The July 2026 verdict out of North Carolina was not about an obscure diagnostic miss. It centered on a maneuver the plaintiffs said should never have been used during shoulder dystocia: fetal vertex rotation after the infant’s shoulder became impacted. A jury awarded $18.2 million after the child sustained permanent global pan-plexus brachial plexus injury, and the plaintiffs’ legal team framed the act as the “never maneuver.”[1]
That phrase is useful because it is blunt. It is also easy to overstate. “Never maneuver” is not a standardized obstetric category in indexed medical literature based on the available source material; it emerged from litigation. The safer way to use it is as a legal and patient-safety shorthand for a contraindicated action during a known emergency, not as if it were a formal clinical taxonomy.
Still, the case raises the question that matters for AI systems meant to detect childbirth complications and prevent a “never maneuver”: when a dangerous action or omission is already defined as outside protocol, can real-time clinical decision support catch the break before injury occurs?

The More Plausible AI Use Case Is Not Prediction Alone
Obstetric emergencies do not wait for a perfect model. Shoulder dystocia, preeclampsia, infection risk, fetal heart rate deterioration, hemorrhage risk, and medication decisions all unfold inside rooms where the record may lag behind the bedside and the bedside may lag behind the guideline. A system that merely announces a risk score can be interesting and still fail the practical test: did it change what happened next?
That is why the Maimonides Medical Brain deployment deserves attention. According to the hospital’s institutional case study, Maimonides Medical Center began using AI in OB/GYN in 2018 and reported a reduction in obstetric never-event rates from 118 per 1,000 deliveries at baseline to approximately 11 per 1,000 deliveries over four years, across 28,300 births. The institution described this as a 91% reduction.[2]
Those numbers are large enough to take seriously and institution-specific enough to handle carefully. They do not mean an independently validated AI product has been proven to prevent 91% of obstetric injury in every labor unit. They mean one hospital reported a large decline in a defined set of monitored protocol failures after implementing a real-time surveillance and escalation system.
What Maimonides Actually Monitored
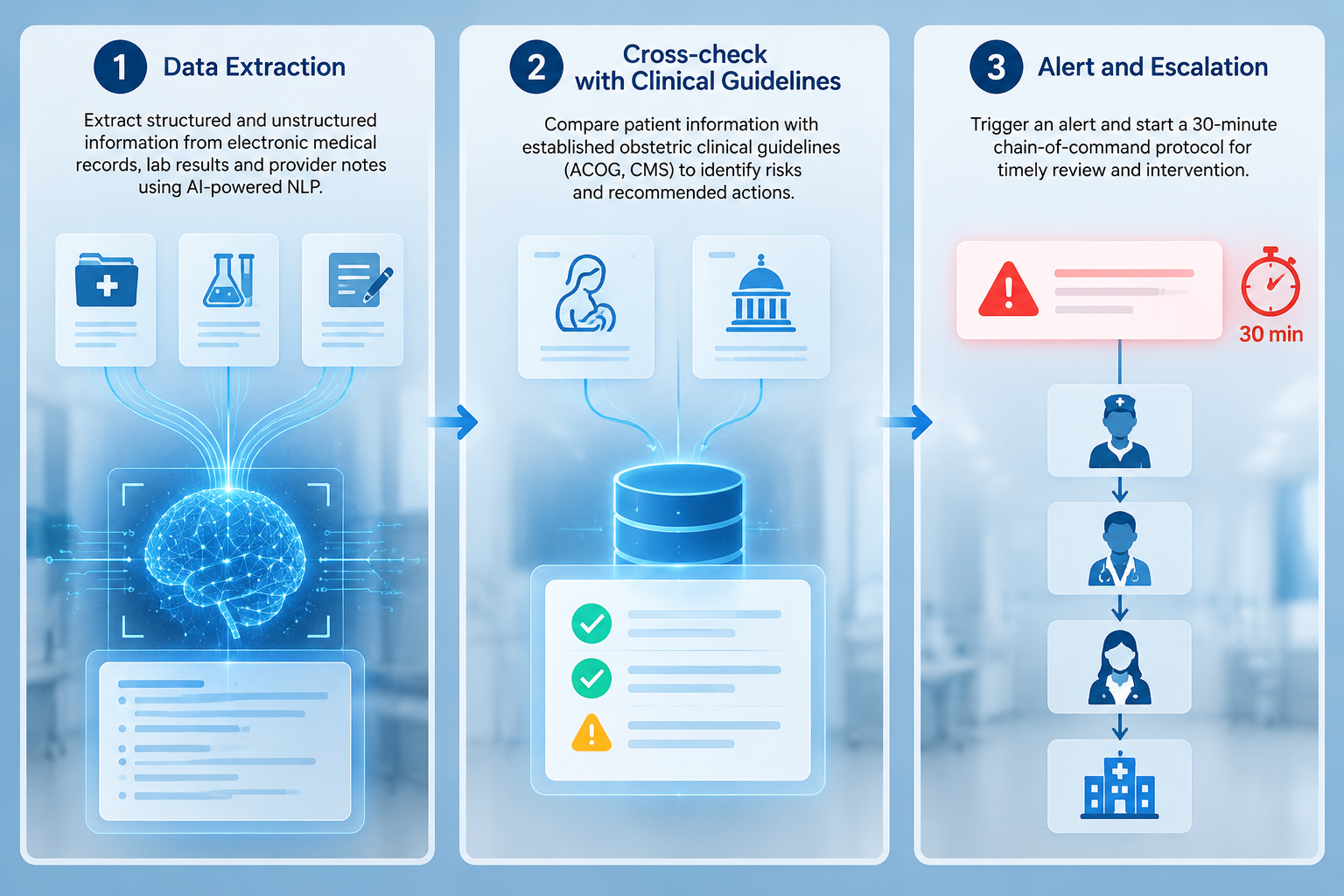
The most important detail in the Maimonides case is not that the system used AI. It is what the AI was asked to watch. The Medical Brain used natural language processing to extract information from electronic medical records, lab results, and provider notes, then cross-checked those data against ACOG and CMS-aligned rules for 11 obstetric never-event scenarios.[2]
The monitored scenarios included failure to administer group B strep antibiotics, omitted magnesium sulfate for preeclampsia, failure to discontinue Pitocin in the setting of non-reassuring fetal tracing, and contraindicated maneuvers during shoulder dystocia.[2] That list matters because it is different from asking a model to infer a rare complication from weak signals. The surveillance target is a gap between available clinical information and an expected protocol response.
