The important word in “humanoid robot in laparoscopic surgery” is not “autonomous.” In the Liang et al. study published in Nature in July 2026, the robots did not independently decide how to dissect Calot’s triangle, clip the cystic duct, or remove a gallbladder. Surgeons teleoperated Unitree G1 humanoid platforms through the LapSurgie framework while performing laparoscopic cholecystectomy in live porcine models.[1]
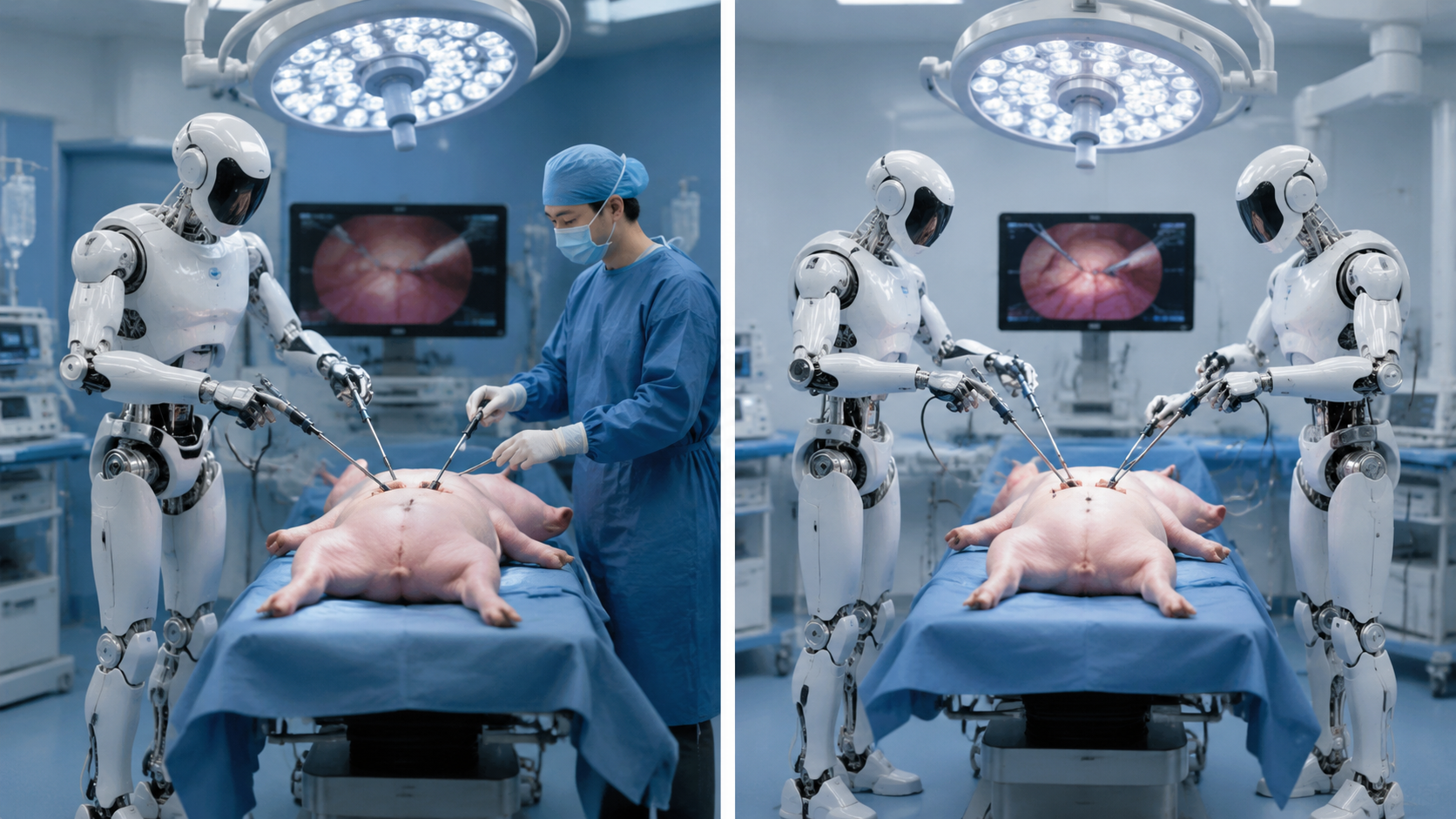
That correction matters because it makes the result more, not less, useful. This was not a showroom arm waving a grasper over a plastic trainer. It was in vivo laparoscopic surgery, with the awkwardness of tissue, camera view, instrument exchange, traction, and operating-room choreography still present. The study tested two configurations: a human-robot team, with one humanoid robot working alongside a human assistant, and a robot-robot team, with two humanoids operating side by side. Both completed the porcine cholecystectomy task.[1]
The public attention around the paper is understandable. UC San Diego described the work as a world-first use of teleoperated humanoid robots in live surgery, and Forbes framed it in similarly eye-catching terms.[2][3] But the practical question is narrower: what did the system actually do, how did it compare with known robotic and manual baselines, and what friction appeared once the platform was asked to operate on a living model rather than demonstrate dexterity in isolation?
