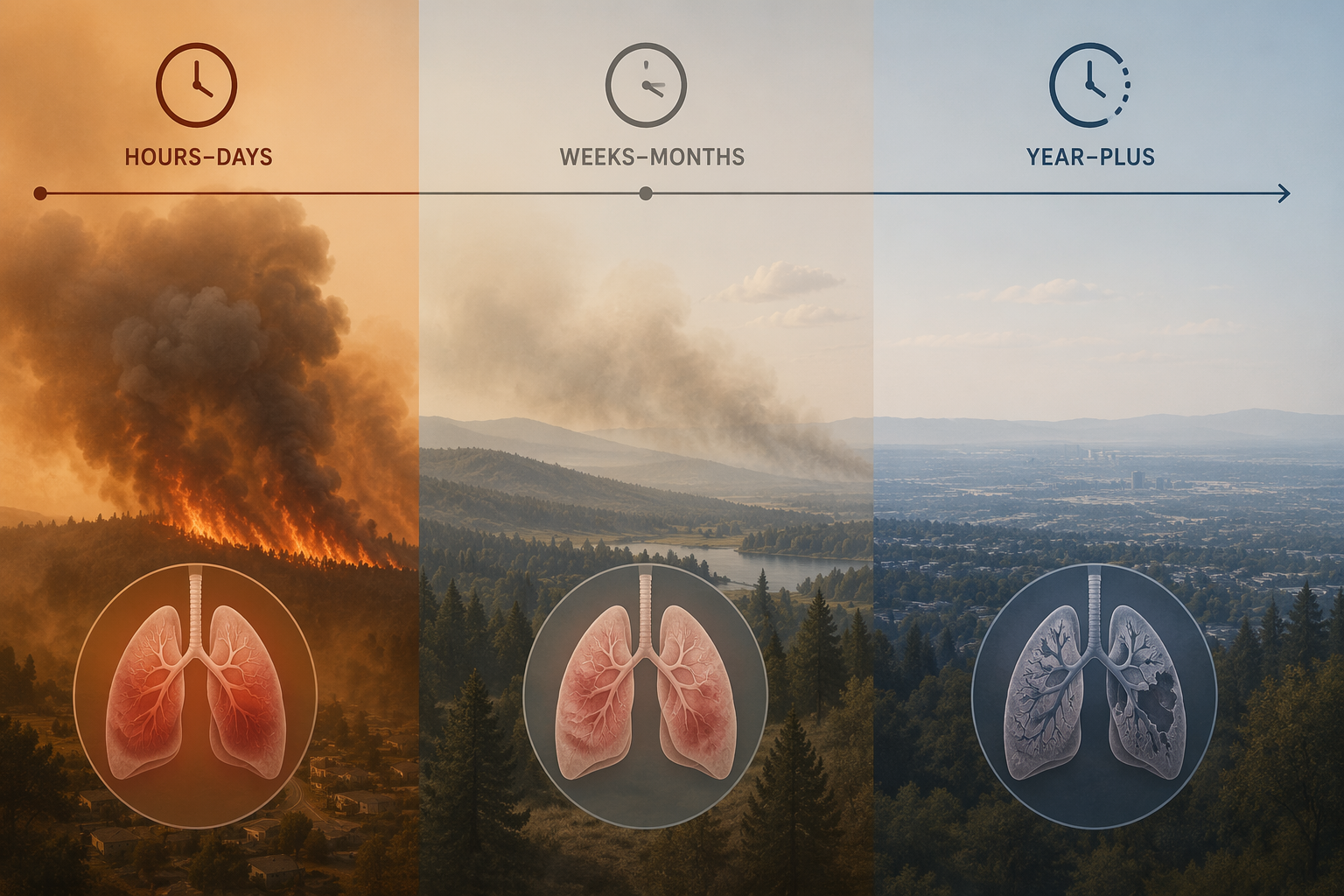
The clinical question is not simply whether wildfire smoke harms the respiratory system. It is how long the exposure lasts, which outcome is being counted, and when that outcome becomes visible. Hours to days point toward asthma visits, asthma admissions, COPD exacerbation risk, and mortality during smoke events. Weeks to three months raise a different problem: cardiorespiratory hospitalization risk after the sky has cleared. A 12-month moving average belongs to population mortality attribution, not to a bedside claim about one smoky week.
| Exposure window | Clinical signal most supported by the evidence | Interpretive caution |
|---|---|---|
| Hours to days | Asthma emergency department visits and admissions; COPD and asthma mortality signals during smoke events | Relative risks are modest for asthma utilization but can be operationally important when exposure is widespread |
| Weeks to three months | Persistent hospitalization risk for ischemic heart disease, hypertension, COPD, and asthma after smoke exposure | The strongest evidence comes from one large US study and needs replication |
| 12-month moving average | Nonaccidental mortality attributable to wildfire PM2.5 at the population level | This is not the same as lifetime or multi-decade cumulative exposure |
That distinction matters because wildfire smoke duration can otherwise flatten several different clinical phenomena into one exposure label. A patient with asthma who presents two days into a smoke episode, a patient with COPD hospitalized weeks later, and a mortality model using a year-long exposure construct are not asking the same evidence to do the same job.