| System task | Why it matters in labor and delivery |
|---|---|
| Extract relevant data from EMRs, labs, and provider notes | The trigger may sit in a lab result, a medication order, a note, or a fetal monitoring interpretation rather than in one clean field. |
| Compare the patient state with evidence-aligned rules | The system is looking for protocol mismatch, such as an omitted medication or a contraindicated action. |
| Alert clinicians when the mismatch appears | Detection has to reach the people who can still change the course of care. |
| Escalate if no response occurs within 30 minutes | A safety system that cannot move past an ignored alert is mostly documentation. |
The 30-minute escalation rule is not a small workflow detail. Maimonides reported that if no provider responded to an alert within 30 minutes, the system automatically escalated through a chain-of-command hierarchy.[2] In labor and delivery safety reviews, this is often where the preventability question becomes uncomfortable. The first missed cue may be clinical. The second is operational: no one with enough authority, bandwidth, or distance from the room intervened in time.
Detection Is Only Half the Safety Intervention
A contraindicated maneuver during shoulder dystocia is a vivid example because it concentrates attention on a single decision in a high-pressure room. But the larger safety pattern is broader. A missed antibiotic, an omitted magnesium sulfate order, or continued Pitocin despite a concerning tracing may not look dramatic at the moment it happens. The harm comes from the system allowing the mismatch to persist.
This is where protocol-compliance surveillance differs from ordinary clinical reminders. A reminder asks a clinician to consider an action. A surveillance-and-escalation loop asks whether the required response happened and, if not, who is now accountable for resolving the gap. That distinction is especially important in obstetrics, where hierarchy, handoffs, fatigue, and documentation lag can all delay escalation without anyone intending to be reckless.
The Maimonides baseline rate of 118 never events per 1,000 deliveries should also be read as a rate of monitored events under that institution’s definitions, not as a universal measure of catastrophic injury. The post-deployment rate of approximately 11 per 1,000 deliveries is likewise a reported rate inside the same local program.[2] The useful comparison is internal: before and after the surveillance system, using the institution’s never-event framework.
That internal comparison is still consequential. Across 28,300 births, a drop of that size suggests the tool was not merely adding another alert to an already noisy environment.[2] It suggests that the combination of real-time data extraction, protocol matching, and escalation changed behavior often enough to show up in operational results.
Where the “Never Maneuver” Fits
The WakeMed verdict gives the phrase “never maneuver” institutional force because it attaches a memorable label to a devastating outcome. The case involved fetal vertex rotation during shoulder dystocia and a permanent global pan-plexus brachial plexus injury, according to the plaintiffs’ announcement.[1] It is exactly the kind of event that prompts boards, insurers, and department chairs to ask whether the organization had a way to stop a known wrong action before it became a permanent injury.
An AI system would not make shoulder dystocia simple. It would not remove the urgency, the need for trained hands, or the burden on the team leader to choose the next maneuver. The narrower and more realistic question is whether the system can recognize that a documented or impending action conflicts with the protocol framework and bring that conflict to the right person fast enough.
That may sound modest compared with claims about autonomous diagnosis, but modest is an advantage here. Protocol surveillance does not need to discover a new physiology of childbirth. It needs structured and unstructured clinical data soon enough, rules clear enough to apply, alert routing strong enough to cut through hierarchy, and escalation serious enough that silence is not treated as resolution.
Not the Same as Fetal Monitoring AI
Some obstetric AI products focus on electronic fetal monitoring pattern recognition rather than protocol-compliance surveillance. PeriGen announced FDA 510(k) clearance in February 2025 for PeriGen Patterns 3.0, with the clearance expanded to 32 weeks, and describes PeriWatch Vigilance as a fetal monitoring support platform.[3] Those tools sit near the same clinical environment, but they answer a different question.
