The hard part of concussion return to play protocols is not usually naming the steps. It is deciding what to do with the athlete who has cleared symptoms at rest, looks normal in the training room, wants the next practice rep, and still has a recovery course that may not be finished. The standard approach remains deliberately cautious: the CDC HEADS UP progression moves through six steps, with at least 24 hours at each step, and the athlete advances only if symptoms do not return; if symptoms recur, activity stops and the athlete resumes at the previous asymptomatic step after rest. [1]

That protocol is not a loophole for automation. The Amsterdam 2022 international consensus statement keeps return to sport in the domain of clinical judgment, supported by serial assessment and supervised progression rather than a one-time clearance event. [2] The useful question for machine learning, then, is narrower than the marketing language often implies: where can a prediction model add information to a process that already exists?
Where Prediction Fits in a Graduated Protocol
A return-to-play pathway already produces repeated observations: symptom burden, exertional tolerance, vestibular or cognitive complaints, school or work function, sleep, headache recurrence, and sport-specific load. A model does not need to replace those observations to be useful. Its more defensible role is to flag which athletes are less likely to follow the uncomplicated path.
In practice, that means a machine learning output would sit beside the protocol rather than above it. If an athlete is predicted to have prolonged recovery, the next step is not automatic restriction from sport for a fixed period. It may be closer monitoring during aerobic progression, a more conservative schedule between stages, earlier referral for targeted rehabilitation, or a clearer conversation with the athlete, parents, coaches, and school staff about why a symptom-free day is not the same as full physiologic recovery.
The same logic applies after apparent clearance. A low-symptom athlete who reaches non-contact training still has to tolerate sport-specific load. A model that predicts elevated risk after concussion could help decide who needs closer neuromuscular assessment, strength and balance work, or trainer follow-up after the first game back. That is a different clinical use case from declaring someone eligible to play.

The Yates Model: Strong Numbers, Narrow Context
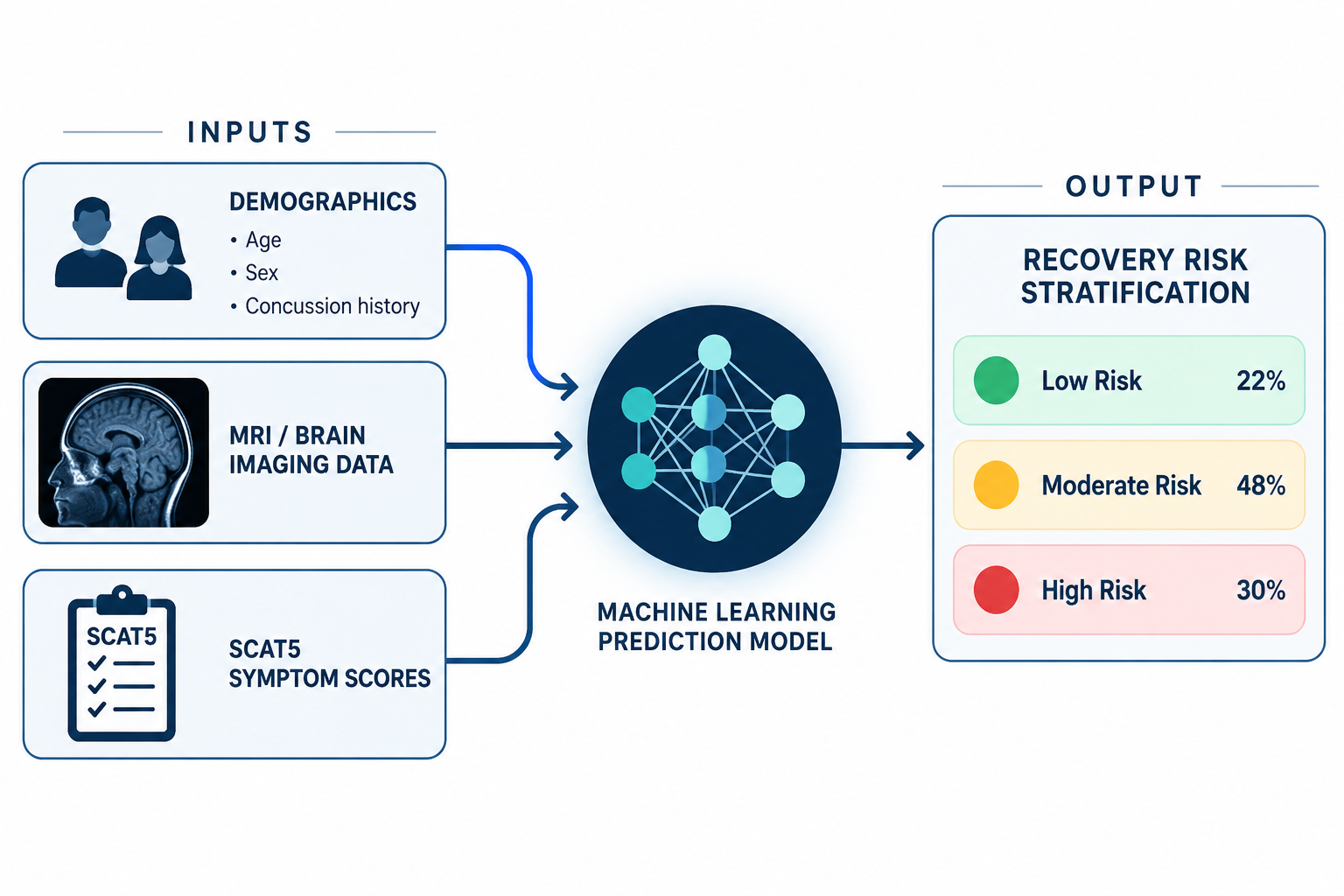
The most concrete example is the 2025 study by Yates and colleagues, which developed a multivariate model to predict concussion recovery in sportspeople. The investigators used demographics, MRI findings, and SCAT5 data in a single-center UK cohort of 375 athletes. Their random forest model predicted missing more than five games with 94.6% accuracy, 100% sensitivity, 93.8% specificity, and an AUC of 0.963. [3]
Those are clinically attention-grabbing results because the model is not just sorting athletes by one symptom score. It uses multiple streams of information that already matter in concussion care. A tool that is highly sensitive for prolonged recovery would be attractive in the clinic because the cost of missing a high-risk athlete is usually greater than the cost of slowing down a progression that later proves uncomplicated.
But the context matters as much as the percentage. The model was developed in one center, in a defined cohort, with a specific outcome: more than five games missed. [3] That outcome is relevant to return-to-play planning, but it is not identical to biologic recovery, school recovery, symptom resolution, or safe reintegration into contact sport. A model that predicts missed games may partly reflect medical factors, sport schedules, clinical culture, team policy, and competition timing.