Acute smoke exposure: small relative risks, real clinical volume
The short-term respiratory evidence is the most intuitive because it aligns with what emergency departments and urgent-care clinics see during visible smoke: more wheeze, more rescue medication use, more exacerbations, and more patients whose baseline disease leaves little reserve. In a comprehensive review summarizing wildfire smoke health evidence, asthma emergency department visits increased with a relative risk of 1.07 per wildfire smoke event, and asthma admissions increased with a relative risk of 1.06. COPD mortality was also elevated, with an odds ratio of 1.14 during smoke exposure windows.[1]
Those asthma estimates should not be inflated into a dramatic individual prediction. A relative risk of 1.07 does not mean most exposed patients will require emergency care. It means that, across exposed populations, the rate of asthma emergency department visits rose modestly compared with the reference condition. In a large metro area under smoke for several days, that modest increase can still be enough to change staffing pressure, inhaler demand, triage waiting times, and admission bottlenecks.
The COPD mortality signal deserves a different reading. Mortality during smoke exposure is not just another utilization endpoint. COPD patients often have fixed airflow limitation, cardiovascular comorbidity, and less physiologic margin during hypoxemic or inflammatory stress. An odds ratio of 1.14 is not a bedside rule for an individual patient, but it is clinically relevant because the outcome is severe and concentrated among people already vulnerable to decompensation.[1]
Asthma mortality also appears in the smoke-event literature as a more severe, less common endpoint. The same review reports that asthma mortality increased more than threefold during smoke events.[1] That finding should be interpreted with the caution appropriate to event-based observational data, but it prevents a common mistake: treating wildfire smoke as a nuisance exposure that only increases mild symptoms.
What the acute window can and cannot answer
The acute window is best suited to questions about exacerbation timing. It supports planning for asthma and COPD surges during and immediately after smoke events. It does not, by itself, answer whether risk has returned to baseline once the air looks clear, and it does not explain annual mortality burden. When those questions are folded back into the acute evidence, clinical interpretation becomes imprecise.
This is also where exposure definition becomes more than a methods detail. “Smoke event,” “wildfire PM2.5,” daily concentration, cumulative multi-day exposure, and modeled plume exposure are not interchangeable. A respiratory admission study and a mortality attribution study may both use wildfire smoke language while measuring different exposure windows and outcomes.
The important after-period: hospitalization risk can persist after visible smoke clears
The more clinically disruptive finding is not that smoke causes symptoms while smoke is visible. It is that elevated cardiorespiratory risk may continue into the weeks and months after a fire. Wei et al. 2025 examined 21.7 million hospitalizations across 15 US states from 2006 through 2020 and reported elevated risks for ischemic heart disease, hypertension, COPD, and asthma that persisted for weeks to three months after smoke exposure.[2]

The scale of that study is why it changes the practical frame. A 15-state hospitalization base over a 2006–2020 window is large enough to make the after-period hard to dismiss as anecdote. The finding also crosses respiratory and cardiovascular categories: COPD and asthma remain directly relevant to pulmonary care, while ischemic heart disease and hypertension matter because many respiratory patients carry cardiovascular risk that can complicate smoke-related decompensation.[2]
Hypertension reportedly showed the greatest increase among the evaluated outcomes.[2] That does not make wildfire smoke primarily a hypertension story, but it does argue against a narrow airway-only interpretation. Fine particulate exposure can plausibly create overlapping cardiopulmonary stress, and hospitalization categories capture the organ system that finally crosses a clinical threshold, not necessarily the only system affected.
For clinicians and public health officials, the weeks-to-months window changes the monitoring problem. The patient who worsens after the orange sky has disappeared may still be inside a biologically and epidemiologically relevant risk period. The public-health official who stands down all respiratory surveillance once the plume maps improve may miss delayed demand in COPD and asthma hospitalizations.
The limitation is equally important. The three-month persistence signal comes from a landmark observational study, not from multiple replicated trials across every geography and fuel type. That is not a defect unique to wildfire smoke research; randomized exposure is not an option here. But it means the finding should be used as a reason to keep post-fire risk visible, not as a precise universal countdown clock.
