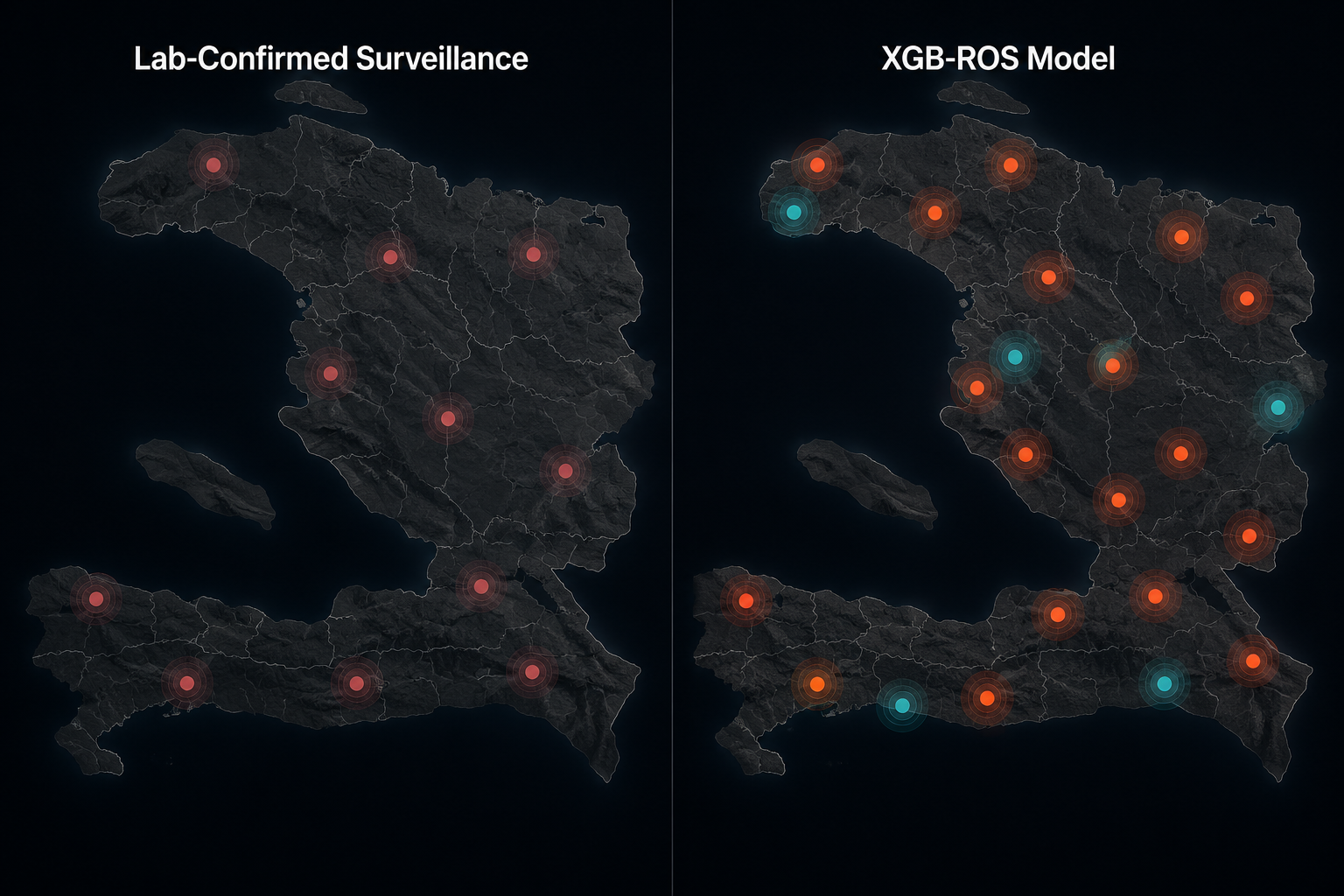
The most important result in the Haiti rabies modeling study is not that an extreme gradient boosting model performed well. It is that the map changed. Laboratory-confirmed surveillance identified 12 high-risk clusters; the XGB-ROS approach identified 20, including eight communities that had no prior diagnostic infrastructure at all.[1] In rabies surveillance, that difference is not cosmetic. It is the difference between a place with no apparent signal and a place that may have been unable to generate one.
That is where rabies symptoms and post-exposure prophylaxis guidelines matter for this discussion, but only as the clinical reason the surveillance problem is so unforgiving. Once symptomatic rabies develops, the disease is almost uniformly fatal; prevention depends on timely risk recognition and post-exposure prophylaxis after a credible exposure. If transmission zones are invisible to the public health system, bite follow-up, vaccination decisions, and field investigation begin late or never.
