“Sugar-free” is a useful label for carbohydrate counting, but it is a poor synonym for metabolically inert. The more interesting question for sugar-free candy’s digestive health effects is not whether every non-nutritive sweetener behaves like sugar. It is whether some people carry a baseline gut ecology that makes them more likely to show measurable glycemic or microbiome shifts after exposure.
The strongest evidence for asking that question still comes from the 2022 randomized trial by Suez and colleagues, which enrolled 120 healthy adults and assigned them to saccharin, sucralose, aspartame, stevia, or placebo sachets over two weeks, at doses below the acceptable daily intake. Saccharin and sucralose impaired glucose tolerance in the human participants, while all four tested sweeteners altered stool and oral microbiome composition or function.[1]
That distinction matters. The trial did not show that every sweetener caused the same metabolic outcome. It did show that the microbial response was not a decorative side finding. The investigators used shotgun metagenomic sequencing and TCAM trajectory analysis to track changes across stool and oral samples, then asked whether the altered microbiome could carry the phenotype into another host.[1]
The Human Signal Came First
In nutrition studies, it is easy to overread a microbiome shift. Sequencing can detect movement that is biologically real but clinically vague. The Suez trial is more compelling because the evidence chain started with a human metabolic readout: glucose tolerance worsened after saccharin and sucralose exposure, but not significantly after aspartame or stevia in the same trial structure.[1]
The exposure also deserves careful wording. This was not a trial of finished sugar-free candy products. Participants consumed commercial sweetener sachets, and those sachets contained glucose as a bulking agent.[1] That does not erase the finding, but it does keep the conclusion narrower than many headlines would prefer. A candy matrix can add polyols, fibers, flavoring systems, fats, and dose patterns that were not tested here.
For clinicians, the practical issue is still familiar. Saccharin and sucralose appear in sugar-free products, including some candies, gums, and tabletop substitutes. If these compounds can impair glucose tolerance in some healthy adults over a short exposure window, they deserve more caution than a simple “non-caloric” category implies. But the trial does not justify telling every patient that every sugar-free candy will disrupt their metabolism.
Microbiome Change Was Not Just a Statistical Ornament
All four non-nutritive sweeteners in the Suez trial produced distinct changes in the microbiome, even when the glucose-tolerance result diverged. That is already a useful brake on sloppy interpretation. Microbiome disruption and glycemic impairment were related enough to investigate mechanistically, but they were not identical outcomes.
