The surveillance problem is easy to miss because the chart can look complete. A patient arrives in an emergency department, the clinician documents poultry, livestock, or other animal exposure somewhere in the note, and the visit moves forward as an ordinary respiratory or conjunctivitis encounter. If H5N1 testing is not ordered, the patient never enters the part of the surveillance system that is easiest to count.
CDC monitoring for H5N1 in people is built around lab-confirmed infections and testing among exposed people, which is the right foundation for national reporting. What it cannot show, by itself, is how often relevant exposure histories were documented in emergency department records but never translated into a test order or public health signal.[1] That is the gap where AI-assisted avian influenza outbreak detection becomes less of a broad technology claim and more of a chart-review problem at scale.

What the Maryland study actually found
A University of Maryland School of Medicine team tested whether GPT-4 Turbo could retrospectively screen emergency department documentation for H5N1-relevant animal exposure. The study analyzed 13,494 adult emergency department visits across the University of Maryland Medical System in 2024.[2] The model flagged 76 records for possible relevant exposure; human review confirmed 14 patients with recent animal exposures that mattered for H5N1 risk assessment.[2]
The most important sentence in that result is also the easiest one to flatten: none of those 14 patients had been tested for H5N1.[2] The model did not uncover bird flu cases. It uncovered documented exposure risk that had not become H5N1 testing. Infection status remained unknown because the clinical workflow had already passed the point where a test might have answered the question.
That distinction matters operationally. A hospital epidemiologist does not need an LLM to announce that a patient has H5N1 without laboratory evidence. What may be useful is a system that notices when the chart already contains a reason to consider testing, isolation guidance, occupational exposure follow-up, or a public health call — especially when that reason is embedded in ordinary narrative text rather than a discrete field.
| Study element | What it means for surveillance |
|---|---|
| 13,494 adult ED visits in 2024 | The model was applied across a real health-system emergency department corpus, not a handpicked set of known positives. |
| 76 flagged records | The screen narrowed a large review task to a small set of charts for human validation. |
| 14 confirmed recent H5N1-relevant exposures | The confirmed signal was small but clinically meaningful because these patients had not been tested. |
| No H5N1 tests among the 14 | The study identifies missed testing opportunities, not confirmed infections. |
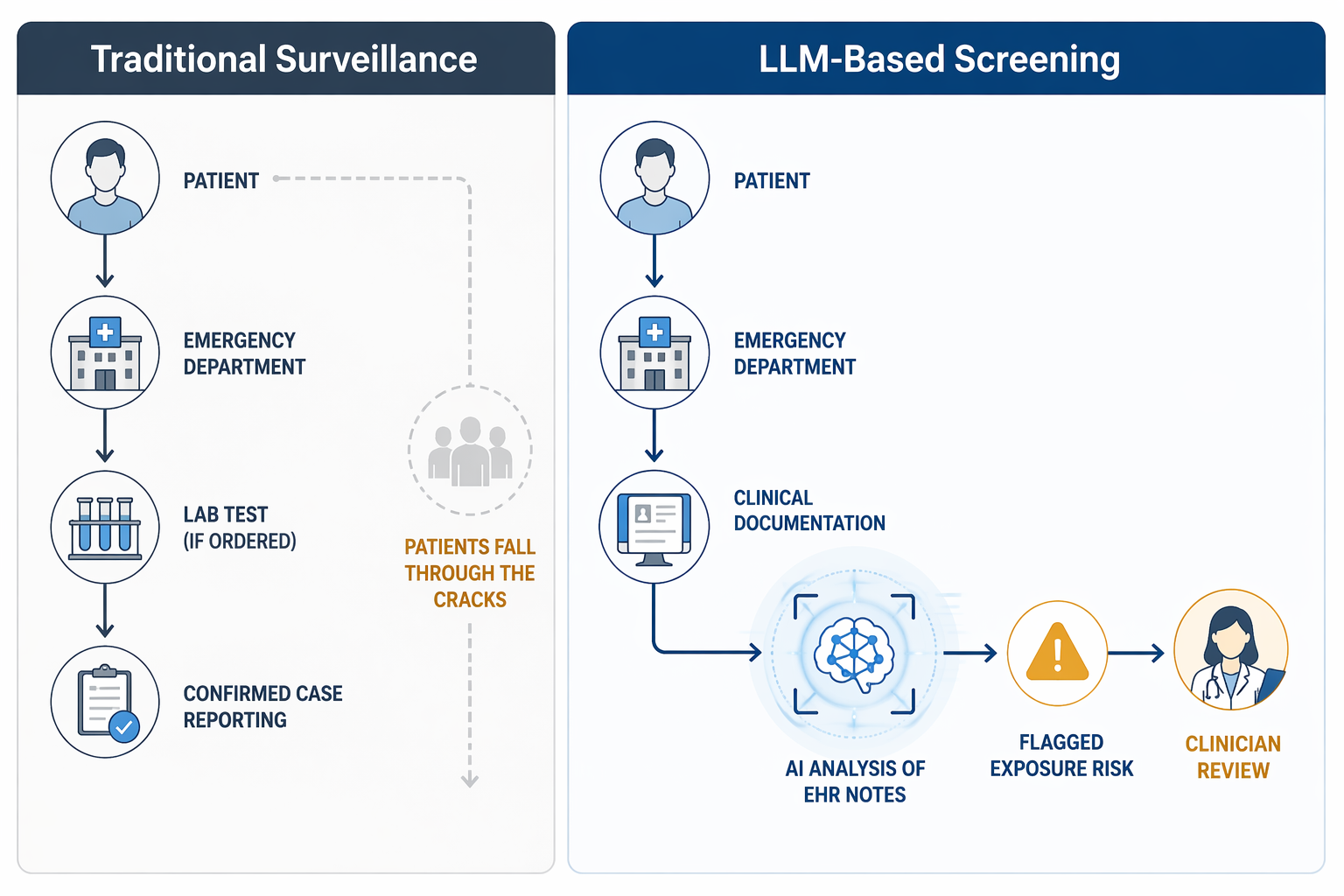
The surveillance shift is from confirmed cases to documented risk
