AI remote patient monitoring use cases are not a single evidence category. By Q3 2026, the strongest clinical case sits in cardiology, especially heart failure, hypertension, and arrhythmia detection. Diabetes and respiratory monitoring have credible but more uneven evidence. Post-surgical monitoring and neurology are still emerging. Mental health is the clearest boundary case: active development, substantial regulatory attention, and no FDA-authorized AI device with a mental health indication as of Q3 2026.
| Evidence tier | Specialties and use cases | What the evidence currently supports | Main caveat |
|---|---|---|---|
| Strongest | Cardiology: heart failure decompensation prediction, hypertension control, atrial fibrillation detection | Reduced readmissions or admissions in several RPM studies, sustained blood pressure control in digital therapeutic data, and clinically plausible alert-to-intervention workflows | Not every cardiac tool is the same kind of evidence; implementation claims and peer-reviewed outcomes need to be kept separate |
| Moderate | Diabetes: CGM-based hypoglycemia prediction, insulin optimization; respiratory: COPD exacerbation forecasting, sleep apnea screening | Earlier risk detection and some reported hospitalization reductions, with stronger support for sensor-based prediction than for fully autonomous optimization | Adoption, usability, and physiologic plausibility do not by themselves prove durable outcome improvement |
| Emerging | Post-surgical monitoring and neurology | Promising signals for surgical site infection detection, complication prediction, and EEG decision support | Evidence is more fragmented and less mature than cardiology |
| Thin / pre-evidence | Mental health NLP tools, chatbots, and generative AI monitoring | Development activity and regulatory scrutiny are increasing | No FDA-authorized AI mental health device as of Q3 2026, and outcome evidence remains limited |
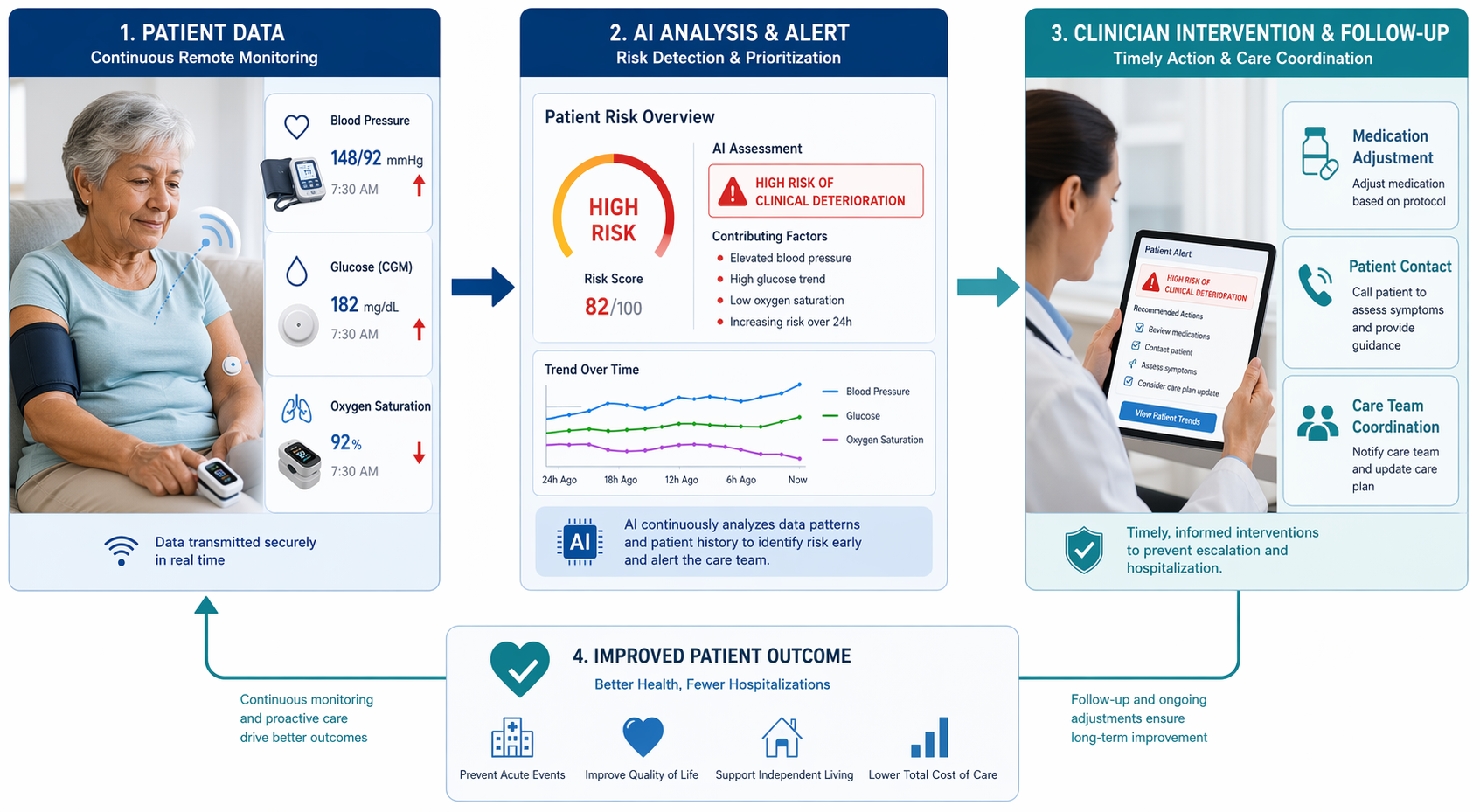
The useful dividing line is not whether a device uses a model. It is whether the model changes a monitored patient’s clinical pathway: an alert is reviewed, someone calls the patient, medication is adjusted, a visit is moved earlier, or an admission is prevented. A risk score that lands in an unstaffed queue is not yet remote care. It is a measurement waiting for a workflow.