This is the adoption problem in one sentence: impressive single-center performance is not the same as protocol-integrated decision support. Before a sports medicine program can rely on a model like this, it needs to know whether the same performance holds in a different clinic, with different scanners or documentation habits, across sports, ages, sexes, and competitive levels.
What a Model Output Could Change on Tuesday Afternoon
The most realistic use is not a red or green clearance button. It is a risk-stratified plan that changes the supervision around the existing steps.
| Protocol moment | What the clinician already checks | How a model could help |
|---|---|---|
| Initial post-injury assessment | Symptoms, exam findings, injury history, school or work tolerance | Estimate risk for prolonged recovery and set expectations early |
| Before aerobic progression | Symptom stability at rest and with daily activity | Identify athletes who may need slower exertional loading or earlier rehabilitation referral |
| Sport-specific exercise | Symptom recurrence with movement, coordination, and conditioning | Support closer trainer-clinician communication if predicted risk remains high |
| Non-contact and full-contact practice | Tolerance of higher-intensity sport demands | Prompt additional review before exposure to contact or collision |
| After return to sport | Ongoing symptoms, performance, pain, lower-extremity complaints | Flag athletes who may need post-clearance musculoskeletal monitoring |
That workflow also protects against a common misuse of prediction. If a model estimates low risk but the athlete develops headache or dizziness during sport-specific exercise, the protocol should still stop progression. Conversely, if a model estimates high risk and the athlete remains symptom-free through graduated exertion, the prediction should shape surveillance and counseling, not function as an unexplained veto.
For an athletic trainer, the value may be practical: who needs a same-day clinician call after exertion, who should be checked again after practice, and who should not be lost to follow-up once the schedule gets busy. For a physician, the value is a more structured risk conversation. Instead of saying only that recovery is variable, the clinician can explain which inputs pushed the athlete toward a higher-risk category, provided the model can show its reasoning.
Post-Clearance Injury Risk Extends the Question
Recovery duration is only one RTP-relevant outcome. Claros, Buckley, and Brockmeier reported a machine learning model for lower-extremity musculoskeletal injury risk in collegiate athletes after concussion, with 95% accuracy. Their work also found that lower-extremity musculoskeletal injury risk doubles after concussion and remains elevated beyond the initial return-to-play window. [4]
That finding changes the tone of the clearance conversation. If elevated injury risk persists after the formal RTP window, then “cleared” is too small a word for what the care team has to manage. The athlete may be allowed to return, but the trainer may still need to watch landing mechanics, fatigue response, cutting tolerance, strength asymmetry, or new lower-extremity symptoms. The administrator may see the case as finished; the clinical team should not.
This does not prove that every athlete needs a prolonged restriction after concussion. It supports a narrower and more useful conclusion: post-concussion monitoring should not end simply because the athlete has completed the steps and rejoined competition. A model that estimates post-RTP musculoskeletal risk could be useful precisely because the risk may show up after the celebratory moment.