Pattern recognition asks whether a tracing shows concerning features. Protocol surveillance asks whether, given the available patient state, the care team has done something required or avoided something contraindicated. The first may help identify fetal distress. The second may help prevent the failure to act on information already present.
That boundary matters because fetal monitoring AI has its own evidence problems. A 2019 Cochrane review of computer interpretation of intrapartum electronic fetal monitoring found no improvement in neonatal outcomes.[4] That does not invalidate all AI in labor and delivery. It does warn against treating any promising obstetric AI result as proof that a broad category of tools improves babies’ outcomes.
The Wider AI Literature Supports Caution, Not Hype
A 2025 review of AI in obstetric emergencies summarized machine-learning approaches across shoulder dystocia, postpartum hemorrhage, fetal distress, and related emergencies. For shoulder dystocia prediction models, the review reported AUC values in the 0.79 to 0.87 range.[5] That is meaningful model performance, but it is not the same as showing fewer injured newborns after deployment.
This distinction is where many AI discussions in obstetrics become too loose. Adoption is not effectiveness. AUC is not bedside behavior. A flagged risk is not an escalated response. A single-center operational decline is not generalizable proof. Each measure can be useful, but only if it is kept in its lane.
The Maimonides report is therefore stronger than a model-performance paper in one respect and weaker in another. It is stronger because it is tied to actual births, operational alerts, and reported never-event rates over four years. It is weaker because the available evidence is institution-published, single-center, not independently peer-reviewed, and not a randomized controlled trial.[2]
What a Hospital Should Ask Before Buying
For a health system evaluating AI tools to detect childbirth complications and prevent a “never maneuver,” the procurement question should not start with whether the vendor says “AI.” It should start with whether the hospital can define the preventable failures it wants the system to catch.
- Which obstetric scenarios are monitored, and are they tied to current local, ACOG-aligned, or CMS-aligned protocols?
- Which data fields and notes does the system read, and how quickly after entry can it act on them?
- Who receives the first alert, and what happens if that person is scrubbed in, unavailable, or disagrees?
- What is the escalation interval, and does escalation reach someone empowered to intervene?
- How will the hospital measure success: alert response, protocol adherence, never-event rates, neonatal outcomes, maternal outcomes, or malpractice exposure?
- Who audits false positives, missed events, override patterns, and alert fatigue?
The last question is not administrative housekeeping. A system that repeatedly interrupts labor teams for weak alerts can train clinicians to ignore it. A system that misses the cases it was purchased to catch can create a false sense of safety. A system that escalates without clear governance can turn clinical disagreement into organizational noise rather than accountable review.
Maimonides’ reported 30-minute escalation structure is one answer to that governance problem.[2] Other hospitals may need different timing depending on staffing, in-house coverage, resident supervision, midwifery models, and EMR configuration. The point is not to copy the interval blindly. The point is that detection without an escalation pathway leaves too much of the safety intervention unfinished.
The Evidence Boundary
The Maimonides experience is a strong signal for replication. It is not a mandate for broad adoption. The reported 91% reduction came from a single institution’s own case study, using its own monitored scenarios, workflows, EMR environment, staffing patterns, and escalation culture.[2] Those features are not incidental; they are part of the intervention.
A replication study would need to show whether the same type of system works across hospitals with different documentation habits, different baseline event rates, different patient populations, and different willingness to escalate across hierarchy. It would also need independent outcome review, because a never-event rate is only as trustworthy as the definitions, capture method, and adjudication behind it.
That does not make the result easy to dismiss. Many clinical AI tools are built around prediction problems where the next step is uncertain. Protocol surveillance in obstetrics is a more disciplined target. It focuses on moments when the standard is already defined, the relevant data may already be in the chart, and delay or omission can be audited after the fact.
For the “never maneuver” specifically, AI should not be sold as a guarantee that no clinician will ever make a dangerous choice during shoulder dystocia. The defensible claim is narrower: a real-time system may reduce the chance that a contraindicated maneuver or omitted required intervention proceeds without detection, alerting, and escalation. That is still a serious patient-safety claim, and it deserves serious evidence.
The procurement-relevant conclusion is therefore restrained but not timid. AI protocol surveillance may be one of the more plausible clinical AI applications in obstetrics because it targets defined preventable failures rather than asking clinicians to trust a black-box prediction in isolation. Maimonides’ 91% reduction is a signal worth testing elsewhere, not a number that should be pasted into every hospital’s business case as if implementation alone will reproduce it.
References
- $18.2M Verdict for Child Injured by “Never Maneuver” During Delivery, Grant & Eisenhofer, July 14, 2026.
- Maimonides Medical Brain institutional case study, Maimonides Medical Center.
- PeriGen Patterns 3.0 FDA 510(k) clearance press release, PeriGen, February 2025.
- Computerised interpretation of fetal heart rate during labour for improving pregnancy outcomes, Cochrane, 2019.
- Artificial intelligence in obstetric emergencies, 2025.
Comments
Join the discussion with an anonymous comment.