Tourette syndrome advocacy often begins with an oddly difficult task: proving that something real happened when the person who lives with it may not tic on command, may suppress tics in public, or may have a quieter day during the appointment that is supposed to document need. Conservative estimates put Tourette syndrome prevalence at 0.3% to 1%, yet the condition remains widely misunderstood and underdiagnosed.[1] That gap matters in clinics, but it also follows families into school meetings, insurance appeals, workplace conversations, and public awareness campaigns.
The question behind ai for tourette syndrome awareness and advocacy is therefore not whether a new system looks impressive in a demo. It is whether AI-based tic detection can create records strong enough to help people explain a fluctuating, stigmatized condition to audiences that often want visible proof.

Why Measurement Becomes An Advocacy Problem
The Yale Global Tic Severity Scale remains the practical reference point for assessing tic severity. It is valuable because it gives clinicians a structured way to rate motor and vocal tics, impairment, frequency, intensity, complexity, and interference. Its weakness is not carelessness; it is the nature of the disorder. Tourette syndrome waxes and wanes, and a brief clinical observation plus patient or family recall can miss the pattern a parent has been trying to describe for months.[1]
That limitation becomes sharper outside the clinic. A student may tic intensely after holding it together through class. A family may ask for testing breaks or a low-distraction environment and be told the behavior was not observed. A clinician may write a careful letter, but the document still depends on narrative testimony and episodic assessment. In advocacy settings, the problem is not only whether symptoms exist. It is whether the record survives skepticism.
AI tic detection enters here as a measurement tool. The useful promise is not that an algorithm understands Tourette syndrome better than a clinician or patient. It is that video analysis, wearable sensors, and automated severity monitoring may capture tic frequency and patterns across longer stretches of time than a clinic visit can reasonably cover.
What The Detection Evidence Actually Shows
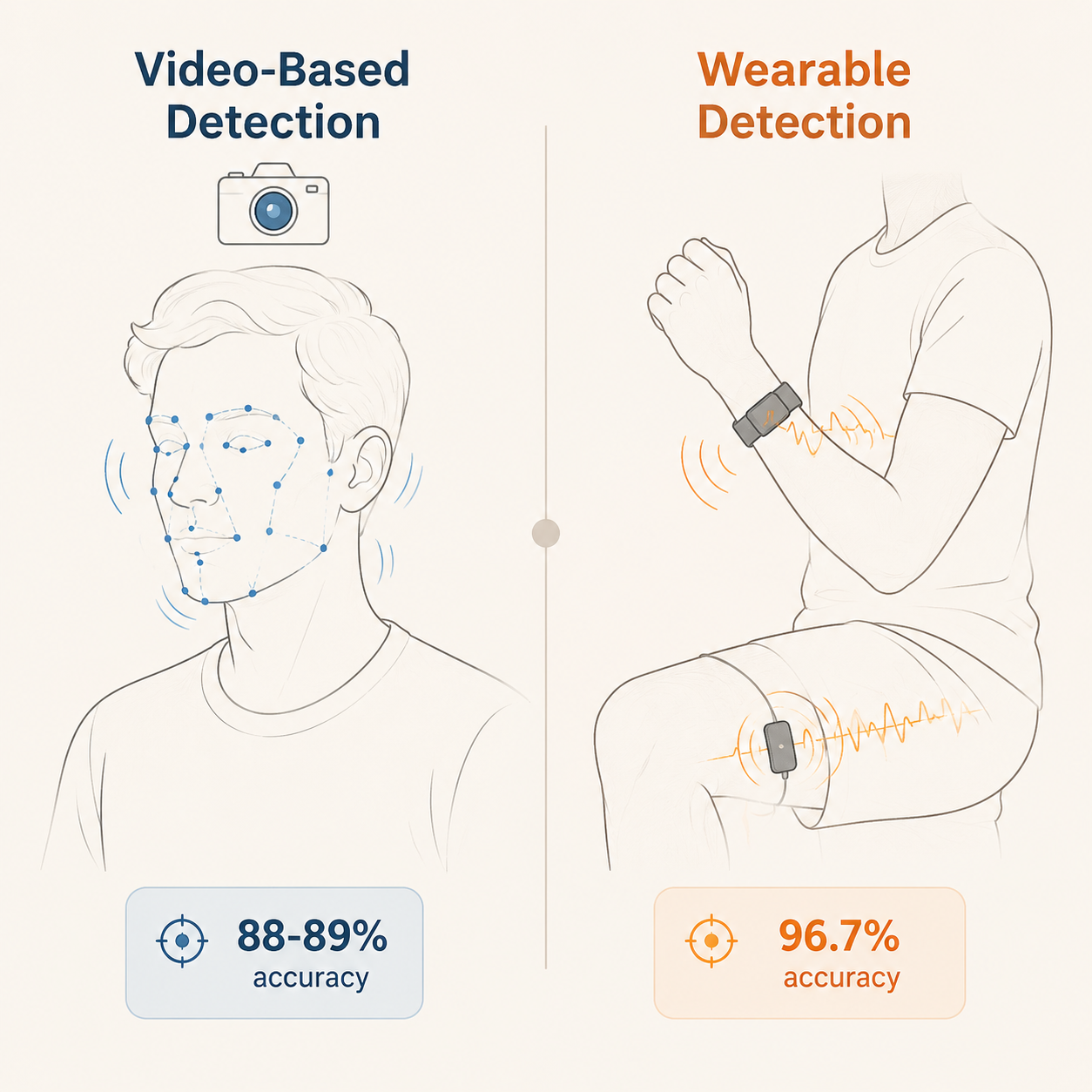
The performance numbers are no longer vague digital-health optimism. In 2023, Brügge and colleagues reported a machine-learning approach for automated motor tic detection using Random Forest classifiers, with an F1 score of 82% and accuracy of 88.4%.[2] In another 2023 video-based study, Wu and colleagues reported a deep neural network system for tic action evaluation with an F1 score of 79.5% and accuracy of 88.5%.[3] A 2022 wearable-sensing study by Cernera and colleagues found that surface electromyography combined with accelerometry differentiated tics from voluntary movements with 96.7% accuracy.[4]
| Approach | What It Measured | Reported Performance | What Advocates Can Reasonably Take From It |
|---|---|---|---|
| Video-based machine learning | Automated motor tic detection from recorded video | F1 82%; accuracy 88.4% [2] | Video can produce reviewable evidence of observed motor tics, especially when the dispute is whether a visible tic pattern occurred. |
| Video-based deep neural network | Tic action evaluation using a video-based system | F1 79.5%; accuracy 88.5% [3] | A second video approach reached similar accuracy, which strengthens confidence that the signal is not limited to one model design. |
