Market Growth vs. Clinical Reality: The Adoption-Investment Gap
The numbers are striking. The global conversational AI healthcare market is projected to expand from $13.68 billion in 2024 to $106.7 billion by 2033, according to industry analyses. This trajectory places conversational AI among the fastest-growing segments in health technology. Yet the same reports reveal a stark disconnect: 56% of healthcare leaders plan to invest in generative AI over the next two to three years, but only 19% of medical practices have adopted even basic conversational AI technology. The gap between investment intent and deployed reality is not a lag — it is a signal.
This pattern repeats across clinical AI more broadly. A cross-sectional survey of 43 U.S. health systems conducted in Fall 2024 found that while 100% of respondents reported adoption activities for ambient AI notes — a generative AI tool for clinical documentation — only 19% reported high success with AI for clinical diagnosis, and 38% for clinical risk stratification. The survey, published in BMC Digital Health, drew responses from organizations predominantly operating with net patient revenue exceeding $1 billion — the segment best positioned to absorb the cost and complexity of AI deployment.
The implication for health system decision-makers is clear: the market is moving faster than the evidence base. Investment enthusiasm is outpacing the clinical validation needed to justify broad deployment. Understanding where the evidence stands — and where it does not — is the first step toward responsible adoption.
FDA Regulatory Status: 1,451 Authorized Devices, Zero Generative AI
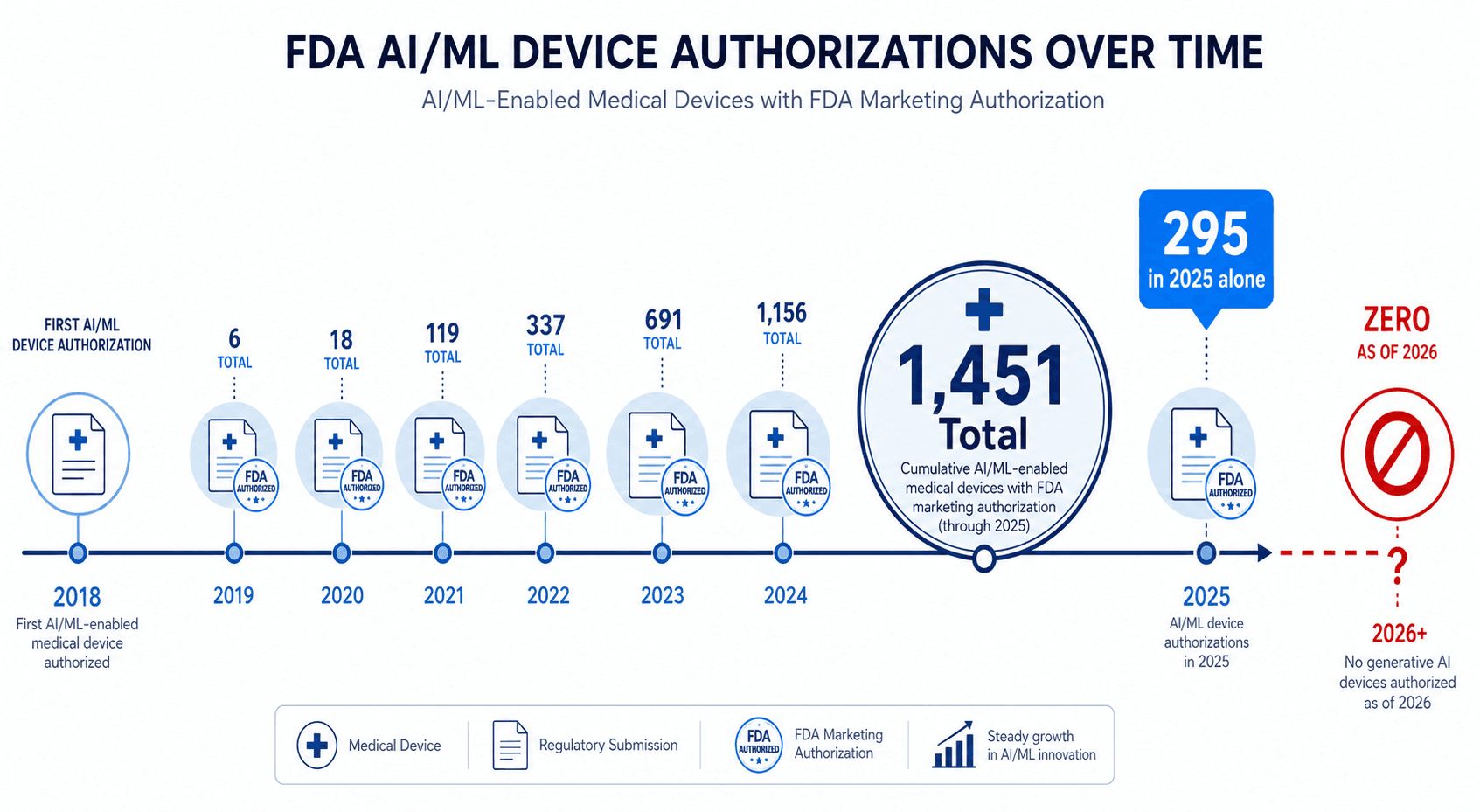
As of March 2026, the FDA has authorized 1,451 AI/ML-enabled medical devices — up from 1,250 in 2025. Of these, 1,396 used the 510(k) clearance pathway. In 2025 alone, the agency cleared 295 AI/ML-enabled devices from 221 unique manufacturers, with a median clearance time of 142 days. Radiology dominates the landscape with 1,104 devices (71.5% of all clearances), followed by cardiovascular (141), neurology (67), anesthesiology (27), and gastroenterology-urology (26).
Yet within this rapidly growing catalog, a notable absence stands out: no device using generative AI or powered by large language models has been authorized by the FDA as of March 2026. This is not a trivial gap. It means that every conversational AI tool currently marketed to health systems — whether for patient triage, clinical documentation, or decision support — operates outside the FDA's medical device regulatory framework, or relies on a predicate that does not account for the unique failure modes of generative models.