What Counts as Stronger Evidence in AI-RPM
The better AI-RPM evidence usually has three features. First, it follows patients long enough to observe events that matter clinically, not only dashboard engagement. Second, it reports outcomes that a clinical team can recognize: hospitalization, readmission, length of stay, blood pressure control, hypoglycemia, exacerbation, or complications. Third, it makes the intervention visible. The model detected risk; the care team acted; the patient’s course changed.
A 2024 systematic review in npj Digital Medicine is useful because it pulls RPM evidence away from isolated product claims. The review included 29 randomized controlled trials across 16 countries and found consistent positive trends for patient safety, adherence, reduced hospital admission risk, and reduced length of stay, while quality-of-life measures were mixed. Its search ran through May 2023, so it does not capture newer studies published after that window.[1]
That distinction matters. A systematic review can show that monitored follow-up tends to help in certain settings, but it may not prove that a specific AI model, a specific alert threshold, or a specific vendor workflow caused the benefit. In AI-RPM, the model is only one part of a care delivery system.
Cardiology: The Most Developed Clinical Use Case
Cardiology deserves the most attention because the monitored signals are familiar, the deterioration pathways are clinically actionable, and the outcome measures are hard to ignore. Weight, blood pressure, heart rate, rhythm, symptoms, and device signals can all point toward a decision: adjust diuretics, intensify antihypertensive treatment, evaluate an arrhythmia, or bring a patient in before the next scheduled appointment.
Heart Failure: Prediction Only Matters When It Reaches the Nurse or Clinician in Time
Heart failure is the clearest example of AI-RPM becoming clinical rather than decorative. The useful claim is not that a model can classify a patient as high risk. The useful claim is that it can detect decompensation early enough for the team to intervene before the patient is short of breath, overloaded, and headed to the emergency department.