What Was Actually Tested
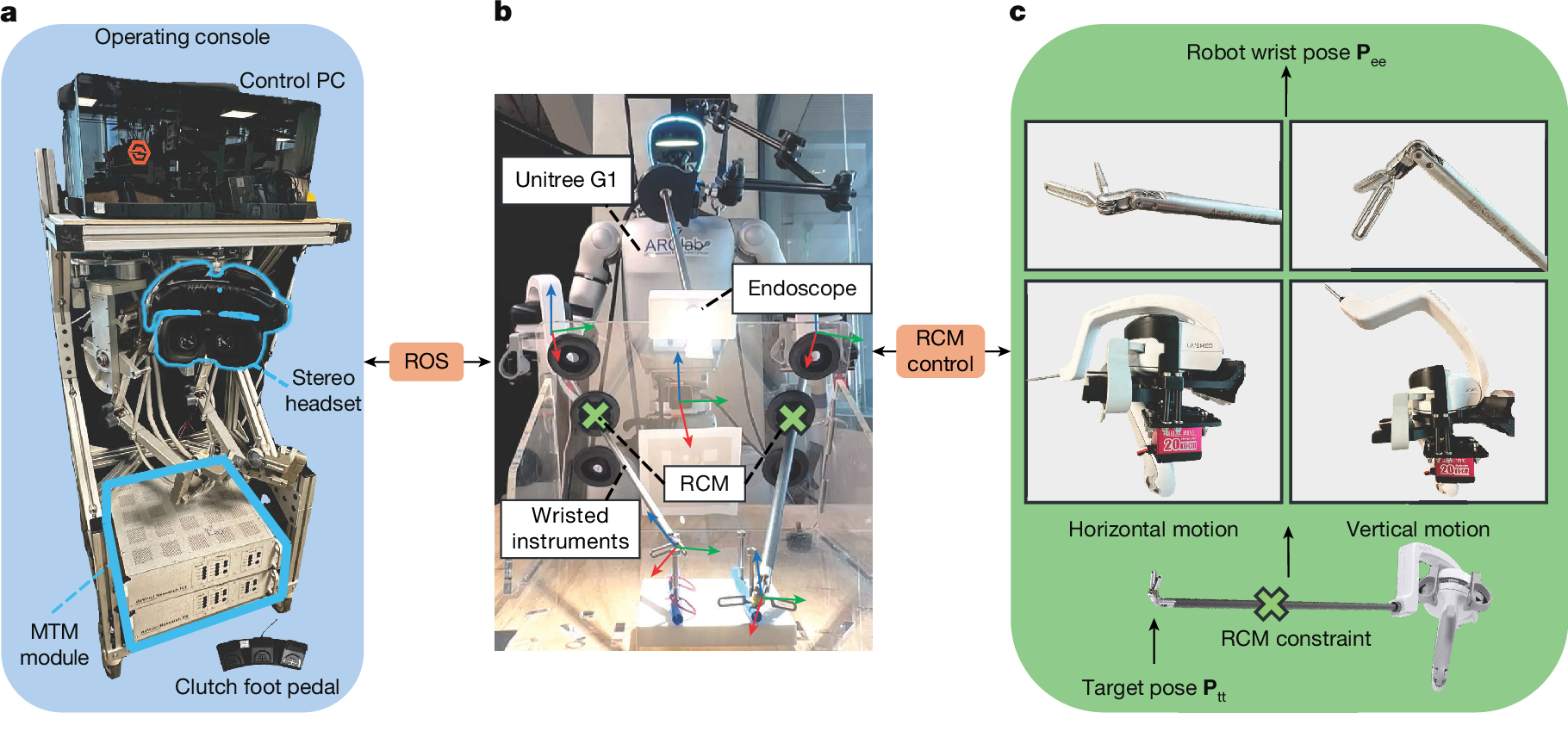
The platform was not a purpose-built hospital robot. Liang et al. used Unitree G1 humanoid robots, described in the research materials as roughly 5 ft tall, about 60 lb, bipedal, and built with 29 degrees of freedom. The commercial platform is often discussed in the low tens of thousands of dollars, with a cited range of about $16,000 to $20,000 for the stock humanoid hardware.[1]
The surgical adaptation is where the study becomes more interesting than the price tag. The robots used off-the-shelf ArtiSential/LivsMed wristed laparoscopic instruments connected through custom 3D-printed adapters, with surgeons operating through a stereo vision console and the LapSurgie teleoperation framework.[1] In other words, the experiment asked whether a general-purpose humanoid body could be made to perform a recognizable minimally invasive surgical task when paired with surgical instruments and a surgeon-controlled interface.