The oral microbiome is often treated as peripheral in discussions of sweeteners, yet the trial measured both oral and stool communities. That matters because sweetener exposure begins in the mouth, and microbial functional shifts can occur before any intestinal readout becomes visible. The study’s TCAM trajectory analysis allowed the investigators to compare how each participant’s microbial profile moved over time rather than relying only on a before-and-after average.[1]
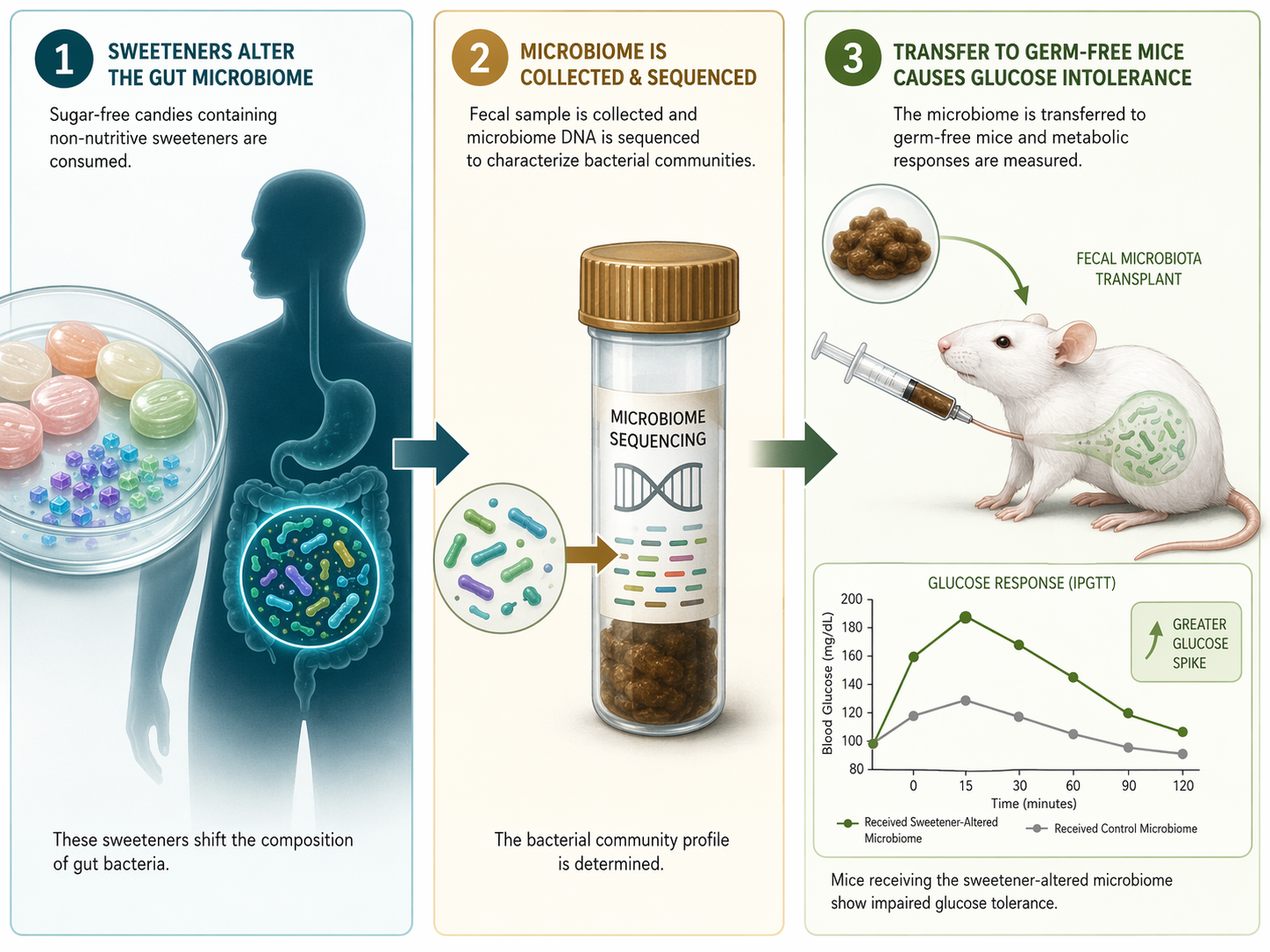
The most persuasive step was the fecal microbiome transfer into germ-free mice. When microbiomes from human sweetener consumers were transferred, the glycemic impairment phenotype could be transferred as well.[1] This is the point where the mechanism becomes harder to dismiss as a sequencing artifact. A transferred phenotype in germ-free mice does not make the human result universally generalizable, but it gives the microbial mediation argument physical weight.
What the Models Were Actually Predicting
The machine learning component of the Suez trial is often the most tempting part to oversell. The models did not look at a person’s microbiome and issue a clinically validated sweetener prescription. They analyzed whether baseline metagenomic, metabolomic, and clinical features were associated with later glycemic response after sweetener exposure.[1]
That is still important. Baseline features are measured before exposure, so they can function as candidate predictors rather than merely post hoc damage markers. The investigators reported that baseline abundance of glycolysis pathway genes, purine biosynthesis genes, TCA cycle metabolites, and specific species including Prevotella copri and Bacteroides xylanisolvens were linked to subsequent glycemic response.[1]
| Baseline signal | Why it matters for interpretation |
|---|---|
| Glycolysis pathway gene abundance | Suggests that pre-existing microbial carbohydrate-processing capacity may relate to later glucose-tolerance response. |
| Purine biosynthesis genes | Points to baseline microbial functional state rather than only species presence. |
| TCA cycle metabolites | Connects microbial ecology with host-relevant metabolic pathways. |
| Prevotella copri | A species-level feature associated with later glycemic response in the study dataset. |
| Bacteroides xylanisolvens | Another species-level feature reported among baseline predictors. |
The glycolysis signal is especially plausible because it sits close to the biological question. A microbial community already enriched for carbohydrate-processing pathways may respond differently when exposed to a sweet-tasting compound delivered with a glucose bulking agent. But plausibility is not validation. A pathway can help explain variance in a dataset without being ready to stratify patients in clinic.