Traditional case surveillance becomes visible when testing happens. The Maryland workflow starts earlier, at the point where exposure history is written down but has not necessarily been acted on. In practical terms, GPT-4 Turbo was not replacing a laboratory test or a clinician’s judgment. It was reading notes for phrases and contexts that suggest animal exposure relevant to H5N1, then pushing a subset of records toward human review.
That is a narrower and more useful claim than saying generative AI detects outbreaks. In an emergency department, exposure details often appear in the same free-text space as work history, home environment, animal contact, travel, or presenting symptoms. Those details may be clinically relevant but inconsistently structured. A language model’s advantage is not that it is glamorous; it is that it can read messy narrative fast enough to make a second-pass surveillance workflow plausible.
The workflow also changes who gets burdened after the miss. Without an upstream flag, infection prevention staff or public health investigators may later try to reconstruct whether anyone asked about animal exposure, whether the answer was documented, and whether the absence of testing reflected low suspicion or simple failure to notice the clue. A retrospective LLM screen cannot undo that, but it can show that the raw material for earlier action was already present in the record.
The performance numbers are promising, but they answer a limited question
On a historical validation sample of 10,000 emergency department visits from 2022 to 2023, the tool achieved a 90% positive predictive value and a 98% negative predictive value.[2] Those metrics are strong enough to make the workflow worth serious attention, particularly because the intended task is triage for review rather than autonomous diagnosis.
Positive predictive value answers a practical staffing question: when the model flags a chart, how often is the reviewer likely to find a real relevant exposure? Negative predictive value answers a different question: when the model does not flag a chart, how often is it likely to be correct that the chart lacks the target exposure signal? In this use case, both matter. A low PPV would bury reviewers in noise. A low NPV would leave the surveillance gap mostly intact.
The study also reported 26 minutes of human input and an estimated $0.03 per patient note for the GPT-4 Turbo analysis.[2] Those numbers are the reason this is more than a model-performance anecdote. If a chart-level exposure screen requires hours of expert review per day, it becomes another unfunded infection prevention wish. If it can narrow the review set cheaply, it begins to resemble a surveillance assist that a health system might pilot.
Still, the metrics do not prove that real-time alerts will improve care. They came from retrospective analysis, where the chart is already written, no clinician is being interrupted, and no one has to decide whether to order a test during a crowded shift. A live emergency department adds harder variables: alert fatigue, clinician trust, timing of documentation, EHR integration, local testing access, and who is accountable for responding when the system fires.