| Element | What the study used | Why it matters clinically |
|---|---|---|
| Robot body | Unitree G1 humanoid platform | Shows whether a general-purpose humanoid form can be adapted to an operating table rather than designing every component around one procedure |
| Control model | Teleoperation through LapSurgie | Keeps the surgeon in command; this was not autonomous laparoscopic surgery |
| Instruments | Wristed laparoscopic instruments with custom adapters | Gives the robot surgical end effectors rather than relying on generic humanoid hands |
| Procedure | Laparoscopic cholecystectomy in live porcine models | Moves the evidence beyond a dry lab task while still remaining preclinical |
| Comparators | da Vinci Research Kit and manual laparoscopy | Provides a recognizable benchmark rather than leaving performance as a standalone demonstration |
The hardware cost contrast with established surgical robots is tempting, but it should be handled with care. A stock humanoid price is not the cost of a sterile, certified, serviced, liability-covered surgical system. The da Vinci system is often discussed in the $1.8 million to $2.5 million capital range, and a 2026 ACS Bulletin article estimated a direct da Vinci cost per case around $3,300 using Intuitive’s 2024 revenue of $5.6 billion across 1.7 million procedures.[5] There is no equivalent cost-per-case denominator for humanoid-based laparoscopy.
The Accuracy Result Deserves Attention, With Restraint
The most striking quantitative result was not that the humanoid robots completed the porcine procedures. It was that, in the user study, the surgeons had their lowest mean weighted error on the humanoid platform: 2.44 ± 2.03, compared with 3.56 ± 3.80 on the da Vinci Research Kit and 4.25 ± 2.47 in manual laparoscopy.[1]
That is a real signal, and it is surprising enough to be taken seriously. The dVRK is not a consumer gadget; it is a familiar research platform derived from the da Vinci ecosystem. A humanoid system assembled from a lower-cost general-purpose platform, wristed instruments, adapters, and teleoperation software performing at least comparably on weighted error is a meaningful benchmark.
The restraint comes from the participant structure. The user study included 14 participants, but only 2 were surgeons; the other 12 were novices.[1] A result that looks favorable in a small mixed-experience cohort may not predict performance across attending surgeons, fellows, residents, or OR teams under time pressure. The available material also does not make the statistical strength of the surgeon-subset advantage clear enough to treat the lower weighted error as a settled superiority claim.
So the right reading is neither “humanoids beat da Vinci” nor “the result is too small to matter.” The study establishes that this teleoperated humanoid configuration can produce accuracy metrics in the same conversation as an established research robotic platform, and that the surgeon subset produced a lower mean weighted error on the humanoid system in this experiment.[1] That is a foundation for replication, not a purchasing argument.
Completion Is Not the Same as Surgical Readiness
The more clinically revealing evidence sits in the operational constraints. The procedures required multiple intraoperative recalibrations, and the humanoid approach took substantially longer than the dVRK comparator.[1] These are not cosmetic limitations. In laparoscopic cholecystectomy, time and interruption change the work of everyone in the room: the surgeon waits for instrument behavior to recover, the assistant maintains exposure, anesthesia continues managing a living patient, and the scrub and circulating teams absorb the uncertainty.
Recalibration is especially important because it exposes where the current system still depends on controlled tolerance rather than clinical robustness. A teleoperated instrument can look precise during a short task and still become fragile when trocar geometry, camera angle, arm position, tissue traction, and human coordination drift during a full procedure. If the team must repeatedly pause to restore alignment, the platform is still asking for protection from the workflow instead of disappearing into it.
The authors explicitly compared the long procedure times with the early da Vinci experience, noting that early da Vinci procedures initially took about 6 hours.[1] That historical comparison is fair as context: new surgical systems often begin slowly. It is not evidence that humanoid laparoscopy will follow the same improvement curve. The da Vinci trajectory depended on dedicated engineering, regulatory pathways, training systems, service infrastructure, procedural selection, and years of accumulated clinical practice. A humanoid platform would need its own evidence, not borrowed inevitability.
The Two-Team Design Shows Flexibility, Not Yet Workflow Fit
Testing both a human-robot team and a robot-robot team was a useful design choice. It prevented the study from proving only that a humanoid could act as a single teleoperated instrument holder while a human assistant quietly carried the hard parts. Showing completion in both configurations gives the platform a broader feasibility claim.[1]
Still, the configurations answer different questions. A one-humanoid setup asks whether the robot can integrate into an existing OR hierarchy where a human assistant remains available for traction, suction, troubleshooting, and judgment. A two-humanoid setup asks whether a more robotic field can be coordinated without losing safety margins. The second is more provocative, but the first may be the more relevant near-term test because clinical teams rarely adopt technology by replacing every supporting role at once.
