whether text was generated by the scribe, edited by the clinician, imported from another system, or added by a coder or staff member. This is not about branding AI text with a scarlet letter. It is about knowing which human reviewed which machine-generated statement before it became part of the legal medical record.
- Require a data-flow diagram showing where audio, transcript, generated note text, metadata, and logs are created and stored.
- Specify retention and deletion periods for raw audio, temporary audio, intermediate transcripts, generated drafts, and audit logs.
- Confirm whether any data is used for model training, product improvement, quality review, or benchmarking.
- Review cross-border cloud processing and subcontractor chains under the business associate agreement and any applicable state or international requirements.
- Define litigation-hold procedures before the first adverse event, complaint, or payer audit.
Cross-border processing should not be treated as a procurement footnote. If protected health information moves through cloud infrastructure outside the expected jurisdiction, the business associate agreement, subcontractor terms, security review, and patient representations all need to match the actual data flow. Counsel should not first learn the architecture from a vendor engineer during an incident response call.
Bias Testing Has to Reach the Exam Room
Ambient AI scribes can fail unevenly. The npj Digital Medicine perspective flags the risk that large-language-model-based scribes may underperform for patients with non-standard dialects or accents because training data may be opaque or insufficiently representative.[1] That risk is easy to acknowledge in a policy statement and harder to test in a clinic where background noise, overlapping speakers, interpreter use, and specialty jargon all affect performance.
The fairness issue is not limited to whether a word is transcribed correctly. A model may compress a patient's narrative differently depending on speech pattern, language switching, or conversational style. It may assign less specificity to symptoms described through an interpreter. It may make a confident summary out of an uncertain exchange. These are documentation errors, but they can also become quality, access, and civil-rights problems if they systematically affect particular patient groups.
A health system does not need to solve model fairness in the abstract before piloting an ambient AI scribe. It does need to test the product in the actual populations and settings where it will be used. A dermatology clinic, emergency department, primary care practice, and behavioral health service do not produce the same audio environment or the same documentation risk.
- Sample generated notes across accents, dialects, interpreter-mediated visits, and noisy clinical settings.
- Track clinically material omissions, speaker attribution errors, negation errors, and unsupported additions.
- Require vendors to disclose known performance limitations, even when training data cannot be fully disclosed.
- Create a patient and clinician complaint pathway specific to ambient documentation errors.

How Evaluation Frameworks Help Procurement Ask Better Questions
Evaluation frameworks are useful here only if they change the questions asked before signature. SCRIBE, CRAFT-MD, MedHelm, and RE-AIM are identified in the recent literature as structured ways to assess ambient scribe tools and implementation.[1] They should not become decorative appendix material. They should become procurement, compliance, clinical operations, and audit prompts.
A framework can force a health system to separate accuracy from adoption. A tool may be popular with clinicians and still produce unacceptable errors in certain visit types. It can reduce time spent documenting and still create weak provenance. It can generate readable notes and still be unsuitable for coding suggestions. Those distinctions matter because adoption is not effectiveness, and effectiveness is not legal readiness.
| Framework use | Question it should force |
|---|---|
| SCRIBE-style documentation evaluation | Does the generated note accurately reflect the encounter, including omissions, additions, attribution, and clinical relevance? |
| CRAFT-MD-style clinical assessment | Is the tool being evaluated in realistic clinical workflows rather than idealized demonstrations? |
| MedHelm-style benchmarking | How does performance vary across tasks, specialties, patient populations, and input conditions? |
| RE-AIM implementation review | Who is reached, who adopts the tool, how well it is implemented, and whether the organization can maintain controls over time? |
The better procurement record is not the one with the longest AI policy. It is the one that shows a specific product was evaluated against its actual functions: recording, transcription, summarization, coding assistance, decision support, or some combination of them. The evaluation should also show who approved each function. A legal department may be comfortable with transcription but not coding support. A compliance team may approve use in routine primary care but not emergency psychiatric evaluations. Those distinctions should be visible before deployment.
Hallucination Numbers Should Not Carry More Weight Than They Can Bear
Some reported hallucination figures for ambient AI scribes are circulating through secondary sources. MedCity News reports a 1% to 3% hallucination rate per note while citing a PMC article, and also discusses comparisons between AI-generated and handwritten documentation that require verification against the primary source before they should be treated as settled figures.[2] Those numbers may be directionally useful for concern, but they should not become the foundation of a health system's risk model without primary-source review.
For compliance purposes, the more important question is often not the average hallucination rate. It is the severity and detectability of the error. A fabricated normal finding, a missed red-flag symptom, a wrong medication instruction, or an unsupported billing element does not become acceptable because the overall error rate appears low. The control has to fit the harm.
Health systems should therefore measure their own deployment. They should define what counts as a clinically material error, who adjudicates it, how often samples are reviewed, and when a product is paused or limited to narrower use. Vendor-reported performance is useful background. Local error review is the governance control.
A Preparation Standard for Health Systems
Preparing for possible reclassification does not require predicting exactly what FDA will do or when. It requires building a file that would make sense if a regulator, plaintiff, payer, patient, or board committee later asked why the system treated the product as safe to deploy. That file should be specific enough to survive the product's evolution.
- Classify the product by function, not marketing label: recording, transcription, summarization, coding assistance, decision support, or another defined use.
- Document liability allocation, including vendor disclaimers, indemnities, limitation-of-liability clauses, and the clinician's review obligation.
- Adopt jurisdiction-specific consent workflows, including rules for two-party consent states, opt-in or opt-out models, incapacity, minors, interpreters, and sensitive visits.
- Map data flows for audio, transcripts, drafts, final notes, metadata, logs, subcontractors, and cross-border processing.
- Set retention and deletion rules before go-live, including how litigation holds override routine deletion.
- Require provenance logging that distinguishes generated text, clinician edits, imported material, and coding-related additions.
- Test performance across specialties, care settings, accents, dialects, interpreter use, and noisy environments.
- Create escalation rules for material errors, repeated error patterns, patient complaints, and functions that expand beyond the approved use case.
The approval pathway should also include a change-control trigger. If a vendor adds coding suggestions, new summarization features, automated quality prompts, or decision-support language, the implementation should return to review. Too many AI governance programs fail because the product originally approved is not the product being used six months later.
This is where health systems can avoid the worst version of future regulation. If federal guidance eventually draws a brighter line around summarization, coding, or clinical recommendations, an organization with contracts, consent records, retention rules, provenance logs, and audit results will have something to adapt. An organization that treated the ambient AI scribe as a background convenience will have to reconstruct its governance after workflows, expectations, and data trails are already embedded.
Waiting for federal guidance is itself a governance choice. It is a weak one. The legal record is being built now, in vendor terms, patient notices, clinician review habits, deletion settings, audit logs, and exceptions no one wanted to slow down long enough to name.
References
- Barriers and opportunities of scaling ambient AI scribes, npj Digital Medicine
- What Healthcare Leaders Should Know Before Implementing AI-Powered Documentation Tools, MedCity News, July 2026
- 6 Health Systems Enhancing Care Delivery with Ambient AI Scribes, AHA Market Scan, April 14, 2026
Comments
Join the discussion with an anonymous comment.