| Wearable sEMG plus accelerometry | Differentiation of tics from voluntary movements | Accuracy 96.7% [4] | Wearables may help document movement events when video is impractical or too exposing, though the device itself can create visibility concerns. |
| Automated severity and digital monitoring | Longitudinal tracking and digital assessment possibilities | Synthesized in a 2026 digital health review [1] | The strongest advocacy use may come from patterns over time rather than a single detected tic. |
The Brügge and Wu studies are particularly useful because they point toward independent video routes to a similar place: automated detection that is accurate enough to be taken seriously, but not accurate enough to be treated as self-explanatory proof in every setting. An 88% to 89% accuracy range can support documentation. It cannot remove the need for clinical interpretation, context, or human review.
For awareness work, that distinction is important. A video-based system might help an advocacy organization show that tics are patterned, involuntary movements rather than jokes, habits, or deliberate disruption. It might help a clinician compare tic burden across days instead of relying only on what appears in the exam room. It might give a family a clearer way to show that symptoms intensify in certain environments. Those are plausible uses of the data. They are not the same as evidence that schools, insurers, or the public will respond differently once the data is shown.
Why Wearables Change The Evidence, And The Social Situation
The wearable result is the one that tends to make people sit up: 96.7% accuracy in differentiating tics from voluntary movements when surface electromyography was combined with accelerometry.[4] That pairing matters because movement alone can be ambiguous. Muscle activation data can add another signal, helping distinguish a tic-like movement from an intentional action.
Wearables also change the setting of measurement. A camera asks the person to be recorded. A wearable may follow the person through more ordinary activity. For longitudinal advocacy records, that could be valuable: a family does not have to rely on a five-minute clip, and a clinician could potentially review patterns across time rather than isolated episodes.
But a device worn at school or work can also expose what a person may prefer to keep private. It can invite questions, mark a child as different, or make tic monitoring feel like surveillance. Continuous data collection is not neutral just because the sensor is small. For a condition already vulnerable to teasing, disbelief, and misinterpretation, the social cost of measurement has to be part of the clinical and advocacy judgment.
The Small-Study Problem
The current evidence base is promising and narrow. Key tic detection studies involve small samples, in the range of 35 to 68 participants, and are often centered on facial motor tics in controlled recording conditions.[1][2][3][4] That does not make the findings trivial. It does mean the findings should not be stretched to cover full-body motor tics, vocal tics, complex real-world environments, or the full lived experience of Tourette syndrome.
A system trained and tested under controlled conditions may perform differently in a classroom, on a bus, during a panic-filled tic attack, or in a home where lighting, camera angle, clothing, and background movement vary. A child who suppresses tics in front of adults may produce a different data profile from a child whose tics are more visible in every setting. A person with vocal tics raises measurement questions that facial-motor datasets do not answer.
