No single federal statute expressly says a clinic must obtain patient consent before using an ambient AI scribe. That is the part many rollout conversations get right. The part they too often get wrong is treating that absence as permission to turn the tool on with only a vendor script and a quiet line in the intake packet. For patient consent for ambient AI scribe use in 2026, the safer answer is more layered: HIPAA and business associate rules govern how protected health information is handled, state recording laws may govern the act of listening or recording, new AI-disclosure laws are beginning to add notice and opt-out requirements, and malpractice carriers are telling physicians to document consent even when statutes do not clearly require it.[1]
That does not mean every jurisdiction has the same legal rule. It means a practice that wants a durable policy should assume patients will be told, in plain language, that an ambient tool is being used; should document the patient’s response; and should verify the state-specific recording, AI-disclosure, privacy, and professional-liability rules before deployment. Family medicine clinics and other smaller practices have less room for ambiguity than large health systems with privacy engineers and in-house counsel. If a patient later complains, “I did not know AI was listening,” the chart, consent workflow, vendor file, and staff script need to tell the same story.

Start by separating the legal layers
Ambient AI scribe consent gets confusing because several legal categories are being pulled into the same exam room. They do not answer the same question.
| Layer | What it mainly asks | Why it matters before deployment |
|---|---|---|
| HIPAA and business associate agreements | May the vendor receive, create, maintain, or transmit protected health information for the clinic? | A vendor relationship may need a business associate agreement and privacy review, but HIPAA alone does not settle the patient-consent question. |
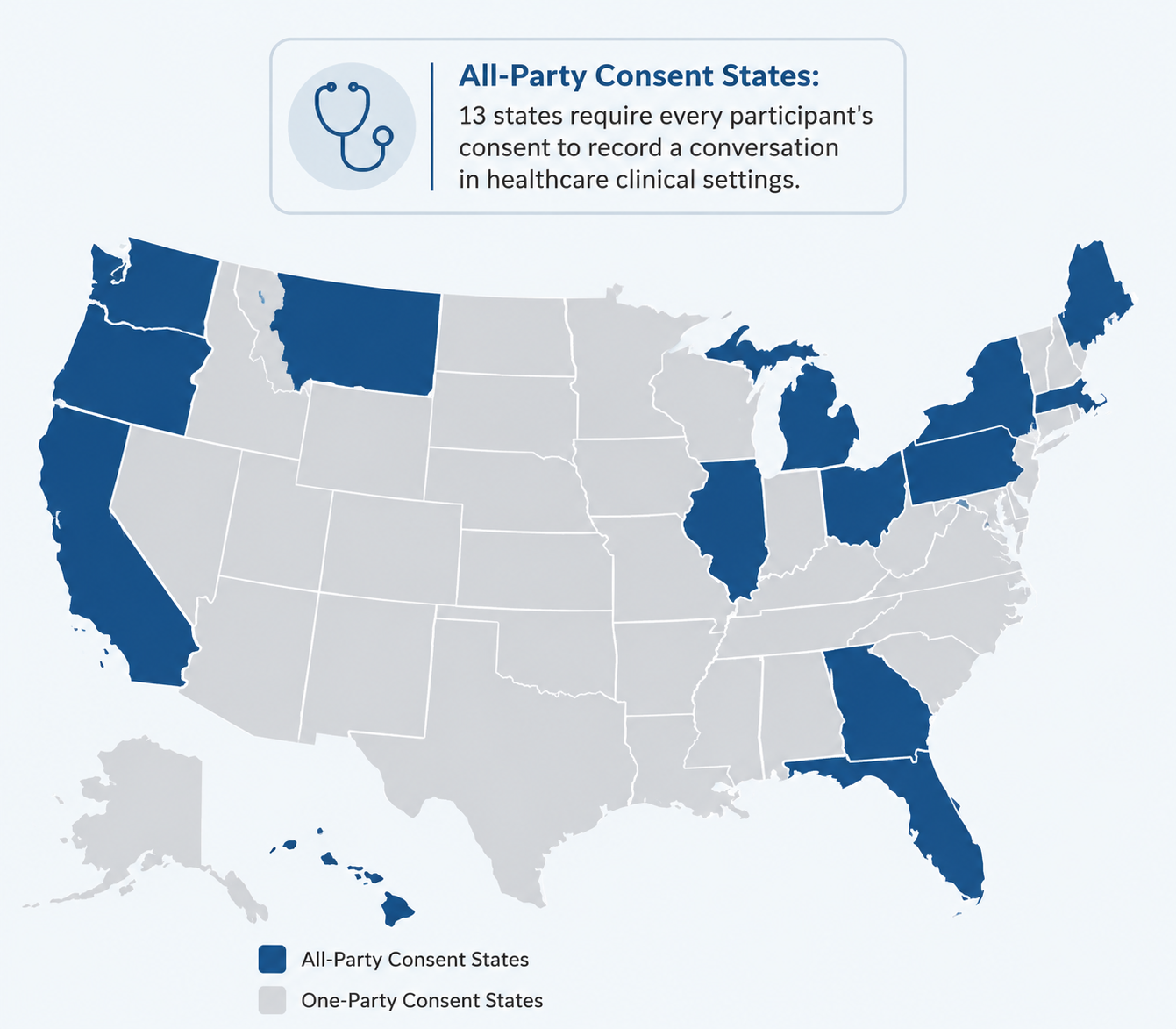
| State recording and wiretapping laws | May the conversation be recorded, intercepted, or captured without every participant’s consent? | All-party consent states create the most immediate concern when an ambient tool listens to or records a clinical encounter. |
| State AI-disclosure laws | Must patients be notified when generative AI is used in clinical communications or scribing? | New statutes are appearing state by state, with unresolved questions about how they apply to clinician-reviewed ambient notes. |
| Malpractice and risk management guidance | Would the practice’s process look reasonable if documentation, consent, or accuracy is later challenged? | Carrier guidance may raise the practical risk floor even where a statute is silent. |
The American Bar Association’s Health Law analysis frames the problem this way: HIPAA, state wiretapping statutes, privacy and cybersecurity obligations, and emerging state AI laws all have to be considered together, but none of them produces a simple nationwide consent rule for ambient AI scribes.[1] The family medicine-focused analysis from the North Carolina Academy of Family Physicians and Fish similarly notes that no federal law yet directly addresses ambient scribe consent, while warning clinics that state recording laws still apply.[2]
HIPAA is necessary, but it is not the whole consent answer