Random Forest, XGBoost, and Explainability Without the Tutorial
The model names matter only insofar as they affect clinical trust. Random forest models combine many decision trees and can handle nonlinear relationships among variables such as symptoms, prior injury, imaging features, and functional assessments. XGBoost is another tree-based method that often performs well with structured clinical datasets. A 2026 systematic review of machine learning models predicting return to sport in athletes identified random forest and XGBoost among the top-performing approaches; in concussion studies, random forest achieved an AUC greater than 0.9 in two of four studies. [5]
The clinical issue is not whether a physician can describe the algorithm. It is whether the output is interpretable enough to discuss responsibly. SHAP and similar explainability tools can show which variables pushed a prediction higher or lower for a given athlete. That matters when a teenager and a parent are being told that the athlete is high risk despite feeling better, or when a coach asks why one athlete is progressing more slowly than another.
An unexplained probability is easy to overuse or ignore. An explained probability can be challenged. If the model leans heavily on an input that is missing, unreliable, or not applicable to the athlete in front of the clinician, that should change how much weight the prediction receives.
The Field Is Promising, but Still Thin in the Places That Matter
The broader literature supports cautious interest rather than routine adoption. Vecchiato and colleagues’ 2026 scoping review covered 55 studies across four artificial intelligence domains in sport-related concussion. The review reported that 10% to 20% of athletes experience prolonged symptoms, and that prognosis and recovery models show moderate-to-good performance, but the field remains limited by small samples, heterogeneous outcomes, and minimal external validation. [6]
The same review reported only 38% female representation. [6] That is not a footnote for a return-to-play tool. If a model is expected to guide care across schools, clubs, colleges, and professional settings, performance in underrepresented groups cannot be assumed from aggregate accuracy. A model that works best in the population that produced the training data may still fail the athlete sitting in the exam room.
There is also a diagnosis problem underneath the modeling problem. Concussion has no single gold-standard test, so training labels can reflect clinical judgment, documentation quality, and local practice. Machine learning can find patterns in messy data, but it cannot erase uncertainty baked into the labels it learns from.
For administrators evaluating a vendor, the right question is not only “What is the accuracy?” It is: accuracy for which outcome, in which cohort, with what missing data, against what reference standard, and validated where? A 94% or 95% figure may be real within a study and still not tell a clinic how the tool will behave across its own athletes.
What Protocol-Integrated Adoption Would Require
For machine learning to become part of concussion return to play protocols, the output has to be placed at named decision points. A model that predicts prolonged recovery at the first visit serves a different purpose from one that predicts musculoskeletal injury after return to sport. A clinic needs to know when the score is generated, who sees it, what action it can trigger, and what action it must never trigger by itself.
- External validation in independent cohorts, not only internal test performance.
- Prospective multicenter testing across sports, ages, sexes, and competitive levels.
- Clear outcome definitions, such as missed games, symptom duration, protocol completion, or post-RTP injury.
- Explainability that shows why an athlete was labeled high risk.
- Workflow rules for trainer-clinician handoffs, symptom recurrence, and documentation.
The workflow rule is not a minor implementation detail. If the score appears only in an electronic record after the athlete has already advanced through practice, it has little clinical value. If it appears without context, it may create pressure to act on a number no one can interpret. If it appears at the right moment, with an explanation and a defined response, it can make an already cautious protocol more individualized.
The safest use case today is conservative decision support: identifying athletes who deserve closer follow-up, slower progression, earlier rehabilitation, or post-clearance monitoring. The least defensible use is accelerating return because an algorithm labels an athlete low risk while symptoms, exertional response, or clinical judgment point the other way.
The Q3 2026 Readiness Level
Machine learning has moved beyond abstract promise in concussion care. Models have predicted RTP-relevant outcomes such as prolonged recovery, missed games, and post-concussion musculoskeletal injury risk with strong reported performance in specific cohorts. The Yates model is especially notable because it combines demographics, MRI, and SCAT5 data and reports unusually high discrimination for missing more than five games. [3]
As of Q3 2026, that is not enough for routine protocol-integrated adoption across diverse sports medicine settings. The current evidence supports machine learning as a promising decision-support layer for concussion return-to-play care, especially for identifying prolonged recovery and risk after return. It does not yet support replacing graduated progression, symptom-dependent stepwise monitoring, or clinician judgment.
References
- HEADS UP Returning to Sports and Activities, CDC, 2025.
- Consensus statement on concussion in sport: the 6th International Conference on Concussion in Sport-Amsterdam, October 2022, British Journal of Sports Medicine, 2023.
- Developing a multivariate model for the prediction of concussion recovery in sportspeople, BMJ Open Sport & Exercise Medicine, 2025.
- A machine learning model for post-concussion musculoskeletal injury risk in collegiate athletes, Sports Medicine, 2025.
- From injury to comeback: A systematic review of machine learning models predicting return to sport in athletes, 2026.
- Artificial intelligence applications in sport-related concussion: an updated scoping review, Journal of Science and Medicine in Sport, 2026.
Comments
Join the discussion with an anonymous comment.