The clinical problem with wildfire smoke is not only that the air gets worse. It is that the patients most likely to decompensate are often identifiable before the emergency department fills, while the system still behaves as if risk appears only when someone arrives wheezing at triage. In a Stanford analysis of extreme smoke days, emergency visits for asthma, COPD, and cough rose by 30% to 110% after those events, even as total ED visits fell by 6% to 9%, likely reflecting broader behavioral avoidance during smoke episodes.[1]
That mismatch matters. A drop in overall ED traffic can make a smoke event look deceptively quiet from the hospital operations view, while respiratory risk is concentrating in a smaller, clinically vulnerable group. For a pulmonary clinic, a primary care panel, or a population-health team, the useful question is not whether air quality is poor in the abstract. It is which patients should be called today, which medication plans need review, which zip codes warrant outreach, and which households may need help reducing indoor exposure before symptoms cross the threshold into urgent care.

From smoke signal to patient list
UC Davis Health’s Wildfire Population Health Approach is useful because it treats wildfire smoke risk as a workflow problem, not just a prediction problem. Its five-pillar model integrates real-time AirNow AQI data into the electronic health record, flags patients in high-risk zip codes, applies natural language processing-derived machine learning models to estimate COPD and asthma hospitalization risk, and layers social vulnerability measures including the Healthy Places Index and Area Deprivation Index into wildfire-risk-tiered care pathways.[2]
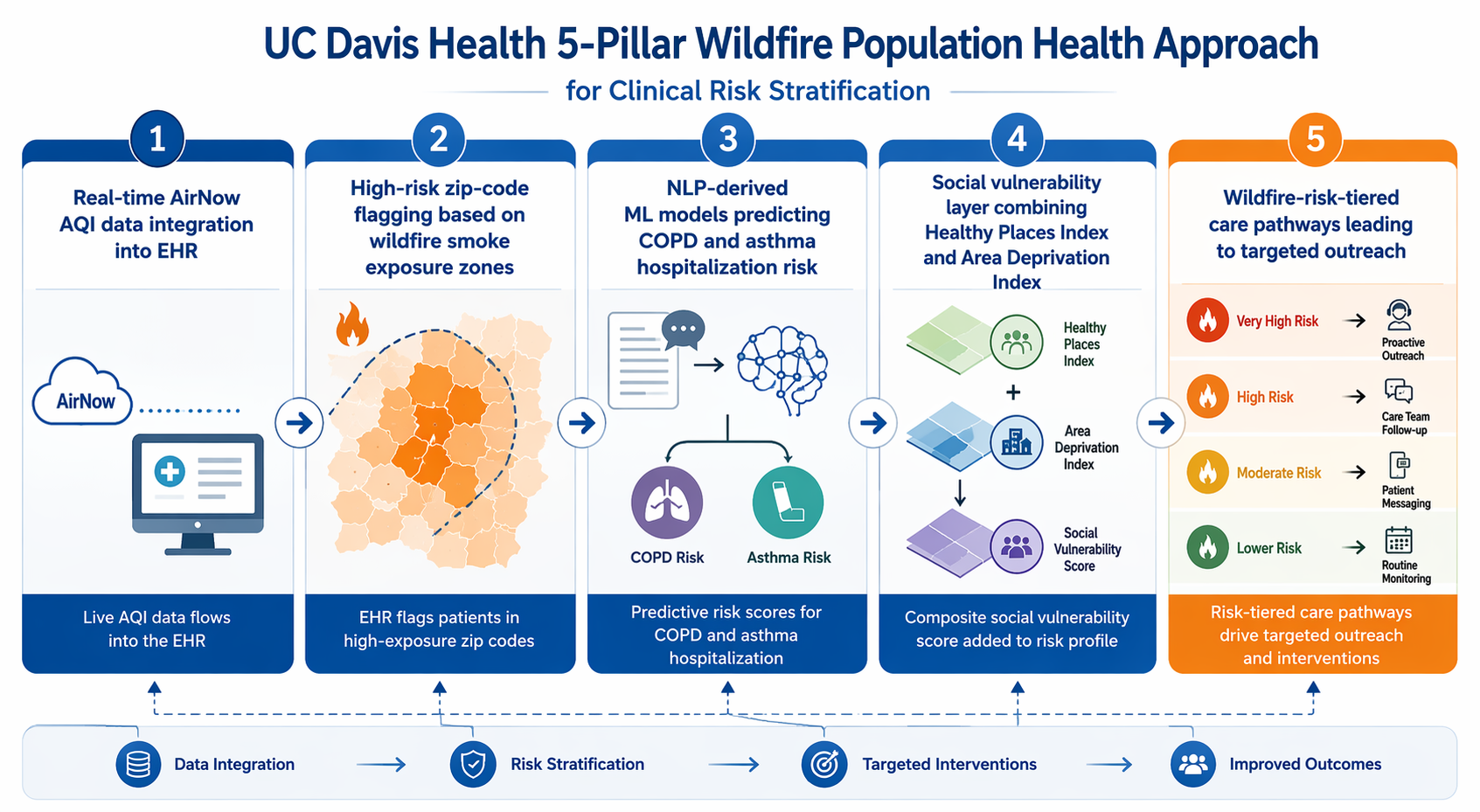
The important move is the linkage. Real-time AQI alone can warn a community. An asthma or COPD registry alone can identify chronic respiratory disease. A social vulnerability index alone can show where exposure mitigation may be harder. None of those sources, by itself, tells a care team which patient should receive outreach when smoke moves over a specific service area. The UC Davis approach brings those layers into the same clinical environment where staff already review panels, document outreach, and route patients into care pathways.[2]