A surveillance signal where the laboratory system had none
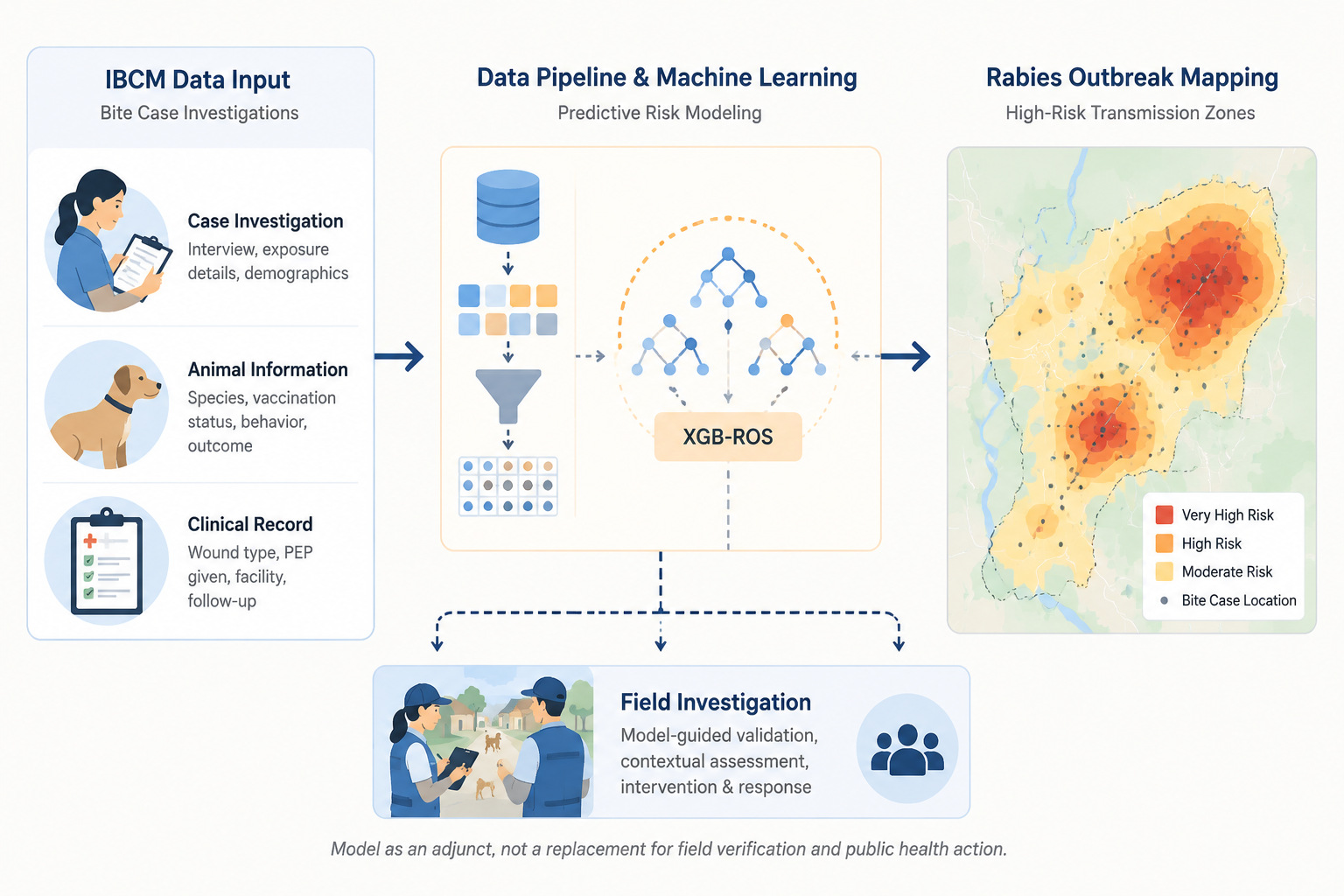
The study used 13,073 Integrated Bite Case Management investigations and trained an XGBoost model with random oversampling, then calibrated predicted probabilities using isotonic regression.[1] The model reported 0.98 accuracy and 0.99 specificity, with sensitivity of 0.78 and a negative predictive value of 1.0.[1] It classified 85.2% of confirmed rabies cases as high risk, while classifying only 0.01% of non-cases as high risk.[1]
Those metrics explain why the expanded map deserves attention, but they do not make the model a replacement for diagnosis. A sensitivity of 0.78 means some true risk can still be missed. The practical value is narrower and more useful: the model can help prioritize places for follow-up when laboratory confirmation is structurally limited, especially when routine surveillance has already shown that it cannot see some communities.
| Surveillance view | High-risk clusters identified | What it means operationally |
|---|---|---|
| Laboratory-confirmed surveillance | 12 | Finds clusters only where samples and diagnostic pathways can produce confirmed cases |
| XGB-ROS model using IBCM investigations | 20 | Adds risk signals from bite investigations, including communities without prior diagnostic infrastructure |
| Increment detected by ML approach | 40% more clusters | Expands the field investigation map rather than closing the case file |
Why bite case management data can become outbreak geography
Integrated Bite Case Management is not a laboratory substitute. Its value is that it records the messy chain of events that usually reaches public health before a confirmed rabies diagnosis does: an animal bite, a report, an interview, a decision about the animal, an assessment of exposure risk, and a follow-up pathway. In low-resource settings, those investigations may be the only systematic trace of transmission pressure.