HIPAA matters because ambient scribes handle clinical information. Depending on the product design, the vendor may receive audio, transcripts, draft notes, encounter metadata, or other protected health information. A clinic therefore has to ask the ordinary HIPAA questions: Is the vendor acting as a business associate? Is there a signed business associate agreement? What data is collected, stored, transmitted, retained, de-identified, or used to improve the product? Who can access it? What happens after termination?
PrivaPlan’s clinic compliance guide emphasizes the need to evaluate AI ambient scribe vendors through HIPAA readiness, business associate agreement terms, privacy policies, security safeguards, and staff training before clinical use.[3] That is not busywork. If the vendor is creating or maintaining PHI on behalf of the practice, the BAA is the paper trail that shows the clinic treated the relationship as a regulated health information relationship rather than a plug-in productivity tool.
But HIPAA compliance does not automatically answer whether the patient had to agree to the tool’s presence in the room. HIPAA can permit certain uses and disclosures for treatment, payment, and healthcare operations without a separate HIPAA authorization. That is different from saying a state recording law, AI-notification statute, professional ethics expectation, or malpractice carrier will be satisfied by silence. The consent analysis has to continue beyond HIPAA.
Recording law is where many clinics should slow down
The most operationally urgent question is often not whether the note is generated by AI. It is whether the encounter is being recorded, captured, or intercepted in a way that triggers state wiretapping or eavesdropping law. A clinic in a one-party consent state may face a different baseline than a clinic in an all-party consent state, but the difference should be confirmed before anyone trains staff to say, “We do not need consent here.”
Zentake’s state-law analysis identifies 13 all-party consent states where recording a clinical conversation without every participant’s consent could violate state wiretapping statutes.[4] That number is useful as an orientation point, not as a substitute for legal review. State recording laws vary in wording, definitions, exceptions, and remedies; the product’s technical design also matters. A tool that streams audio for processing, one that stores audio, one that immediately converts speech to text, and one that only keeps a clinician-approved draft may not present the same risk profile.
No federal court has yet resolved whether ambient AI scribe recording triggers state all-party consent wiretap statutes, and litigation in California and Illinois remains pending.[1] That uncertainty cuts against casual deployment. It is one thing to conclude, after counsel reviews the tool and state law, that a particular workflow is permissible. It is another to let a sales deck turn a disputed legal category into a front-desk assumption.
For a practice operating across state lines, the policy should not be built around the most permissive location. Staff need to know what rule applies where the encounter occurs, including telehealth visits. If the practice cannot reliably operationalize different scripts by jurisdiction, a universal documented-consent approach may be simpler than a technically narrower policy that staff cannot execute consistently.
AI-disclosure laws are adding a separate notice layer
State AI laws do not merely repeat recording law. They may focus on whether generative AI is being used, whether the patient is receiving AI-generated clinical communication, whether a human clinician reviewed the output, or whether the patient has a right to opt out.
