For the search question “taylor farms lettuce recall 2025 affected states,” there are two separate Taylor Farms events to keep apart. The clinically more severe event was an E. coli O157:H7 romaine lettuce outbreak tied to 89 illnesses in 15 states, with 36 hospitalizations, 7 hemolytic uremic syndrome or kidney failure cases, and 1 death; those figures came from Food Safety News reporting on federal court filings, not from an FDA outbreak notice.[1] The broader state distribution came from a separate Honey Balsamic Salad Kit allergen recall listed by FDA in August 2025, involving undeclared sesame and soy across 25 states.[2]
| 2025 Taylor Farms event | Hazard | Relevant dates | Affected states | Evidence limit |
|---|---|---|---|---|
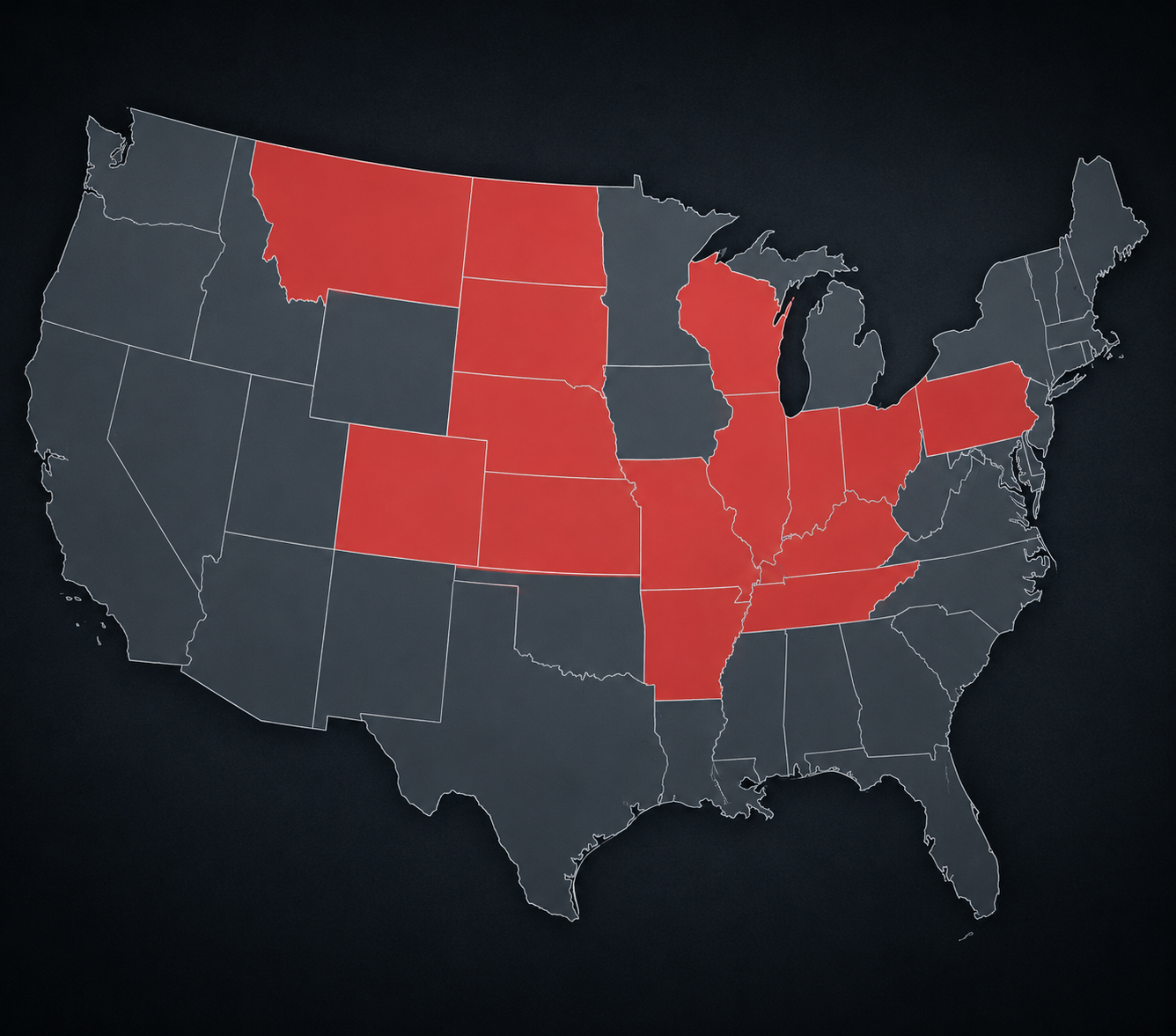
| Romaine lettuce outbreak | E. coli O157:H7 | Investigation period reported as Nov. 2024-Jan. 2025; Taylor Farms named in April 2025 reporting | AR, CO, IL, IN, KS, KY, MO, MT, ND, NE, OH, PA, SD, TN, WI | Case counts and state list came from Food Safety News reporting on court filings; FDA did not publish an official outbreak notice. |
| Honey Balsamic Salad Kit recall | Undeclared sesame and soy allergens | FDA recall notice dated Aug. 26, 2025; product dates in Aug.-Sep. 2025 recall window | AL, AZ, CA, CO, DE, FL, GA, IN, KS, KY, LA, MI, MO, MS, NJ, NY, OH, OR, PA, TN, TX, UT, VA, WA, WV | This was a labeled recall notice, not an infectious disease outbreak. |
That distinction matters for clinicians, laboratorians, and public health staff because the two events stress different parts of the safety system. An allergen recall can move through product labeling, distribution records, and retailer removal. A Shiga toxin-producing E. coli outbreak moves through patients, specimens, laboratory confirmation, jurisdictional reporting, traceback, and public disclosure. The latter is where AI-assisted clinical detection begins to look useful—and where it also runs into the limits of the reporting system around it.