| Metric | Value |
|---|---|
| Total FDA-authorized AI/ML devices (March 2026) | 1,451 |
| Devices cleared in 2025 alone | 295 |
| Devices using 510(k) pathway | 1,396 (96.2%) |
| Radiology devices (dominant specialty) | 1,104 (71.5%) |
| Generative AI devices authorized | 0 |
| Median 510(k) clearance time (2025) | 142 days |
| Devices with PCCPs (2025) | 10% |
The absence of FDA authorization for generative AI devices has direct consequences for procurement. Health systems that rely on FDA clearance as a baseline safety signal cannot assume that a conversational AI tool has undergone the same level of regulatory scrutiny as a traditional AI-based diagnostic device. The FDA's existing framework for software as a medical device (SaMD) was designed for deterministic algorithms, not for the probabilistic, non-reproducible outputs characteristic of large language models.
What the RCT Evidence Actually Shows
A 2024 scoping review published in The Lancet Digital Health examined 86 randomized controlled trials evaluating AI in clinical practice, published between 2018 and 2023. The review provides the most comprehensive picture to date of where AI — including conversational systems — has been rigorously tested. The headline finding: 81% of trials reported positive primary endpoints, primarily diagnostic yield or performance metrics. But the details beneath that number reveal significant limitations.
| Characteristic | Finding |
|---|---|
| Total RCTs reviewed | 86 |
| Trials reporting positive primary endpoints | 81% |
| Single-center trials | 63% |
| Median sample size | 359 patients |
| Trials in gastroenterology | 43% |
| Trials in radiology | 13% |
| Trials evaluating deep learning for imaging | 69% |
| AI models developed in industry | 55% |
| Trials citing CONSORT-AI guidelines | 19% |
| Trials reporting significant decrease in operational time | 35% |
| Trials reporting significant increase in operational time | 25% |
Several patterns warrant caution. First, 63% of trials were single-center, which limits generalizability. A model that performs well at one institution with a specific patient population, hardware configuration, and clinical workflow may fail when transplanted to a different setting. Second, the distribution of trials is heavily skewed: 43% were in gastroenterology, and 69% evaluated deep learning systems for medical imaging. Conversational AI and NLP-based clinical decision support tools are barely represented in the RCT literature.
