The practical question around Google medical AI in 2026 is no longer whether Google is serious about health. It plainly is. The harder question is whether each system is a research model, a developer asset, a consumer-health feature, a drug-discovery platform, or something ready to be deployed as a regulated clinical medical device. As of mid-2026, the answer is uneven: Google has several substantial medical AI fronts, but no Google generative AI model has FDA authorization as a medical device, based on public FDA AI-device tracking and outside analyses of the cleared-device landscape.[1][2]
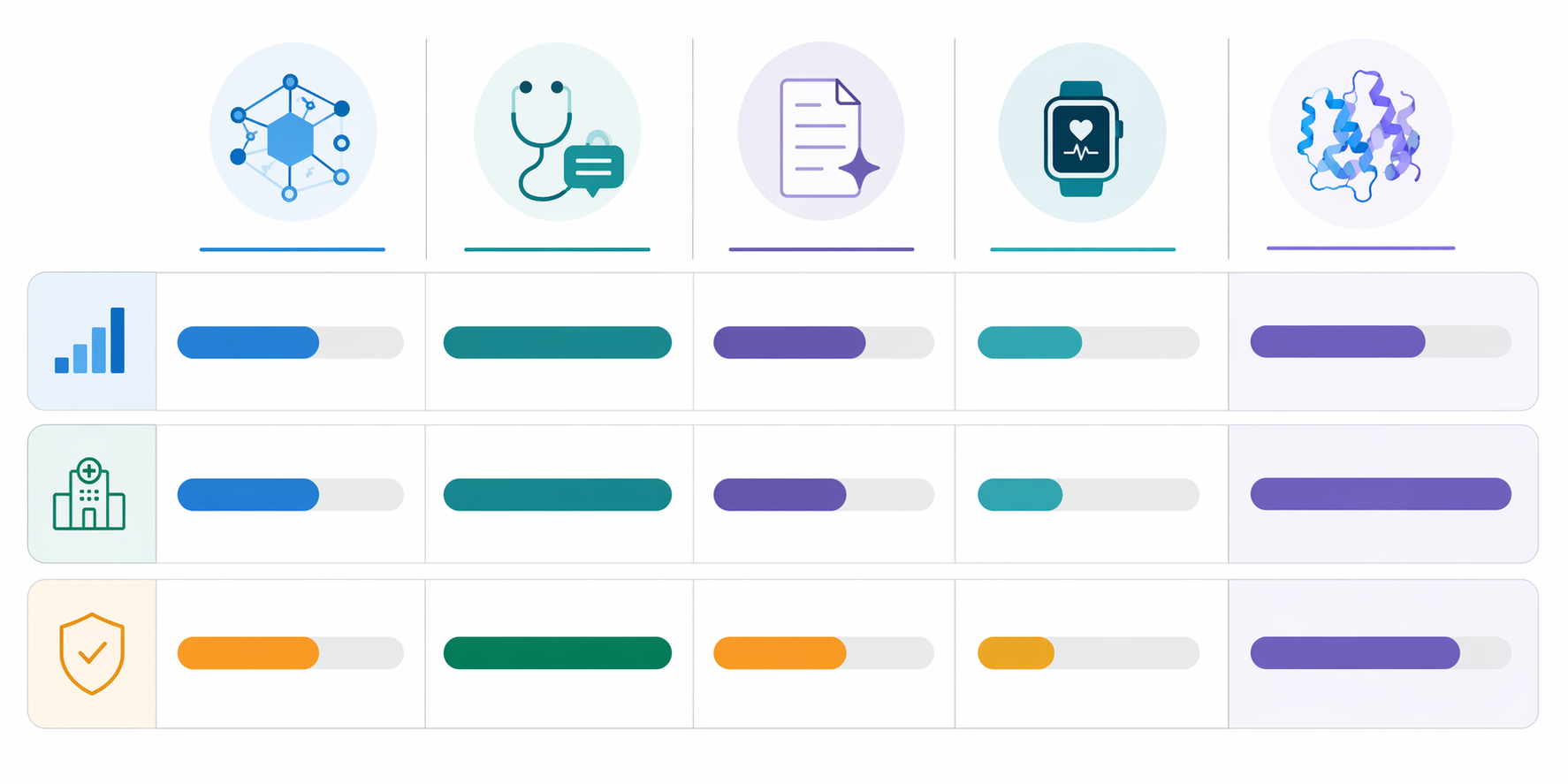
| Initiative | Primary purpose | Evidence maturity as of mid-2026 | Deployment stage | Regulatory status |
|---|---|---|---|---|
| AMIE | Conversational diagnostic and disease-management AI | Strongest clinical evidence path in the portfolio: prospective real-patient feasibility work, longitudinal simulated disease-management research, and multimodal simulated telemedicine studies | Research and feasibility evaluation; not established as routine clinical deployment | No FDA device authorization identified for AMIE |
| MedGemma | Open medical AI models for developers and researchers | Benchmark-oriented and explicitly pre-clinical-grade; includes 4B and 27B variants positioned as efficient medical AI foundations | Open model access for validation, adaptation, and research use | Not presented as a cleared clinical device |
| Med-PaLM 2 / MedLM | Clinical knowledge and medical question-answering models | Important benchmark-era predecessor; Med-PaLM 2 reported 86.5% on USMLE-style questions | Cloud-accessible through Google Cloud / Vertex AI pathways for approved use cases | No FDA device authorization identified for clinical-device use |
| Fitbit Personal Health LLM / Large Sensor Model | Consumer health coaching and sensor-based wellness intelligence | Public evidence emphasizes product capability claims, including sleep and continuous glucose monitor integration; limited peer-reviewed clinical validation is available | Consumer health and wellness product direction | Not presented as an FDA-authorized diagnostic or treatment device |
| AlphaFold / Isomorphic Labs | Protein structure, biology, and drug-discovery infrastructure | Scientifically important discovery platform, but not a patient-facing clinical AI system | Research and drug-discovery pipeline support | Not in the same regulatory lane as conversational clinical AI |
That table is the main point. These systems should not be treated as one product line moving through a single maturity curve. A model released to developers is not the same thing as a model prospectively studied with patients. A consumer health coach is not the same thing as a diagnostic device. A protein-structure engine can be strategically important without being clinically deployable at the bedside.