California AB 3030, effective January 2025, requires disclosure when generative AI is used to generate patient communications concerning patient clinical information, unless the communication is reviewed and approved by a licensed or certified healthcare provider.[5] For ambient scribes, the unresolved issue is the exemption. If the tool drafts a note that a clinician reviews before it becomes part of the chart, does that keep the workflow outside the statute’s notification requirement? Or does some patient-facing output still require disclosure? The Medical Board of California’s summary confirms the review-and-approval exemption, but it does not eliminate interpretive questions for every ambient scribe configuration.[5]
Rhode Island has moved more directly toward ambient scribe notice. Healthcare IT News reported in 2026 that Rhode Island became the fourth state to specifically mandate patient notification and opt-out rights for ambient AI scribing.[6] Because the law is new, implementation guidance has not yet filled in all the practical details. Clinics should be careful about copying an early summary into policy language and treating it as the final operating manual.
This is why “we are in a one-party consent state” is not the end of the analysis. A one-party recording rule may reduce one category of risk while an AI-disclosure or opt-out statute creates another. The cleaner compliance question is not, “Can we avoid asking?” It is, “What combination of disclosure, consent, refusal handling, documentation, and vendor controls will still look coherent if the rule changes or a regulator asks how we made the decision?”
Malpractice guidance raises the practical floor
Malpractice carriers are not legislatures, and their risk guidance is not the same thing as a binding statute. Still, practices ignore carrier guidance at their own peril. If a note is later challenged, the relevant question may not be limited to whether a consent statute technically applied. The question may become whether the physician used the tool reasonably, reviewed the output, corrected errors, protected confidentiality, and made the patient aware enough that the process was not misleading.
TMLT’s 2026 risk management guidance recommends documented patient consent for AI medical scribes regardless of whether a statute requires it.[7] The recommendation sits in the same practical bucket as documenting clinician review of AI-generated notes and maintaining a process for accuracy corrections: it creates a record of reasonable behavior when the legal standard is still forming.
The AMA Journal of Ethics makes the ethical distinction more carefully than many policy templates do. It argues that current informed consent doctrine, as developed for medical treatment, may not neatly extend to documentation technology, and that ambient listening and transcription may call for a distinct transparency framework.[8] That matters because consent for an AI scribe is not consent to a procedure, medication, or surgery. Patients are being asked to allow a documentation technology into a conversation that may include mental health history, family conflict, substance use, immigration concerns, sexual health, or financial stress. A rote checkbox does not carry that weight well.
A defensible workflow for patient consent
A consent workflow for an ambient AI scribe should be built for the people who have to use it at 8:15 on a full clinic morning. The medical assistant needs words that are accurate but not legalistic. The physician needs to know what to do if the patient says no. The practice manager needs proof that staff were trained. The compliance file needs the vendor review, the BAA, and the final script in the same universe.
At a minimum, the workflow should cover six actions:
- Disclose before use that an ambient tool will listen to or process the visit to help create clinical documentation.
- Identify the purpose in ordinary language: the tool assists with note drafting or documentation, not independent diagnosis or treatment decision-making unless the practice has separately validated and approved another use.
- Explain human review where applicable, including that the clinician remains responsible for reviewing, correcting, and signing the note.
- Offer refusal or opt-out where required by law and, in many settings, as a prudent default even if the practice believes refusal is not legally required.
- Document the patient’s response in a consistent location, including refusals and any visit-specific limitations.
- Align the vendor relationship through a BAA, privacy and security review, data-retention review, and staff training before go-live.
That workflow is not a universal legal safe harbor. It is a defensible minimum posture across uncertainty. A practice may need stronger language in an all-party consent state, an opt-out mechanism in a state with an ambient-scribe statute, or special handling for minors, behavioral health visits, reproductive health visits, interpreter use, or group encounters where more than one person is in the room.
What the script should say
The script does not need to sound like a vendor license agreement. It does need to be specific enough that the patient understands what is happening. A workable version might say: “We use a secure documentation tool that listens during the visit and helps draft the medical note. Your clinician reviews and edits the note before it becomes part of your record. You can ask us not to use it for your visit.”
That example is intentionally generic. A real script should be revised for the specific product, state law, specialty, patient population, and workflow. If the vendor stores audio, uses encounter data for model improvement, sends data through subcontractors, or produces patient-facing summaries, the disclosure may need more detail. If the tool does not store audio, the practice should avoid saying it records audio unless that is technically true. Accuracy matters on both sides; overstating the risk can mislead patients just as much as understating it.
Where to document the answer
Consent should not live only in staff memory. The practice should decide where the response goes: a discrete EHR field, a visit-level attestation, a consent form, a rooming template, or another auditable location. The location matters because later review rarely happens under calm conditions. If the patient complains, the practice should not have to reconstruct consent from a sticky note, a training email, and a clinician’s recollection.