The 15-State E. coli Event Is the One With Clinical Weight
The reported E. coli O157:H7 outbreak was not a minor traceback footnote. Food Safety News reported 89 cases across Arkansas, Colorado, Illinois, Indiana, Kansas, Kentucky, Missouri, Montana, North Dakota, Nebraska, Ohio, Pennsylvania, South Dakota, Tennessee, and Wisconsin; 36 people were hospitalized, 7 developed HUS or kidney failure, and 1 person died.[1] For a clinical laboratory, those numbers translate into more than a product name. They mean bloody diarrhea specimens, Shiga toxin testing, culture or molecular confirmation, isolate routing, case interviews, and delayed answers for infection prevention teams trying to understand whether a cluster is local or part of something larger.
The uncomfortable part is the provenance of the public information. The FDA did not publish an official outbreak notice for this event, and the case details became visible through Food Safety News and court-filed materials rather than the usual public outbreak page.[1] Northeastern University’s coverage quoted food safety expert Darin Detwiler characterizing the nondisclosure as “a prioritization of regulatory discretion over public transparency.”[3] That is a hard sentence to dismiss if the question is not simply whether the contaminated food was found, but whether the people downstream had enough information while the event was still actionable.
For public health surveillance, a 15-state spread has a specific operational meaning. No single hospital laboratory sees the whole pattern. A local lab may see one severe result, a state lab may receive a handful of isolates, and a federal system may be the first place where a multistate signal becomes visible. If disclosure is limited, the signal can still exist technically while remaining weak in practice for clinicians, local epidemiologists, and patients trying to connect illness with exposure.
That is why this belongs in a clinical applications discussion rather than only in a produce-recall archive. The durable question is not whether lettuce can be recalled. It is whether better detection at the bench becomes usable outbreak intelligence before the consequence has already landed in emergency departments.
The 25-State Salad Kit Recall Was Different
The Honey Balsamic Salad Kit recall affected more states, but it was a different kind of event. FDA listed the recall on Aug. 26, 2025, for Taylor Farms salad kits containing undeclared sesame and soy allergens, distributed in Alabama, Arizona, California, Colorado, Delaware, Florida, Georgia, Indiana, Kansas, Kentucky, Louisiana, Michigan, Missouri, Mississippi, New Jersey, New York, Ohio, Oregon, Pennsylvania, Tennessee, Texas, Utah, Virginia, Washington, and West Virginia.[2]
That recall matters to affected consumers and to clinicians evaluating allergic reactions, but it does not carry the same surveillance lesson as a multistate E. coli outbreak. The problem is label accuracy and exposure avoidance, not pathogen detection across stool specimens and isolate networks. It answers part of the affected-states query cleanly; it should not be used as evidence about infectious disease surveillance performance.
Where AI Actually Helps in the Laboratory Chain
AI is most credible in this space when it is attached to a specific laboratory task. A convolutional neural network does not “detect an outbreak” by itself. It can scan an image, prioritize fields of view, flag likely organisms, or reduce the number of negative slides a technologist must review manually. That is not glamorous language, but it is exactly where a clinical microbiology lab feels the difference during a surge.
ARUP Laboratories’ Cyclospora work is a useful example because the task is concrete: stool slide review for a parasite that can become painfully labor-intensive during seasonal outbreaks. GovInfoSecurity reported that ARUP’s convolutional neural network system reduced Cyclospora stool slide review to about 2 minutes per slide, helped absorb an approximately 200% testing-volume surge, and supported detection of about 50 positive cases per day during outbreaks, citing Ryan Jensen of ARUP.[4] Those are operational claims from named-source reporting, not a substitute for a peer-reviewed performance paper, but they describe the kind of bottleneck a lab director recognizes immediately.