That distinction is central to the health risks of poor air quality from wildfire smoke. A static high-risk list can be stale by the time wind shifts. A population-level smoke map can miss the patient who has severe COPD, lives in a high-smoke zip code, lacks resources to improve indoor air filtration, and has a prior hospitalization pattern buried in narrative notes. Machine learning is most clinically relevant here when it shortens the distance between environmental exposure, EHR-known vulnerability, and a concrete action.
| Layer | Clinical function | Why it matters during smoke events |
|---|---|---|
| Real-time AirNow AQI in the EHR | Brings local exposure conditions into the clinical workspace | Reduces reliance on separate public dashboards or delayed manual checks |
| High-risk zip-code flagging | Identifies panels in areas with elevated smoke exposure | Helps teams prioritize outreach geographically when capacity is limited |
| NLP-derived ML risk models | Uses EHR data, including information extracted from clinical text, to estimate hospitalization risk for asthma and COPD | Moves beyond diagnosis labels alone when selecting patients for intervention |
| Healthy Places Index and Area Deprivation Index | Adds neighborhood-level social vulnerability | Recognizes that exposure avoidance and indoor air protection are not equally available |
| Wildfire-risk-tiered care pathways | Connects risk strata to outreach and care actions | Prevents the model from ending as a dashboard without a downstream response |
For health-system leaders, the care pathway is not a finishing detail. It is the difference between risk stratification and clinical noise. If a model flags 2,000 patients and no one has decided who calls them, what script they use, how medication access is checked, when a clinician reviews symptoms, or how social needs are escalated, the model has merely created a more sophisticated queue. If the pathway is tiered, a nurse may focus first on patients with severe obstructive disease in high-smoke zip codes, while lower-risk patients receive automated guidance or portal messages. The available evidence supports that kind of operational use; it does not yet support treating these tools as proven admission-reduction systems.
Why the risk signal deserves clinical attention
Wildfire smoke should not be handled as ordinary bad air with a dramatic sky. Stanford data indicate wildfire PM2.5 may be about 10 times more toxic than fossil-fuel PM2.5, a distinction that changes the clinical posture from generic air-quality advice to targeted protection for patients who may have little physiologic reserve.