MedGemma: Open Models With a Deliberately Pre-Clinical Boundary
MedGemma is Google’s most open medical AI move in this group. Google describes 4B and 27B model variants, with positioning around medical text and multimodal development, and states that MedGemma can perform on par with much larger models on MedQA-style benchmarks.[3] That matters for researchers and developers who want a medically oriented starting point rather than a closed demonstration.
The caution is also built into the product frame. Google’s Health AI Developer Foundations materials present MedGemma as pre-clinical-grade, not as a system ready for independent clinical use.[3] That distinction should not be softened. Open availability can accelerate experimentation, local validation, fine-tuning, and safety work; it does not, by itself, create evidence of patient benefit or regulatory clearance.
AMIE Is the Most Clinically Interesting Track
AMIE deserves more attention than the other generative medical AI systems because Google has moved it beyond static benchmark performance into more clinically recognizable evaluations. The evidence still stops well short of deployment readiness, but the direction is different: real patients, feasibility endpoints, multi-visit disease-management simulations, and multimodal telemedicine scenarios.

The BIDMC Feasibility Study Put AMIE in Front of Real Patients
In March 2026, Google described a prospective single-center feasibility study of AMIE at Beth Israel Deaconess Medical Center involving 100 real patients.[4] The study reported zero safety stops, 90% differential-diagnosis accuracy including the final diagnosis, and patient trust improvements measured with the General Attitudes towards Artificial Intelligence Scale.[4]
Those are meaningful details because they move the discussion from “can a model answer medical exam questions?” to “what happens when real patients interact with a conversational diagnostic system under study conditions?” A zero-safety-stop result is not a proof of safety in routine care, and 100 patients at one center cannot establish generalizable diagnostic performance. But the study does mark a more serious evidentiary posture than benchmark-only claims.
The Disease-Management Work Raised the Ambition
Google’s June 2026 AMIE disease-management work moved from one-time diagnostic conversations toward longitudinal care scenarios. The study used 100 multi-visit scenarios across seven specialties and a two-agent architecture, and Google reported that AMIE was non-inferior to 21 primary care physicians on overall management while outperforming them on treatment preciseness and guideline alignment.[5][6]
The clinical ambition is larger here, but so is the interpretive burden. Multi-visit management is closer to the shape of chronic care than a single diagnostic exchange, and specialty breadth makes the test harder to dismiss as narrow pattern matching. Still, these were constructed scenarios, not a demonstration that AMIE improves outcomes, reduces harm, or can be safely inserted into a live care pathway without tightly specified supervision.
The Multimodal Study Shows Why Benchmarks Are Not Enough
The April 2026 AI co-clinician work, conducted with Harvard and Stanford collaborators, evaluated multimodal telemedicine-style encounters with 120 simulated cases.[7] The study is useful partly because it is not uniformly flattering: expert physicians outperformed the AI on red-flag detection.[7]
That result is exactly the kind of detail that should survive the headline. Red-flag detection is not a decorative subscore in telemedicine; it is one of the ways a system avoids false reassurance. A model can look medically fluent and still underperform on the moments when escalation matters most. The study also used simulated patient actors rather than real patients, so it should be read as a research step rather than evidence of clinical readiness.
The Regulatory Gap Is Not a Footnote
The AMIE studies show evidence progress; they do not create FDA authorization. Public AI medical-device tracking does not identify a Google generative medical AI model with FDA device authorization as of mid-2026, and outside analysis of the FDA-cleared AI-device landscape reaches the same broad conclusion.[1][2] The FDA’s public AI-device list is not comprehensive, so this should be framed as a best available public-record finding rather than omniscience. It is still the right operational assumption for a health system.