Prevotella copri deserves the same restraint. Its presence in a predictive feature set does not mean it is a universal “bad responder” marker for sucralose, saccharin, or sugar-free candy. It means that, in this controlled short-term study, baseline abundance of this species helped distinguish participants who later showed different glycemic responses.[1]
For readers interested in clinical AI, this is a familiar boundary. A model can sharpen a hypothesis before it becomes a decision tool. The same distinction shows up in broader discussions of AI for athlete diet optimization, where prediction tasks are often easier to demonstrate than safe individualized guidance.
Why Predictive Does Not Yet Mean Prescriptive
A baseline microbiome model becomes clinically useful only after it survives a harder test: prospectively identifying people at risk before they consume the sweetener, in a population unlike the one used to discover the signal. The Suez trial was randomized and mechanistically rich, but it included 120 healthy adults and followed a two-week exposure window.[1] That is not a weakness for discovery. It is a limitation for deployment.
The glucose bulking agent in the sweetener sachets is another design constraint. If a model learns response patterns under an exposure that combines a non-nutritive sweetener with glucose, it may not behave the same way when the exposure is a pure compound, a lozenge, a chocolate-like candy, or a mixed diet pattern. For sugar-free candy specifically, digestive effects may also involve ingredients not evaluated in the trial.
There is also a basic distinction between microbiome alteration and clinical harm. Aspartame and stevia altered microbiome composition or function in the trial, but they did not significantly impair glucose tolerance in the same way as saccharin and sucralose.[1] If a future model treats any detectable microbial movement as a reason to warn a patient away from a product, it will confuse sensitivity with usefulness.
In practical terms, the model output is best treated like an instrument reading inside a study, not a verdict. It can tell researchers where to look: which microbial pathways, species, and metabolites may shape susceptibility. It cannot yet tell a gastroenterologist that a particular patient will tolerate sucralose-containing candy while another should avoid it.
The 2026 RCT Meta-Analysis Widens the Frame
The 2026 Tufts summary of a meta-analysis of 21 randomized controlled trials adds weight to the concern without replacing the mechanistic value of the Suez trial. It reported that non-nutritive sweetener consumption raised fasting insulin and HbA1c, with gut microbiome disruption proposed as a mechanism.[2]
That broader RCT signal is useful because it moves the discussion beyond a single experiment. Fasting insulin and HbA1c are clinically recognizable endpoints, and randomized trials reduce some of the confounding that shadows observational diet research. Still, a meta-analysis can accumulate effect estimates without resolving who is susceptible, which sweetener matters most, or which microbial feature carries the response.
This is where the two evidence streams fit together. The 2026 synthesis supports caution that non-nutritive sweeteners can affect metabolism and gut health. The 2022 trial supplies a more granular chain: human glycemic response, microbial alteration, germ-free mouse transfer, and baseline predictors. One broadens confidence; the other explains why a personalized prediction model is biologically plausible.
What This Means for Sugar-Free Candy Research
For sugar-free candy, the honest conclusion is narrower than either reassurance or alarm. Non-nutritive sweeteners used in these products cannot be assumed to be metabolically silent. Saccharin and sucralose, in particular, have human trial evidence of impaired glucose tolerance under the tested conditions, while saccharin, sucralose, aspartame, and stevia all altered microbiome composition or function in the Suez study.[1]
Machine learning is most useful here as a way to prioritize mechanisms and design better trials. A strong next-generation study would prospectively enroll a larger and more diverse cohort, measure baseline metagenomic and metabolomic features, assign cleaner sweetener exposures, and test whether pre-specified predictors such as glycolysis pathway abundance or Prevotella copri actually identify people who develop glycemic impairment.
That design problem resembles the broader challenge of using AI in clinical research: models can improve trial stratification and hypothesis testing before they are ready for bedside advice. The same caution applies across AI-enabled clinical trial design and digestive-health applications, where validation context determines whether an algorithm is informative or merely impressive.
For now, the evidence supports research prioritization rather than individual dietary prescribing. Baseline microbiome and metabolomic profiles can identify meaningful correlates of sweetener response. They do not yet justify clinical pre-screening for sugar-free candy tolerance.
Comments
Join the discussion with an anonymous comment.