Large health-system data have shown a 38% hospitalization reduction, and a UMass Memorial implementation report described a 50% readmission reduction, with AI detecting deterioration 5–10 days before symptom onset and enabling preemptive diuretic adjustment. The UMass Memorial figure is clinically meaningful, but it should be read as a health-system press-release-based implementation claim rather than peer-reviewed trial evidence available at publication time.[2]
A CDC Preventing Chronic Disease meta-analysis published in September 2024 gives a broader, more conservative anchor. Across outpatient follow-up after heart failure, COPD, myocardial infarction, and stroke, remote follow-up for heart failure was associated with a 27% reduction in readmission risk, reported as an odds ratio of 0.73.[3]
Those findings are not interchangeable. A meta-analysis of RPM follow-up supports the value of structured monitoring after heart failure hospitalization. A health-system report of AI-enabled early detection supports a plausible and important operational model. A product-specific algorithm study would answer a narrower question. Health systems evaluating heart failure AI-RPM need all three views kept distinct.
Hypertension: Sustained Control Is the Outcome to Watch
Hypertension monitoring is less dramatic than heart failure decompensation, but it may be more scalable. A blood pressure signal is easy to collect at home, and treatment intensification is familiar. The hard part is maintaining control over years rather than producing a short-lived engagement curve.
The Hello Heart study published in JAMA reported 84% sustained blood pressure control over three years through an AI-driven digital therapeutic platform. The caveat is important: this is best described as evidence for a digital therapeutic using data analytics capabilities, not as a clean test of a stand-alone AI algorithm.[4]
For procurement, that caveat does not make the result irrelevant. It changes the question. The decision is not whether to buy “an AI model” for hypertension. It is whether the platform, coaching layer, measurement cadence, escalation rules, and clinician-facing reports produce durable control without creating an unsustainable review burden.
Arrhythmia and Cardiac Screening: Useful, but Not the Same as Managing Chronic Risk
Arrhythmia detection and cardiac screening are often grouped with RPM, but they operate differently from chronic heart failure monitoring. Atrial fibrillation alerts, low ventricular systolic dysfunction screening, and ECG-based risk tools may identify patients who need evaluation. They do not automatically create a longitudinal care pathway.
The Apple Heart Study, Samsung’s low ventricular systolic dysfunction algorithm screening 120,000 patients per month, and EchoNext ECG screening with 77% versus 64% accuracy are examples of how AI-enabled cardiac detection is moving into large-scale workflows.[5]
Here the main clinical question is downstream capacity. A positive screen needs confirmation, triage, counseling, and sometimes treatment. Screening accuracy is valuable, but the implementation succeeds only if the clinical system can absorb the newly identified risk.
Diabetes: Sensor-Rich, Clinically Promising, Still Uneven by Use Case
Diabetes has one of the strongest data streams in remote monitoring because continuous glucose monitoring produces frequent, clinically interpretable measurements. AI can be useful when it turns those streams into near-term hypoglycemia warnings, pattern recognition, or insulin dosing support. The evidence is stronger for prediction and decision support than for broad claims that AI independently improves all diabetes outcomes.
CGM-based systems can predict hypoglycemia 30–60 minutes ahead, which is a clinically meaningful window if the patient or care team can act. That type of forecast has a straightforward mechanism: warn early enough to prevent a low, reduce time in dangerous ranges, or change behavior before symptoms appear.
The Abbott Libre study published in May 2025 adds a different kind of outcome signal: reduced heart complication hospitalizations among monitored patients. It is important partly because the 2024 npj Digital Medicine review searched only through May 2023 and therefore could not include newer evidence of this type.[1][6]
AI insulin dosing optimization remains more delicate. A dose recommendation has a different risk profile from a risk notification. It requires tighter validation, clear accountability, and careful boundaries around automation. A diabetes educator reviewing trends is one workflow; a system that changes dosing logic is another.
Respiratory Monitoring: Plausible Early Warning, Harder Outcome Attribution
Respiratory AI-RPM sits in the moderate evidence tier. The clinical need is obvious: COPD exacerbations and sleep-disordered breathing often worsen outside the clinic, and patients may delay seeking care until symptoms have already escalated. The practical challenge is that respiratory status is noisy. Symptoms, oxygen saturation, activity, medication use, sleep, infection, weather, and comorbid heart disease can all move together.
COPD exacerbation forecasting 3–7 days ahead is promising because it resembles the heart failure logic: detect deterioration before the patient presents in crisis. AI-guided respiratory programs have reported 40–50% hospitalization reductions, but those figures should be treated as program-level signals unless the study design isolates the model’s contribution from nurse outreach, education, medication access, and enrollment effects.