The contrast with Aidoc’s CARE1 is useful only for regulation, not for capability matching. Aidoc announced CARE1 as the first FDA-cleared foundation model in February 2025, which shows that foundation-model-style systems can enter the FDA-cleared device category under some use cases.[1] It does not mean AMIE, MedGemma, or MedLM serve the same function, carry the same indications, or could be evaluated under the same evidentiary package.
For a clinician or health IT leader, this distinction changes the deployment conversation. The question is not whether the model is impressive. It is whether the specific intended use has been validated, whether the clinical workflow defines who reviews the output, whether failure modes have been measured in the target population, and whether the regulatory claim matches the proposed use. For more on the broader pattern, ClinicalMind’s review of the conversational AI evidence and regulatory gap covers the same tension across systems.
Med-PaLM 2 and MedLM: Important, But Mostly Earlier in the Evidence Chain
Med-PaLM 2 remains important because it helped define Google’s clinical-language-model credibility. Google reports that Med-PaLM 2 reached 86.5% on USMLE-style questions, and MedLM is available through Google’s cloud model pathways, including Vertex AI.[8] That makes the Med-PaLM-to-MedLM line relevant to enterprise experimentation and clinical knowledge tasks, especially where organizations can wrap models with governance, evaluation, and human review.
But benchmark performance and cloud availability should not be collapsed into bedside readiness. The model family is better read as a foundation for clinical AI development than as proof of regulated clinical deployment. ClinicalMind’s deeper profile of Google clinical AI models from Med-PaLM to Med-Gemini is the better place to unpack the benchmark lineage in detail.
Fitbit’s Health LLM Belongs in Consumer Health Unless Better Validation Appears
Google’s Fitbit direction is different from AMIE. The Personal Health LLM and Large Sensor Model are aimed at consumer health coaching and interpretation of wearable data. Google has described a 15% sleep accuracy improvement and continuous glucose monitor integration as part of its 2026 health AI updates.[9]
Those claims may matter for wellness products, user engagement, and longitudinal self-tracking. They do not yet amount to a peer-reviewed clinical validation story for diagnosis or treatment. A health coach that helps users understand sleep, activity, or glucose context may be useful; it should not be described as a regulated medical AI system unless the evidence and authorization support that description.
AlphaFold Is a Different Lane, Not a Weaker Clinical Chatbot
AlphaFold should not be forced into the same maturity scale as AMIE or MedLM. Its relevance is primarily biological research and drug discovery, including work connected to Isomorphic Labs, rather than direct patient conversation or clinical decision support. The practical evaluation question is therefore different: how does it change target discovery, structural biology, and therapeutic development workflows, not whether it can be deployed in a clinic as a diagnostic assistant.
That distinction cuts both ways. AlphaFold’s importance should not be discounted because it lacks a bedside deployment story. At the same time, its scientific reach does not fill the regulatory gap for Google’s generative clinical systems. Discovery infrastructure and clinical medical devices answer to different evidentiary expectations.
What Is Clinically Evidenced, and What Is Deployable?
The clinically strongest Google medical AI thread is AMIE. It has prospective real-patient feasibility evidence at BIDMC, simulated longitudinal disease-management research, and multimodal telemedicine simulation work that includes both strengths and a clinically important weakness in red-flag detection.[4][5][7] That is a real evidence trajectory, not just a demo sequence.
The deployment answer is narrower. AMIE is not established as a routinely deployable FDA-authorized medical device. MedGemma is explicitly pre-clinical-grade and developer-facing. Med-PaLM 2 and MedLM remain best understood as clinical knowledge model infrastructure rather than cleared bedside tools. Fitbit’s LLM work is consumer-health oriented with limited public clinical validation. AlphaFold belongs mainly to discovery and biology.
So the mid-2026 judgment is not that Google medical AI is overhyped or empty. It is that the portfolio is broad, technically serious, and increasingly studied, while its components sit on different evidence tracks. None of the generative medical AI initiatives should be presented as FDA-authorized clinical medical devices as of mid-2026.
References
- FDA AI Medical Device Tracker, IntuitionLabs.
- The Current State of Over 1450 FDA Approved AI-Based Medical Technologies, Bertalan Meskó, MD, PhD, LinkedIn.
- MedGemma, Google Health AI Developer Foundations.
- Exploring the feasibility of conversational diagnostic AI in a real-world clinical study, Google Research, March 2026.
- From diagnosis to treatment: Advancing AMIE for longitudinal disease management, Google Research, June 2026.
- Google advances its AMIE research medical AI from diagnosis to treatment, Google, June 2026.
- AI co-clinician: researching the path toward AI-augmented care, Google DeepMind, April 2026.
- AI models, Google Health.
- How Google is using AI to improve health for everyone, Google, 2026.
Comments
Join the discussion with an anonymous comment.