A deployed clinical model can keep a reassuring AUROC and F1 score while the patients, images, devices, workflows, or labels moving through it have already changed. That is the uncomfortable finding at the center of healthcare AI model drift monitoring: the standard dashboard may be measuring downstream performance too late, too coarsely, or only where labels are available.
Kore et al. made that failure mode hard to dismiss. In a Nature Communications study of 239,235 chest X-rays, macro-average AUROC and F1 changed by less than 3% even when significant COVID-era data drift was present. At Trillium Health Partners, data-based drift detection using an autoencoder and black-box shift detection identified COVID-19-driven drift months before any performance metric changed enough to raise the same concern.[1]
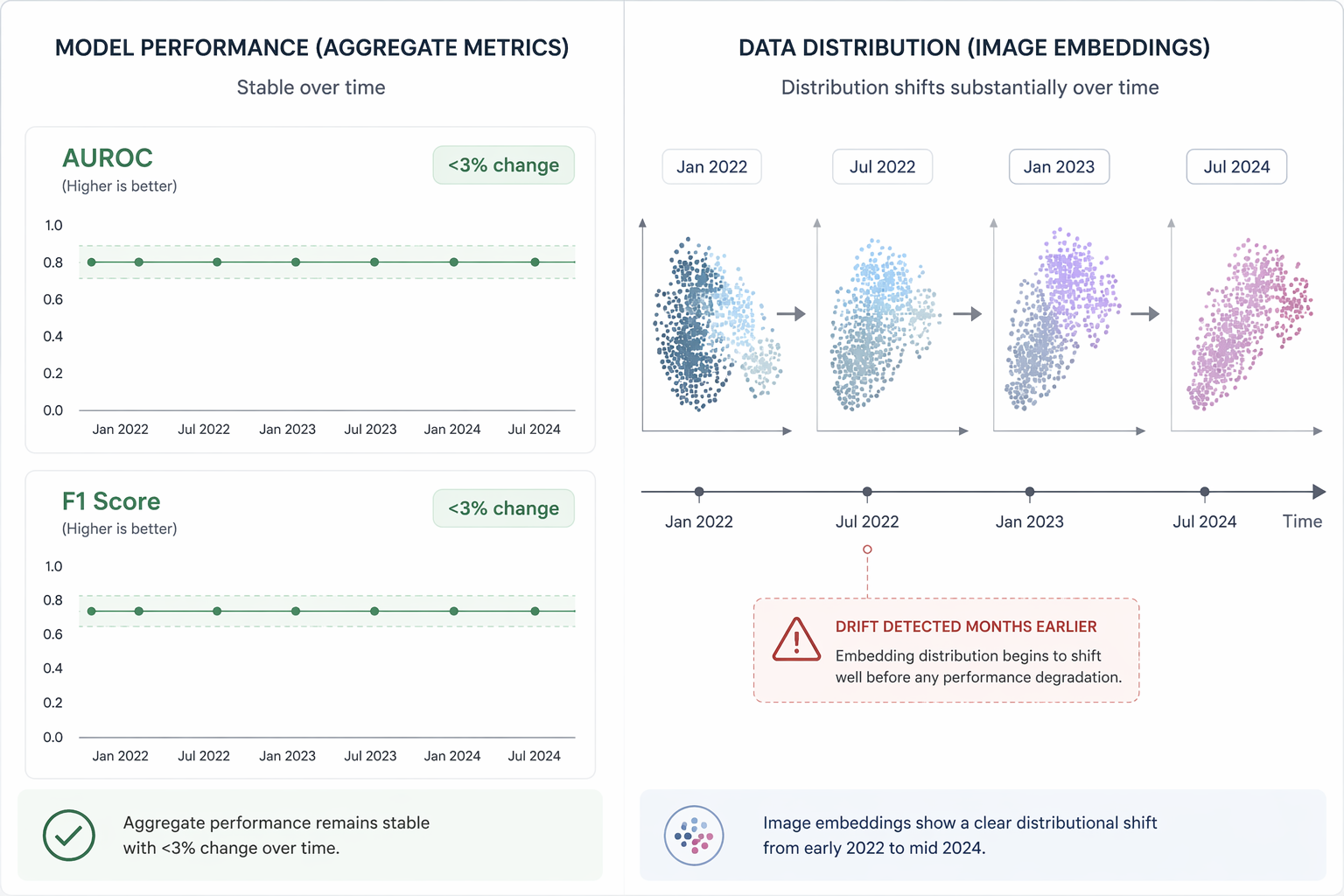
That is not a minor monitoring preference. It means an oversight committee could look at the conventional summary metrics, see stability, and still be missing a clinically relevant change in the incoming data stream. The model has not necessarily failed yet. The environment has moved first.