Third, 55% of AI models evaluated in these RCTs were developed in industry, raising questions about publication bias and the independence of evaluations. Only 19% of trials cited the CONSORT-AI reporting guidelines, which were specifically designed to improve the completeness and transparency of AI trial reporting. The review also notes that 25% of trials reported a significant increase in operational time — a reminder that AI tools do not universally save time, and that workflow integration is a non-trivial challenge.
For conversational AI tools specifically — chatbots, voice-based triage systems, LLM-powered clinical documentation assistants — the RCT evidence base is even thinner. A separate systematic review of AI and NLP techniques for clinical decision support systems, covering 26 studies published between 2000 and 2023, found that 81% used NLP for data collection and 69% used EHRs as a data source, but only 19% used combined NLP strategies. One notable exception: a real-time NLP-driven clinical decision support tool for opioid misuse screening in hospitalized adults achieved 93% sensitivity and 92% specificity in a 30-month quasi-experimental study involving 12,500 patients. But such examples are outliers, not the norm.
Key Barriers to Adoption: Immaturity, Cost, and Regulatory Uncertainty
The Scottsdale Institute survey of 43 U.S. health systems provides a data-driven ranking of the obstacles that prevent AI tools from moving from pilot to production. When asked to identify the primary barriers to AI adoption, health system leaders pointed to three dominant factors:
- Immature AI tools (77%) — The top barrier by a wide margin. Leaders reported that many AI products are not yet reliable enough for clinical use, produce inconsistent outputs, or require excessive human oversight to be practical.
- Financial concerns (47%) — The cost of acquiring, integrating, and maintaining AI tools, combined with uncertain return on investment, remains a significant deterrent. This is especially acute for smaller health systems without dedicated innovation budgets.
- Regulatory uncertainty (40%) — The absence of clear FDA guidance for generative AI tools, combined with evolving state and federal AI governance frameworks, creates hesitation among risk-averse health system leadership.
These barriers are compounded by a fourth, less frequently discussed factor: health equity measurement remains a blind spot. The same survey found that only 17% of organizations always measure the impact of AI on health equity and disparities. 10% rarely measure it, and 20% do not measure it at all. For conversational AI tools, which may perform differently across dialects, languages, and health literacy levels, this measurement gap is a material risk.
The practical implication is that health systems evaluating conversational AI tools should not assume that a vendor's claims of "FDA-cleared" or "HIPAA-compliant" are sufficient due diligence. The regulatory status of generative AI tools is ambiguous, the evidence base is thin, and the financial risk of a failed deployment is substantial. A structured evaluation framework is not optional — it is a prerequisite for responsible adoption.
WHO Ethical Principles and Their Application to Conversational AI
The World Health Organization has articulated six ethical principles for the use of AI in healthcare, published in guidance that applies across all AI modalities — including conversational systems. These principles provide a framework that health systems can use to evaluate not just whether a tool works, but whether it should be deployed at all.

- Protection of autonomy: Conversational AI systems must not deceive patients into believing they are interacting with a human clinician. Clear disclosure of AI identity, the limits of the system's capabilities, and the option to escalate to a human provider are non-negotiable.
- Promoting human welfare, safety, and the public interest: The system must be safe for its intended use. For conversational AI, this means rigorous testing for harmful outputs, clinical misinformation, and failure modes that could delay or prevent appropriate care.
- Ensuring transparency, explainability, and intelligibility: When a conversational AI tool makes a recommendation or generates a clinical note, the basis for that output must be traceable. Black-box systems that cannot explain their reasoning are incompatible with the principle of informed clinical decision-making.
- Fostering accountability and responsibility: The diffusion of responsibility among developers, health systems, and individual clinicians is a known challenge. Clear protocols for who is accountable when a conversational AI system produces an error must be established before deployment, not after.
- Ensuring inclusivity and equity: Conversational AI tools must be tested across diverse patient populations, including speakers of non-standard dialects, patients with limited health literacy, and those with disabilities that affect communication. A system that works well for one demographic group may fail — or cause harm — for another.