The University of Tennessee work points in a similar direction. Produce Processing reported a machine learning system for Cyclospora oocyst identification with 95% confidence and high-throughput, 24/7 operation, citing Scott Lenaghan.[5] Again, that does not prove performance in every clinical environment. It does show the category of work AI can take on: repetitive visual identification, continuous screening, and triage of images or specimens that would otherwise wait for scarce expert review.
| AI use case | What is automated or prioritized | What the reported evidence supports | What it does not prove |
|---|---|---|---|
| ARUP convolutional neural network for Cyclospora slides | Microscopy image review and candidate detection | Faster slide review, surge handling, and daily positive-case throughput as reported by named-source journalism | That all outbreak reporting becomes complete or that every lab can reproduce the workflow unchanged |
| University of Tennessee machine learning for oocysts | High-throughput image-based identification | Reported 95% confidence and 24/7 operation in the described project | Clinical effectiveness across jurisdictions or replacement of confirmatory public health processes |
| FDA AI inspection targeting | Prioritization of inspection resources | Agency interest in using AI to focus oversight activity | Prevention of a specific Taylor Farms event or full transparency after an outbreak |
The food safety agency side is further upstream. Civil Eats reported that FDA Commissioner Marty Makary discussed AI for inspection targeting in May 2025 testimony, and that FDA launched an agency-wide generative AI platform called Elsa in June 2025.[6] Inspection targeting is a different application from diagnostic microscopy. It is not looking at stool slides or producing a clinical result. It is a prioritization tool for oversight, and its value depends on what data feed it, what decisions it influences, and whether those decisions are auditable.
Detection Speed Is Not the Same as Surveillance Completeness
A faster laboratory result changes the first half of the chain. It can reduce slide backlog, flag a likely organism sooner, and help staff keep up when specimen volume rises. It does not, by itself, decide which conditions are reportable, whether all jurisdictions send comparable data, whether food exposure interviews are completed, whether a grower is named, or whether a public notice is issued.
The Cyclospora reporting issue makes that boundary plain. GovInfoSecurity reported that CDC made Cyclospora reporting optional under FoodNet in July 2025, a policy change that can fragment outbreak data just as laboratories are becoming more capable of finding the organism efficiently.[4] This is the kind of mismatch that makes bench-level innovation feel oddly stranded: the microscope workflow improves, but the surveillance denominator can become less complete.
The Taylor Farms E. coli event shows a second boundary: disclosure. If severe multistate illness data exist but no official outbreak notice is published, the problem is not a missing neural network. It is the decision architecture around public communication. AI can shorten the path from specimen to suspected signal; it cannot force a regulator to name a grower or publish an outbreak page.

What the Taylor Farms States Reveal About the AI Question
The affected-state list is more than a geography answer. In the E. coli event, the 15-state distribution suggests a signal that had to be assembled across jurisdictions, specimen sources, and reporting channels.[1] In the salad kit recall, the 25-state distribution reflects a product-distribution problem visible through recall mechanics.[2] Those are not interchangeable datasets, and they should not be interpreted as if they measure the same risk.
For clinical AI, the lesson is narrower and more useful than the usual promise language. AI-assisted diagnostics can help a laboratory see more, faster. It can make tedious microscopy less dependent on uninterrupted expert attention. It can support surge capacity when case volume rises. It can help inspection programs decide where to look first. But outbreak intelligence still depends on the unglamorous parts of the system: who collects the specimen, who confirms the result, who reports it, which network receives it, which fields are mandatory, and what the public is allowed to know.
That is also why the 2026 Cyclospora iceberg lettuce outbreak should not be folded back into the 2025 Taylor Farms answer. The timelines, hazards, and evidence base are different. The 2025 question can be answered with the E. coli romaine states and the Honey Balsamic Salad Kit recall states. The AI discussion belongs beside those events only insofar as it explains the clinical and public health workflow that determines whether future multistate signals become visible quickly enough to matter.
For laboratorians and public health teams, that is the practical stopping point. Better algorithms can reduce detection friction inside the lab. They cannot repair optional reporting, fragmented participation, nondisclosure of growers, or the absence of an official public outbreak notice. The surveillance gain appears only when the algorithm’s output has a reliable path into reporting, reconciliation, and transparent public action.
References
- Taylor Farms Named as Romaine Grower Behind Deadly Outbreak of E. coli Infections. Food Safety News. April 2025.
- Company Voluntarily Recalls Honey Balsamic Salad Kit…. U.S. Food and Drug Administration. Aug. 26, 2025.
- Why the FDA Didn't Announce the Romaine E. coli Outbreak. Northeastern University. April 2025.
- AI Takes On the Cyclospora Outbreak. GovInfoSecurity.
- AI Used to Speed Up Detection of Cyclospora in CPS Project. Produce Processing.
- FDA Expanding Use of AI in Food Safety Inspection. Civil Eats. May 2025.
Comments
Join the discussion with an anonymous comment.