Why AUROC Can Stay Calm While the Data Moves
Aggregate performance metrics answer a narrow question: among the labeled cases evaluated, how well did the model separate or classify outcomes? That is useful, but it is not the same as asking whether today’s input population still resembles the population the model learned from.
Several things can hide inside a stable AUROC. Case mix can shift while easy and hard examples average out. A subgroup can degrade while the total population looks acceptable. A new acquisition device can alter image characteristics without immediately changing enough labeled outcomes to move the summary score. Labels can arrive late, inconsistently, or after clinical workarounds have already changed the observed outcome.
Kore et al. is especially useful because it placed the two forms of surveillance side by side. Performance monitoring looked at macro-average AUROC and F1. Data-based monitoring looked for distributional change in the X-ray data itself. During the COVID-19 period, the latter detected drift earlier than the former.[1]
This distinction matters operationally. If the only escalation rule is “call us when AUROC drops,” the hospital has chosen to wait for a downstream symptom. In a clinical workflow, that can mean clinicians spend weeks or months explaining away strange alerts, site reliability teams chase supposed integration problems, and governance committees receive a green metric that does not describe the thing staff are seeing.
The Same Problem Appears From Different Directions
The chest X-ray result is not an isolated warning. Other studies put pressure on the same assumption from different angles: scanner source, time, real-world workflow, and multi-modal signal agreement.
| Evidence | What Changed | Why Performance Monitoring Alone Was Not Enough |
|---|---|---|
| Kore et al., chest X-rays | COVID-era input distribution shifted across 239,235 images | Macro-average AUROC and F1 changed less than 3% while data-based methods detected significant drift months earlier.[1] |
| De Fauw et al., OCT imaging | Scanner type changed | A model trained on one OCT scanner type had a 5.5% error rate on that type but 46.6% on another scanner type.[2] |
| Nestor et al., MIMIC-III | Historical training data were tested against future data | Models had up to a 0.29 AUC drop when evaluated on later data.[3] |
| University of Michigan sepsis alert | Demographic shifts affected alert behavior during the early COVID-19 period | The hospital deactivated the sepsis-alerting model in April 2020 after spurious alerts emerged.[4] |
| MGH MMC+ framework | Multi-modal concordance changed | When the concordance metric exceeded 10, the share of AUROC values within 3 standard deviations of baseline fell from over 90% to under 50%.[5] |
The De Fauw finding is a clean reminder that “validated” can quietly mean “validated within one machine ecology.” The model’s behavior changed sharply when the OCT scanner type changed: 5.5% error on the scanner type used in training, 46.6% on a different scanner type.[2] Nothing about that result requires hostility toward AI. It requires admitting that a deployment site’s equipment is part of the model’s operating environment.
Nestor et al. adds time as a deployment variable. Models trained on historical MIMIC-III data lost as much as 0.29 AUC when tested on future data.[3] That is not the same mechanism as a scanner mismatch, and it should not be collapsed into a generic statement that “models get worse.” It says that a model trained on one period can face a different clinical data-generating process later.
The University of Michigan sepsis-alerting case shows why this is more than a benchmarking issue. During the early COVID-19 period, demographic shifts contributed to spurious alerts, and the hospital deactivated the model in April 2020.[4] That is the moment monitoring leaves the research slide and enters staffing, trust, escalation, and patient-care operations.
What Data-Based Monitoring Adds
Data-based drift detection watches the incoming data distribution rather than waiting for final labeled performance. In imaging, that may involve learned embeddings or reconstruction-based signals. In tabular models, it may involve feature distributions, missingness, coding patterns, device feeds, demographic mix, or other inputs that can shift before the outcome label is known.
Its value is not that it proves clinical harm. It does not. Its value is that it can detect a change in the model’s operating conditions early enough for someone to investigate whether the change is benign, expected, or dangerous. In Kore et al., that distinction was decisive: the data-based methods saw COVID-era drift before the aggregate performance metrics moved.[1]
The MMC+ framework from MGH points to another monitoring idea: concordance across modalities. In that work, once a multi-modal concordance metric exceeded 10, the proportion of AUROC values remaining within 3 standard deviations of baseline dropped from over 90% to under 50%.[5] That does not make concordance a universal alarm threshold, but it does show why monitoring can benefit from signals that are closer to the data stream than a single end-stage accuracy statistic.