Neither configuration resolves the central deployment issue. The study demonstrates completion under research conditions; it does not demonstrate turnover time, staff training burden, emergency conversion behavior, sterilization workflow, maintenance cadence, or liability assignment. Those questions are not less important because they are less photogenic.
What “Surgical Humanoid” Means Here
The phrase “surgical humanoid” is already being stretched across unlike machines. In this Nature study, the relevant feature is a mobile, general-purpose humanoid body adapted to laparoscopic teleoperation. That is different from fixed multi-arm surgical systems that may be branded as humanoid because they imitate aspects of human surgical posture or multi-limb coordination.
For example, LEM Surgical’s Dynamis has been described in industry coverage as the “world’s first surgical humanoid,” but it is a fixed multi-arm spinal robotic system rather than a Unitree-style mobile humanoid standing at a laparoscopic operating table.[4] The distinction is not semantic. A fixed surgical robot and a bipedal general-purpose humanoid face different safety, sterility, stability, collision, service, and OR integration problems.
Why the Porcine Model Matters, and Where It Stops
A live porcine model is a meaningful step above a box trainer or a synthetic organ model. Tissue compliance, bleeding risk, anatomic variation, laparoscopic field constraints, and team communication all become more realistic. For a first in vivo feasibility study, laparoscopic cholecystectomy is also a sensible procedure: common enough to be recognizable, structured enough to compare, and unforgiving enough that instrument control, traction, and visual orientation matter.
But porcine completion is not human clinical evidence. The study does not establish safety or effectiveness in patients, does not define patient-selection criteria, and does not show how the system behaves across diseased gallbladders, adhesions, obesity, acute inflammation, unexpected bleeding, or conversion scenarios. As of Q3 2026, no humanoid robot has regulatory clearance to perform laparoscopic surgery on human patients.
That leaves the study in a precise place: stronger than a concept video, weaker than a clinical alternative. It gives future investigators a benchmark to beat on time, recalibration frequency, latency, reliability, and safety validation.
The Cost Question Is Premature but Not Irrelevant
The low-cost hardware angle is part of the legitimate engineering appeal. If a widely available humanoid body can be adapted to surgical work, the design space changes. Researchers could iterate faster, test more configurations, and potentially separate parts of surgical robotics from the economics of proprietary capital platforms.
But the clinical cost question begins after the robot becomes a medical device. A hospital cannot buy a stock humanoid, attach wristed instruments with printed adapters, and treat it as a surgical system. Certification, redundant safety systems, draping or sterilizable interfaces, validated cleaning, service contracts, preventive maintenance, staff training, cybersecurity, software version control, malpractice coverage, and failure-mode documentation would all enter the real cost.
The da Vinci cost-per-case estimate is useful because it reminds readers that capital price is only one part of robotic surgery economics.[5] For humanoid laparoscopy, the denominator does not yet exist. There are no human case volumes, no approved indications, no service model, and no validated per-procedure consumable profile.
What Has Been Demonstrated as of Q3 2026
Liang et al. demonstrated that teleoperated humanoid robots can complete laparoscopic cholecystectomy in live porcine models using a Unitree G1-based system, wristed laparoscopic instruments, custom adapters, stereo vision, and the LapSurgie framework.[1] They also showed that, in a 14-participant user study, the surgeon subset achieved a lower mean weighted error on the humanoid platform than on the dVRK or manual laparoscopy, although that subset included only 2 surgeons.[1]
The same study also showed why this is not ready to be treated as a near-term clinical substitute: procedures took substantially longer than with the dVRK, multiple intraoperative recalibrations were required, and the work remains preclinical.[1] Latency, reliability, emergency handling, regulatory clearance, safety certification, training, and real cost per case remain unresolved.
That is enough for a serious feasibility benchmark. It is not enough for a claim that humanoid robotic surgery has arrived.
References
- Versatile humanoid robots for laparoscopic surgery, Nature, July 2026.
- Surgeons use teleoperated humanoid robots to perform live surgery, a world first, UC San Diego Today.
- Humanoid Robots Just Performed Live Surgery For The First Time Ever, Forbes, July 10, 2026.
- LEM Surgical Showcases the World’s First Surgical Humanoid at CES 2026: Groundbreaking NVIDIA Physical AI Toolsets to Drive Dynamis Robotic Surgical System Development, The Spine Market Group.
- Cost of robotic surgery remains complex equation, ACS Bulletin, February 2026.
Comments
Join the discussion with an anonymous comment.