The cautious inference is still useful: AI systems can detect certain tic signals with enough accuracy to generate structured records. The unsupported inference would be broader: that these systems already capture Tourette syndrome comprehensively across everyday life. The second claim is where advocacy language can get ahead of the evidence.
From Tic Counts To School And Coverage Arguments
The most practical advocacy value is likely to come from longitudinal evidence. A single tic count may be less persuasive than a pattern: tics increasing during specific parts of the school day, clustering after periods of suppression, or interfering with handwriting, reading aloud, testing, sleep, or transitions. AI-generated records could make those patterns easier to summarize without forcing families to become full-time symptom archivists.
- For school accommodations, objective records could support requests for breaks, flexible testing arrangements, permission to leave class briefly, reduced penalty for tic-related disruption, or environmental adjustments.
- For insurance arguments, quantified symptom burden could help explain why assessment, therapy, or monitoring is medically relevant rather than optional.
- For clinician letters, longitudinal tic data could supplement exam findings and family reports instead of replacing either.
- For public education, carefully consented visualizations could show variability and involuntariness more clearly than stock images or oversimplified descriptions.
The word could is doing real work here. These are plausible advocacy applications based on better measurement, not proven outcomes. The available studies evaluated detection and monitoring performance; they did not test whether a school team grants accommodations more often after reviewing AI-generated tic data, whether an insurer changes a coverage decision, or whether a public campaign reduces stigma.

Awareness Campaigns Need More Than A Better Graphic
Objective tic data could improve awareness campaigns because Tourette syndrome is still flattened into caricature. Quantified movement patterns, time-based visualizations, and consented clips may help audiences see that tics fluctuate, can be suppressible for a time, and are not simply misbehavior. The 2026 digital health review frames digital tools as part of a broader opportunity in Tourette syndrome care and understanding, including monitoring approaches that can capture symptoms beyond brief clinical encounters.[1]
Still, awareness is not produced automatically by data. A graph can be ignored. A clip can be mocked. A dashboard can be misread as surveillance or as proof that only measurable tics count. Advocacy organizations would need to decide what is shown, who consents, how context is explained, and how to avoid turning children or adults with tics into educational exhibits.
The better use is not spectacle. It is explanation: showing variability over time, linking tic burden to functional consequences, and giving clinicians and families language that is harder to dismiss than “you had to be there.”
Privacy Is Not A Side Issue
Tic data is health data, behavioral data, and social data at the same time. Video can reveal a face, a classroom, a home, or a peer group. Wearables can reveal when symptoms worsen, where they happen, and how often. If the purpose is advocacy, the audience may extend beyond the clinical team to teachers, administrators, insurers, campaign staff, or the public. Each additional audience increases the chance that data collected to protect someone will be used to label them.
For children, the consent problem is especially delicate. A parent may want documentation to secure accommodations, while the child may worry about being recorded, watched, or singled out. A school may ask for proof but may not be equipped to store sensitive video or sensor reports responsibly. An insurer may welcome quantified data when it limits ambiguity, but families may reasonably worry about how long such data persists and who can access it.
Any advocacy use of AI tic detection needs minimum boundaries: collect only what is needed, explain who will see it, separate clinical records from public education materials, avoid identifiable footage when visualization will do, and give people with tics real control over whether their data is used beyond direct care or accommodation requests.
What Has Not Been Shown Yet
The evidence now supports a narrower and more useful answer than either hype or dismissal. AI-based systems can detect some tics with relatively high accuracy. Video approaches have reported accuracy around 88% to 89%, and a wearable sEMG-plus-accelerometry approach has reported 96.7% accuracy in distinguishing tics from voluntary movements.[2][3][4] These findings make objective longitudinal documentation a realistic direction for Tourette syndrome advocacy.
What has not been shown is whether that documentation changes the decisions advocates care about. No cited detection study demonstrates that educators grant better accommodations, insurers approve coverage more consistently, or public audiences develop less stigmatizing beliefs after seeing AI-generated tic data. The bridge from measurement to advocacy is logical, and in many rooms it may be badly needed, but it remains a bridge that has not been tested in real-world outcome studies.
Current AI tic detection appears accurate enough to strengthen the evidentiary foundation for Tourette syndrome awareness and advocacy. Its advocacy utility remains unproven until studies examine whether objective tic data changes accommodations, coverage, stigma, or public understanding in the settings where people with tics are actually judged.
References
- Digital health and Tourette Syndrome, Frontiers, 2026.
- Automated Motor Tic Detection: A Machine Learning Approach, Movement Disorders, 2023.
- Video-based evaluation system for tic action in Tourette syndrome, PMC, 2023.
- The Human Tic Detector, PubMed, 2022.
Comments
Join the discussion with an anonymous comment.