A good drift signal changes the governance conversation. Instead of asking only whether the model is still “performing fine,” the committee can ask what changed: the input source, patient mix, workflow, label process, clinical practice, or outcome prevalence. Those are different questions with different owners.
Not Every Drift Is the Same Failure
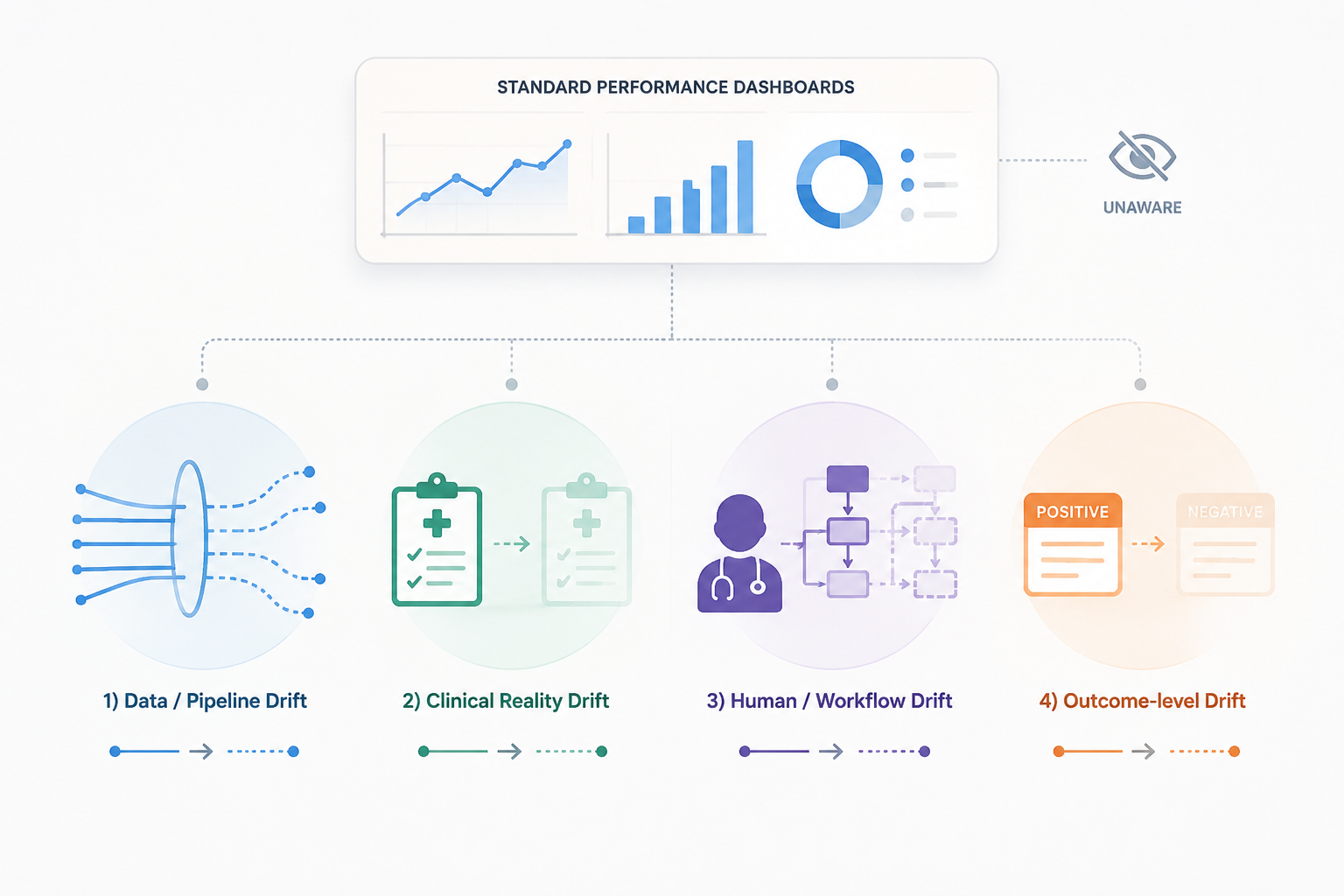
Drift becomes unmanageable when every change is described as “the model degraded.” The monitoring plan needs sharper language. A scalable drift monitoring review published in 2025 organizes the field around detection and correction methods, while an Atomic Object analysis separates healthcare AI drift into data or pipeline drift, clinical reality drift, human or workflow drift, and outcome-level drift.[6][7]
For clinical oversight, three distinctions are especially important:
- Data drift: the input distribution changes. A scanner, coding system, device feed, demographic mix, or referral pattern may shift while the relationship between inputs and outcomes remains similar.