Exposure recognition is not infection detection
The cleanest way to describe the Maryland result is this: GPT-4 Turbo identified patients whose records contained documented animal exposure that could have supported H5N1 testing consideration. It did not determine whether those patients were infected, contagious, or part of an outbreak cluster. Because none of the 14 confirmed exposure-risk patients were tested, the study cannot tell us whether testing would have found H5N1.[2]
CIDRAP’s coverage of the study highlighted the same practical boundary, including the Clinical Infectious Diseases commentary by Shenoy and colleagues that framed the tools as finding “chickens, not eggs.”[3] The phrase is useful because it keeps the inference in the right place. The model can identify known risk factors when those risk factors are documented. It cannot infer an exposure the patient never mentioned, a clinician never asked about, or a note never captured.
That boundary is not a minor limitation. If a farmworker avoids disclosing animal contact, if an exposure history is taken verbally but not entered into the note, or if a patient does not recognize that backyard poultry contact matters, an EHR-based LLM has nothing reliable to read. The harder public health problem remains upstream: making sure the exposure history is asked, understood, documented, and acted on.
Where this fits in the larger AI surveillance ecosystem
The Maryland study sits at the clinical end of AI surveillance: individual patient records, documented risk factors, and potential clinician follow-up. Other systems work farther away from the bedside. EPIWATCH, for example, uses natural language processing on open-source information to generate early epidemic signals before official detection, while AI-enabled wastewater methods look for population-level viral patterns outside clinical encounters.
Those approaches are complementary rather than interchangeable. A 2025 Nature Communications study from UNLV researchers used an AI-driven algorithm on roughly 3,700 wastewater samples and identified viral variant signatures with as few as 2 to 5 samples earlier than existing methods; the study focused on SARS-CoV-2, while the authors discussed broader applicability to influenza.[4] Wastewater can see signals that never become a hospital visit. ED chart screening can see documented clinical context that wastewater cannot assign to a patient.
For a broader view of what these systems can and cannot deliver across public health settings, ClinicalMind’s article on what AI surveillance actually delivers for public health is the better place to widen the lens. The Maryland H5N1 study is valuable precisely because it does not try to be the whole surveillance ecosystem. It tests whether one known blind spot in emergency care can be made more visible.
What a hospital still has to prove before deployment
A credible retrospective screen is not the same thing as a safe live intervention. Before this becomes a production EHR alert, a hospital would need to decide where the signal goes: the treating clinician, infection prevention, an ED charge nurse, an occupational health pathway, or a public health liaison. Each recipient changes the workflow and the failure mode.
- If the alert goes to the treating clinician, it must arrive early enough to affect testing and isolation decisions.
- If it goes to infection prevention, the team needs authority and staffing to review charts quickly.
- If it creates a public health notification, the criteria must avoid turning weak documentation into overconfident reporting.
- If it runs silently for surveillance review, the hospital must define how missed opportunities are fed back into clinical practice.
Generalizability is also unsettled. The study came from one health system, and performance may change in regions with different animal exposure patterns, different documentation habits, different EHR note templates, or different levels of clinician awareness. A model that reads one institution’s notes well may still need local validation before it is trusted elsewhere.
Cost deserves the same caution. The $0.03-per-note estimate is encouraging, but it reflects GPT-4 Turbo API pricing at the time of the study.[2] A hospital implementation has to account for current model pricing, privacy and security architecture, HIPAA-compliant deployment, monitoring, governance, and the human labor attached to every true or false alert.
LLM-based EHR screening now has credible retrospective evidence as an affordable way to surface documented H5N1 exposure risk that current surveillance can miss. The next unanswered question is not whether GPT-4 Turbo can read old notes. It is whether prospective alerts can lead clinicians to test appropriate patients without adding workflow noise, misplaced confidence, or another queue that someone downstream has to clean up.
References
- H5N1 Bird Flu: Current Situation, CDC.
- Generative AI Uncovers Undetected Bird Flu Exposure Risks in Maryland Emergency Departments, University of Maryland School of Medicine, 2025.
- AI tool can help identify patients who may have H5N1 avian flu: Researchers, CIDRAP.
- AI and wastewater surveillance unite to detect emerging viruses, News-Medical, 2025.
Comments
Join the discussion with an anonymous comment.