Sleep apnea screening through AI-powered wearables belongs in the same broad respiratory category but answers a different question. Screening may identify people who need diagnostic testing; it does not by itself prove improved adherence to therapy, fewer cardiovascular events, or better daytime function. The evidence threshold should match the claim being made.
Post-Surgical Monitoring: Useful Signals, Early Evidence
Post-surgical AI-RPM has a compelling clinical story: patients leave the hospital earlier, complications evolve at home, and a wound image, temperature pattern, symptom report, or activity drop may reveal trouble before the scheduled follow-up. That does not yet put it in the same maturity tier as heart failure monitoring.
Reported surgical site infection AI detection sensitivity of 85–90% and complication-reduction ranges of 20–35% are encouraging. They are not enough, by themselves, to establish general deployment readiness across surgical services. Wound type, patient population, image quality, escalation pathway, and post-discharge staffing all affect whether detection becomes safer recovery.
This is a domain where the alert recipient matters especially. A flagged incision image may need same-day review. A vague recovery-risk score may not. The difference is not cosmetic; it determines whether the monitoring program prevents complications or simply documents anxiety after discharge.
Neurology and Mental Health: Where the Boundary Is Sharpest
Neurology has emerging AI-RPM activity, including tools such as an EEG AI co-pilot at Cleveland Clinic. The use case is credible: neurologic data are complex, longitudinal interpretation is difficult, and decision support could reduce review burden. But the available evidence described here does not yet support placing neurology beside cardiology in clinical maturity.
Mental health requires even stricter language. NLP-based chatbots, conversational tools, and generative AI monitoring systems are active areas of development, but they remain largely pre-evidence for the kind of clinical outcomes expected in mature RPM. As of Q3 2026, no FDA-authorized AI device has received a mental health indication.[7]
The FDA Digital Health Advisory Committee meeting in November 2025 formally evaluated generative AI mental health devices, which signals regulatory scrutiny rather than endorsement. That distinction should not be blurred. A technology can be important enough for regulators to examine and still not be mature enough for routine clinical deployment.[7]
Deployment Readiness Depends on the Alert Workflow
For health systems, the evidence map leads to a practical procurement rule: evaluate AI-RPM by specialty and workflow, not by the presence of AI in the product description. A heart failure tool that detects fluid overload 5–10 days before symptoms and routes the alert to a nurse who can arrange diuretic adjustment is a different clinical object from a chatbot that infers mood risk from language.
- For cardiology, ask whether the program has evidence for admissions, readmissions, blood pressure control, rhythm detection accuracy, or another measurable clinical endpoint.
- For diabetes, separate hypoglycemia prediction and CGM pattern analysis from more consequential insulin dosing automation.
- For respiratory care, examine whether reported hospitalization reductions come from the AI model, the care team intervention, or the combined program.
- For post-surgical monitoring, confirm who reviews flagged images or symptoms, how quickly, and with what authority to intervene.
- For mental health, do not treat development activity or regulatory discussion as evidence of authorized clinical performance.
The strongest AI remote patient monitoring use cases now have enough evidence to be treated as clinical deployment questions rather than speculative technology bets. That does not make the field uniform. Cardiology is ready for the most serious operational evaluation. Diabetes and respiratory monitoring deserve selective adoption with attention to the exact use case. Post-surgical, neurology, and mental health tools need sharper validation before they are described with the same confidence.
References
- npj Digital Medicine systematic review, npj Digital Medicine, 2024.
- UMass Memorial AI remote monitoring readmission reduction report, AJMC, October 2024.
- CDC Preventing Chronic Disease meta-analysis, Preventing Chronic Disease, September 2024.
- Hello Heart study, JAMA.
- Apple Heart Study; Samsung LVSD algorithm; EchoNext ECG screening evidence.
- Abbott Libre heart complication hospitalization study, May 2025.
- FDA Digital Health Advisory Committee meeting on generative AI mental health devices, FDA, November 2025.
Comments
Join the discussion with an anonymous comment.