A model trained on these records is not learning rabies biology from scratch. It is extracting spatial and epidemiologic patterns from investigations that field teams already perform. When many bite investigations share features associated with confirmed rabies risk, the model can flag a community as high risk even when no diagnostic sample has ever moved through a laboratory pipeline from that place.
That mechanism is why the eight newly identified communities matter. They were not merely additional dots on a model output. They represented locations where the official laboratory-confirmed map had no diagnostic infrastructure through which rabies risk could become visible.[1] In a dashboard, such places can look reassuringly blank. In the field, blank can mean unmeasured.
The same study’s ORED risk-stratification framework produced a 3.2-fold increase in epidemiologically useful data compared with routine IBCM-based surveillance and identified 12% more at-risk communities.[1] Those gains are not abstract performance claims. More usable data can change which communities receive investigation time, where vaccination campaigns are considered, and which suspected transmission chains are treated as public health priorities.
The model depends on the field system it improves
The attractive version of this story is that machine learning fills a diagnostic gap. The more accurate version is that machine learning reuses the surveillance work already being done and makes some of its latent signal easier to act on. If bite investigations stop, if case definitions drift, if follow-up quality declines, or if geographic coverage narrows, the model’s inputs degrade with them.
That dependency should shape adoption. A high-specificity model can help avoid sending scarce field teams everywhere. A model with sensitivity of 0.78 cannot justify ignoring places it does not flag.[1] Negative predictions may be reassuring within the study data, but they are not a license to let surveillance decay, especially outside the setting where the method was validated.
For public health teams, the useful sequence is therefore not automated: maintain IBCM reporting, run risk stratification, review high-risk signals, investigate in the field, and feed what is learned back into surveillance practice. The model changes the order in which places demand attention. It does not remove the need to verify what is happening there.
- Use the model output to prioritize field investigation, not to declare community-level safety.
- Treat newly flagged communities without diagnostic infrastructure as surveillance-equity priorities.
- Keep IBCM inputs stable enough that changes in model output reflect risk rather than reporting collapse.
- Reassess calibration and performance before transferring the approach to another country or surveillance system.
What the Haiti result does and does not generalize to
The global need is clear. Rabies causes approximately 59,000 deaths each year, with 95% occurring in Africa and Asia, and the World Health Organization’s “Zero by 30” target aims to end human deaths from dog-mediated rabies by 2030.[2] CDC public materials likewise frame rabies as a preventable but deadly disease where timely post-exposure care is central to prevention.[3]
But the validation setting in the cited machine learning study is Haiti. The results should not be treated as proof that the same model will perform the same way in sub-Saharan Africa, South Asia, Southeast Asia, or any other endemic setting. Different bite reporting systems, dog ecology, care-seeking behavior, sample transport capacity, and public health staffing could all change the relationship between IBCM data and confirmed rabies risk.
The funding and deployment context also matters. A Global Biodefense report described the work as supported through the Global Health Security Agenda and emphasized that the model is designed to complement, not replace, field investigation.[4] That is the right boundary for a research-stage public health AI method.
In ClinicalMind’s clinical-applications frame, this belongs as surveillance informatics rather than individual clinical guidance. It is not an FDA-cleared clinical tool, not a post-exposure prophylaxis decision engine, and not a substitute for local rabies exposure assessment. Its relevance to PEP is upstream: better detection of transmission zones can help public health systems recognize where exposure risk is being missed.
The adoption boundary
The Haiti study shows that an XGB model trained on bite case management data can make hidden rabies transmission zones visible when laboratory-confirmed surveillance has blind spots. The strongest evidence is the 20 high-risk clusters identified by the model compared with 12 from laboratory-confirmed data alone, including eight communities without prior diagnostic infrastructure.[1]
The same evidence sets the limit. This approach needs maintained IBCM inputs, continued field investigation, careful calibration, and external validation beyond Haiti. Used that way, the model can widen the surveillance map. Used as a shortcut around the public health system that generated its data, it would recreate the same invisibility in a more technical form.
References
- Machine learning to improve the understanding of rabies epidemiology in low surveillance settings, Scientific Reports, https://pmc.ncbi.nlm.nih.gov/articles/PMC11519585/
- WHO Rabies Epidemiology and Burden of Disease, World Health Organization, https://www.who.int/teams/control-of-neglected-tropical-diseases/rabies/epidemiology-and-burden-of-disease
- About Rabies, Centers for Disease Control and Prevention, https://www.cdc.gov/rabies/about/index.html
- Seeing the Invisible: How Machine Learning Is Closing Rabies Surveillance Gaps in Haiti, Global Biodefense, July 6, 2026, https://globalbiodefense.com/2026/07/06/seeing-the-invisible-how-machine-learning-is-closing-rabies-surveillance-gaps-in-haiti/
Comments
Join the discussion with an anonymous comment.