Year-long exposure constructs answer a different question
Long-term wildfire smoke evidence shifts from near-term clinical utilization to population mortality. A 2025 study reported that long-term exposure to wildfire PM2.5 was associated with approximately 11,415 nonaccidental deaths annually in the contiguous United States, with adults aged 65 years and older showing the highest mortality rate increases.[3]
The key phrase is “long-term exposure,” but the key method is more specific: the study used a 12-month moving average. That is a meaningful exposure construct, especially for annual mortality attribution, but it should not be paraphrased as lifetime cumulative smoke exposure or decades-long personal exposure history. The clinical interpretation is narrower and stronger when the exposure window remains visible.
The cause-of-death distribution also complicates a respiratory-only reading. The study attributed 72.5% of excess deaths to cardiovascular, mental, endocrine, and digestive diseases.[3] Respiratory harm remains central to patient-facing smoke episodes, but the mortality burden captured by a 12-month moving average extends well beyond asthma and COPD.
That difference should affect how the evidence is used. Acute relative risks help anticipate respiratory care demand during smoke events. Medium-term hospitalization data support continued vigilance after smoke clears. A year-long mortality model helps estimate public-health burden. These are complementary, not interchangeable.
Wildfire PM2.5 should not be treated as ordinary PM2.5 with a source label
One reason duration matters is that wildfire smoke is not only a matter of particle mass. Aguilera et al. 2021 found that wildfire-specific PM2.5 was more harmful per unit than non-wildfire PM2.5 for respiratory hospitalizations, with increases of 1.3% to 10% per 10 μg/m³ for wildfire PM2.5 compared with 0.67% to 1.3% per 10 μg/m³ for non-wildfire PM2.5.[4]
That dose-response difference supports a practical distinction: clinicians and analysts should be cautious about importing general ambient PM2.5 assumptions into wildfire events without considering source-specific toxicity. The point is not that every wildfire plume has identical composition. It is that wildfire-generated particles may carry different risk per unit concentration than background or non-wildfire particles.
A multi-country analysis by Zhang et al. 2025 extended that concern across 1,052 communities in eight countries, reporting that wildfire-specific PM2.5 posed greater hospitalization risks for asthma, COPD, pneumonia, and influenza than non-wildfire PM2.5.[5] That finding is useful because it moves the source-specific signal beyond one local context, although hospitalization risk remains an outcome-specific measure rather than proof of every possible long-term effect.
Boundary findings: cancer, lung function, fuel type, and thin duration guidance
Several longer-horizon findings are worth noting without letting them take over the clinical center of the article. The wildfire smoke review reports a lung cancer hazard ratio of 1.049 among people within 50 km of wildfires over 10 years.[1] That estimate is directionally important but small, and it belongs to a chronic-risk discussion rather than an acute exacerbation frame.
The same review cites follow-up after the 1997 Indonesian fires showing decreased lung function 10 years after exposure.[1] Because this is available here as secondary reporting, it is best treated as a signal that severe smoke episodes may have durable respiratory consequences, not as a fully characterized estimate for contemporary US clinical practice.
Fuel type adds another boundary. Grassland, boreal forest, structural, and mixed-fuel fires can produce different chemical profiles, and toxicity may vary accordingly. The current clinical literature does not yet allow every duration estimate to be cleanly stratified by fuel source, which is one reason broad statements about “wildfire smoke exposure” can overrun the evidence.
Formal duration guidance is also thinner than the clinical need. The operational framework in this article comes mainly from peer-reviewed epidemiology and hospitalization studies, not from a mature consensus guideline that tells clinicians exactly how long to monitor every exposed patient after every fire.
A clinically useful reading of duration
Duration is not a background descriptor. It determines which harm is plausible, which endpoint should be watched, and how cautiously the evidence should be interpreted. Hours to days explain near-term asthma and COPD exacerbation pressure. Weeks to three months keep post-fire COPD, asthma, and cardiovascular hospitalization risk on the board after visible smoke has cleared. A 12-month moving average supports population mortality attribution, but it should not be stretched into a claim about lifetime cumulative exposure.
That calibrated reading is less dramatic than saying wildfire smoke is simply dangerous, but it is more useful. The respiratory system does not experience smoke duration as a single exposure category. Emergency departments, inpatient services, chronic disease programs, and mortality studies each see a different part of the same exposure timeline.
References
- Wildfire smoke and respiratory health: a comprehensive review, PMC.
- Cardiorespiratory effects of wildfire smoke particles can persist for months even after a fire has ended, Harvard T.H. Chan School of Public Health.
- Long-term exposure to wildfire smoke associated with higher risk of death, Yale School of Public Health.
- Fine particles in wildfire smoke and pediatric respiratory health in California, Nature Communications, 2021.
- Wildfire-specific fine particulate matter and hospital admissions in 1,052 communities across eight countries, Nature Sustainability, 2025.
Comments
Join the discussion with an anonymous comment.