Refusal needs a workflow too. If a patient declines the ambient scribe, staff should know whether to turn off the tool, remove the device, pause recording, switch to manual documentation, or reschedule only if the visit genuinely cannot proceed without the technology. Refusal should not be treated as a disruption. It is part of the consent design.
Transparency can lower acceptance, so plan for that honestly
The hardest operational truth is that fuller disclosure may reduce patient acceptance. Lawrence et al. reported in JAMA Network Open in July 2025 that consent dropped by 26 percentage points when full AI details were disclosed.[9] That finding should not be used as an argument for vague notice. It should be used as a staffing and rollout warning: if a practice gives patients meaningful information, some patients will say no.
That drop-off creates real pressure. Clinicians want relief from documentation burden. Managers want the subscription to justify itself. Vendors want adoption. But a consent process designed to preserve acceptance by hiding the part patients care about is not a stable compliance strategy. The better response is to prepare for refusals: keep manual documentation available, train staff not to argue, and monitor whether refusal rates differ by location, language, age, visit type, or clinician.
The study measures a consent response under disclosure conditions; it does not prove that every clinic will lose the same share of patients, and it does not answer the legal question by itself.[9] Its value is more practical. It reminds practices that transparency has a cost, and that the cost belongs in the implementation plan rather than being discovered by the front desk after go-live.
The policy should survive ambiguity
A durable ambient scribe policy should name the uncertainty instead of smoothing it away. California’s AB 3030 leaves questions about clinician-reviewed outputs. Rhode Island’s ambient scribe opt-out law is recent enough that implementation guidance still matters. Pending California and Illinois lawsuits may clarify how recording laws apply, but they have not done so yet. Carrier recommendations are influential, not binding. Those are not footnotes; they are the operating environment.
Before turning on the tool, a clinic should be able to answer these questions without calling three people in a panic:
- What exactly does the tool capture during the encounter: audio, transcript, draft note, metadata, or something else?
- Is audio stored, and if so, where, for how long, and who can access it?
- Does state recording law require all participants to consent for this workflow?
- Does any state AI-disclosure or ambient-scribe law require notice, opt-out, or specific wording?
- Has the vendor signed a BAA, and does the BAA match the product’s actual data practices?
- Where is the patient’s consent, refusal, or opt-out documented?
- Who reviews AI-generated draft notes, and how are errors corrected before signature?
For multi-site practices, the answers may not be identical across locations. For telehealth, the practice may need to account for where the patient is, where the clinician is, and which state’s recording or disclosure law applies. For visits involving family members, interpreters, trainees, or caregivers, the practice should decide whether everyone in the room must be told and whether everyone must agree. These details are where a polished policy becomes a usable one.
A practical 2026 standard
The practical standard for 2026 is not that every ambient AI scribe workflow is legally identical, or that documented consent guarantees compliance. It is that a practice should be reluctant to deploy an always-listening documentation tool without clear patient-facing disclosure, a recorded patient response, a refusal path, clinician review of the output, and a vendor file that supports the privacy promises being made in the exam room.
In one-party consent jurisdictions, documented consent may be more conservative than the narrowest possible reading of recording law. In all-party consent states, it may be essential. In states adopting AI-specific notice or opt-out laws, it may need to be paired with required statutory language or workflow rights. Across all of them, it gives the practice a better answer when a patient, regulator, plaintiff’s lawyer, or malpractice carrier asks what the patient was told before AI entered the room.
The law is still moving state by state. Practices should verify local requirements before deployment and revisit the policy as the California and Illinois litigation develops, Rhode Island implementation guidance emerges, and AI-disclosure interpretations mature. Until then, plain-language disclosure and documented consent are not just a legal hedge. They are the most workable way to protect the clinic staff and clinicians who will have to stand behind the rollout after the vendor demo is over.
References
- Ambient AI Scribes: Privacy & Cybersecurity, American Bar Association, 2026, link
- Legal & Ethical AI Ambient Scribe Tools for Family Medicine Clinics, NCAFP, 2026, link
- AI Ambient Scribes: Is Your Health Care Clinic Ready?, PrivaPlan, 2026, link
- Consent for AI Scribe Use, Zentake, link
- Notice to Consumers Regarding Use of Generative Artificial Intelligence, Medical Board of California, link
- Rhode Island passes ambient AI scribe opt-out law, Healthcare IT News, link
- Using AI medical scribes: Risk management considerations, TMLT, 2026, link
- How Should We Think About Ambient Listening and Transcription Technologies’ Influences on EHR?, AMA Journal of Ethics, November 2025, link
- Lawrence et al. JAMA Network Open study, JAMA Network Open, July 2025, link
Comments
Join the discussion with an anonymous comment.