- Concept drift: the relationship between inputs and the target changes. A feature that once predicted deterioration may mean something different after treatment protocols, testing behavior, or clinical practice changes.
- Label drift: the observed ground truth changes. This can happen when outcome definitions, documentation practices, adjudication rules, or follow-up completeness change.
These categories overlap in real deployments, but they should not be treated as interchangeable. Data drift can often be monitored without waiting for labels. Concept drift usually requires closer clinical interpretation because the same input may carry a different meaning. Label drift can make performance metrics themselves unstable, because the “truth” being used for evaluation has changed.
That is why AUROC and F1 are downstream indicators. They are still necessary; nobody should operate a clinical model without performance surveillance. But they do not tell the whole story of whether the data-generating process is still the one the model was built to handle.
The Sample-Size Problem
Data-based drift detection is not magic. Kore et al. found that sensitivity was strongly tied to sample size: with 500 images, the p-value never dropped below 0.1, while with 4,000 images the method detected a 40% enrichment.[1] That caveat belongs in every serious monitoring plan.
Small hospitals, rare-disease models, low-volume imaging services, and narrowly scoped specialty deployments may not generate enough observations for reliable statistical detection on a short cadence. A monthly drift dashboard can look sophisticated and still be underpowered. In those settings, governance needs to be honest about what the signal can and cannot resolve.
That does not argue against drift monitoring. It argues against pretending that every detector works equally well at every scale. Low-volume deployments may need longer aggregation windows, pooled monitoring across similar sites, stronger qualitative workflow surveillance, targeted audits after known operational changes, or predefined review after device, protocol, or population shifts.
Vendor Monitoring Is Moving, But Evidence Still Matters
Vendor governance discussions are beginning to reflect these concerns. Censinet’s guide to AI model drift monitoring describes vendor monitoring requirements and cites a 16% governance statistic, along with a population stability index threshold of PSI greater than 0.25 as a potential signal of significant shift.[8] Those kinds of thresholds can help procurement and risk teams ask more concrete questions.
They should not become a substitute for local evidence. The same Censinet material cites a claim that 91% of models lose effectiveness from a third-party source, magai.co, rather than presenting it as independently verified healthcare evidence.[8] That distinction matters. Vendor risk language can sharpen oversight, but it should not outrank empirical monitoring results from the actual deployment environment.
The practical vendor question is not simply whether monitoring exists. It is what the monitoring watches, how often it runs, how much data is needed before it is interpretable, which drift types it can detect, who receives alerts, and what happens when a data-based signal conflicts with a stable AUROC.
What Reliable Oversight Has to Watch
The evidence does not support abandoning performance metrics. AUROC, F1, calibration, sensitivity, specificity, subgroup performance, and alert burden all remain important. The error is treating any one of them as a smoke alarm for every kind of drift.
Reliable healthcare AI model drift monitoring needs at least four forms of discipline. First, it must monitor the incoming data distribution, not just labeled outcomes. Second, it must name the suspected drift type rather than folding data, concept, and label changes into one vague degradation story. Third, it must account for sample size before interpreting a quiet detector as evidence of stability. Fourth, it must define escalation rules for situations where the data moves before AUROC admits anything is wrong.
That last point is where many dashboards fail. A clinically meaningful shift may first appear as a new scanner, a changed order set, a different patient mix, an altered documentation pattern, or a wave of clinician overrides. By the time aggregate performance metrics move, the workflow may already have absorbed the damage.
The better posture is not alarmism. It is earlier visibility. Performance metrics tell oversight teams how the model performed on evaluated cases. Data-based drift detection tells them whether the ground under those cases is still recognizably the same.
References
- Data drift in medical machine learning: implications and potential remedies, Nature Communications, 2024, link
- Clinically applicable deep learning for diagnosis and referral in retinal disease, Nature Medicine, 2018, link
- Feature robustness in non-stationary health records: caveats to deployable model performance in common clinical machine learning tasks, Proceedings of Machine Learning Research, 2019, link
- Unexpected Consequences of Electronic Health Record–Based Predictive Models, New England Journal of Medicine, 2021, link
- MMC+: Multimodal Monitoring of Clinical AI, arXiv, 2024, link
- Scalable Drift Monitoring in Medical Machine Learning, arXiv, 2025, link
- Drift Monitoring in Health AI, Atomic Object, link
- AI Model Drift Monitoring: Ensuring Ongoing Performance of Healthcare AI Vendors, Censinet, link
Comments
Join the discussion with an anonymous comment.