- Promoting responsive and sustainable AI: Systems must be designed for ongoing monitoring, updating, and eventual decommissioning. Model drift — where a conversational AI's performance degrades over time as language patterns or clinical knowledge evolve — is a known risk that requires active management.
These principles are not abstract. They translate directly into procurement criteria, deployment protocols, and ongoing governance requirements. A health system that cannot demonstrate how it will address each of these principles for a given conversational AI tool should reconsider whether that tool is ready for clinical use.
Practical Evaluation Frameworks for Health Systems
Given the evidence gap and regulatory uncertainty, health systems need a structured approach to evaluating conversational AI tools. The following framework organizes evaluation criteria into four domains, each with specific questions that procurement and clinical governance teams should answer before committing to a deployment.
| Domain | Key Questions | Red Flags |
|---|---|---|
| Evidence quality | What peer-reviewed evidence supports this tool? Is there an RCT, prospective study, or only a vendor white paper? What is the study population and sample size? Has the tool been externally validated? | No published evidence; evidence only from vendor-funded studies; single-center validation only; no demographic diversity data |
| Regulatory status | Does the tool have FDA clearance? If so, what pathway (510(k), De Novo)? If not, what is the manufacturer's regulatory strategy? Is the tool classified as a medical device or a non-device health IT tool? | Claims of FDA clearance without a submission number; unclear regulatory classification; no plan for future FDA submission |
| Integration and workflow | Does the tool integrate with the existing EHR via FHIR APIs or other standards? What is the impact on clinician workflow? Does it require dedicated IT support? What is the documented failure rate in real-world deployments? | No EHR integration; requires manual data entry; increases documentation time; no published deployment data |
| Equity and safety monitoring | How was the tool tested across different patient populations? What is the plan for ongoing monitoring of performance disparities? How are harmful outputs detected and addressed? | No demographic performance data; no plan for equity monitoring; no process for reporting adverse events or model failures |
Health systems should also consider the maturity of the vendor organization itself. The conversational AI market includes startups with limited track records alongside established health IT companies. Questions about funding stage, number of active deployments, and the vendor's approach to model updates and version control are all relevant to assessing long-term viability.
Future Direction: CHAI Assurance Standards and Emerging Governance Networks
Several initiatives are underway to close the gap between conversational AI's market momentum and its clinical maturity. These efforts aim to provide the assurance infrastructure that health systems need to evaluate and deploy AI tools responsibly.
- CHAI assurance standards: The Coalition for Health AI (CHAI) is developing assurance standards specifically designed to help health systems evaluate AI tools across dimensions of safety, effectiveness, and equity. These standards are intended to complement FDA regulation by providing a framework for local governance and procurement decisions.
- VALID AI: This initiative focuses on creating a voluntary certification program for AI in healthcare, modeled on the UL safety certification process. The goal is to provide a recognizable trust signal that health systems can use when evaluating AI tools, including conversational AI systems.
- Health AI Partnership (HAIP) networks: A consortium of health systems collaborating on AI governance best practices, HAIP produces shared resources for AI evaluation, deployment, and monitoring. Health systems that join such networks gain access to peer-reviewed evaluation templates, shared incident reporting, and collective bargaining leverage with vendors.
These emerging frameworks are not yet mature enough to replace FDA clearance or RCT evidence. But they represent a recognition that the existing regulatory and evidence infrastructure is insufficient for the unique challenges posed by conversational AI. Health systems that engage with these networks now will be better positioned to evaluate and deploy conversational AI tools as the evidence base and regulatory framework evolve.
The central message for healthcare professionals, policy readers, and procurement decision-makers is this: the conversational AI market is real, the investment is coming, and the potential benefits are substantial. But the evidence base is not yet commensurate with the market hype. Responsible deployment requires a clear-eyed assessment of what is known, what is not known, and what frameworks exist to bridge that gap. The tools that will succeed in the long term are not the ones with the largest marketing budgets — they are the ones that can demonstrate safety, efficacy, and equity through rigorous, independent evidence.
Comments
Join the discussion with an anonymous comment.