Respiratory disease is the obvious entry point because asthma and COPD exacerbations are what clinics and EDs see quickly after smoke exposure. The Stanford ED findings support the practical need for earlier outreach: disease-specific visits rise even when total ED utilization declines.[1] Pediatric data add another reason not to treat smoke episodes as transient irritant events; a Yale School of Public Health study found that children exposed to wildfire smoke had reduced lung function persisting 2 to 4 years after exposure.[3]
The clinical frame cannot stop at wheeze. A PNAS mortality study estimated approximately 11,415 nonaccidental deaths per year attributable to long-term smoke PM2.5 exposure, with a 95% confidence interval of 6,754 to 16,075 deaths.[4] In that analysis, 72.5% of attributable deaths came from cardiovascular disease, mental disorders, endocrine diseases, and digestive diseases rather than respiratory disease alone.[4]
Cardiovascular evidence points in the same direction. A Circulation Research review reported a 42% increase in heart attack emergency room visits, a 22% increase in ischemic heart disease, and up to a 70% increase in out-of-hospital cardiac arrests associated with wildfire smoke exposure.[5] Those findings do not mean a pulmonary outreach model automatically solves cardiovascular risk. They do mean that health systems building smoke-response registries should be careful about making the denominator too narrow.
A practical smoke-risk model may begin with asthma and COPD because those are clinically actionable and well represented in respiratory workflows. But once a health system has connected AQI, geography, EHR history, and social vulnerability, the same infrastructure can support broader panel review for patients with cardiac disease, complex chronic illness, or limited ability to shelter from exposure. The model’s first use case should not become its clinical ceiling.
What AI can add, and what it cannot prove yet
The strongest argument for AI in this setting is heterogeneity. Smoke exposure changes by hour and location. Patient vulnerability varies by diagnosis, prior utilization, medication access, home environment, age, comorbidity, and social conditions. A clinician can recognize many of those risks one patient at a time; a population-health program needs a way to sort thousands of patients quickly enough for outreach to matter.
Respiratory AI literature suggests that related tools can detect or anticipate deterioration. A review of AI in respiratory care reported that wearable sensors with AI algorithms can detect wheezing and abnormal respiratory patterns with greater than 80% accuracy, and that machine learning models can predict severe COPD exacerbations up to 7 days in advance.[6] Those findings are relevant, but they are not equivalent to showing that a wildfire-smoke risk-stratification program reduces admissions across health systems.
That evidence distinction is where many AI discussions become too loose. A retrospective model that ranks risk well has answered one question: whether past data contain a signal. A pilot embedded in one institution has answered another: whether the tool can be made to function in a local workflow. A prospective, multi-center trial showing fewer admissions or ED visits after deployment would answer a harder question: whether the intervention improves outcomes when staff, patients, geography, data quality, and smoke patterns vary.
The current support for AI-driven wildfire smoke stratification is closer to the first two categories than the third. UC Davis provides a concrete implementation model, and respiratory AI studies show that machine learning can extract meaningful signals from clinical and sensor data.[2][6] But the available literature does not yet show multi-center prospective trials demonstrating that deploying these wildfire-specific tools reduces hospital admissions.
The equity problem sits inside the model, not beside it
Wildfire smoke risk is not distributed only by meteorology. Patients in underserved communities may face higher exposure and fewer practical options for reducing it: older housing, less access to filtration, jobs that cannot move indoors, transportation barriers, or limited ability to leave a smoke-affected area. The UC Davis model’s inclusion of Healthy Places Index and Area Deprivation Index is therefore not cosmetic. It is an attempt to make the risk tier reflect more than diagnosis codes and recent utilization.[2]
Still, adding social vulnerability measures does not eliminate bias. If sensors are sparse in underserved neighborhoods, exposure estimates may be less precise exactly where vulnerability is high. If an algorithm is trained on EHR data from patients who historically had better access to care, it may learn utilization patterns that understate risk among people who avoid or cannot reach clinics. If outreach success is measured only by portal response, the model may appear to perform best for patients already easiest to reach.
Equity monitoring has to be part of deployment, not a retrospective apology. Health systems piloting these tools should examine who is flagged, who is contacted, who accepts intervention, who deteriorates despite no alert, and whether false negatives cluster by language, insurance status, neighborhood, race, ethnicity, age, disability, or digital access. Internal discussions of algorithmic bias and health equity in clinical AI belong in the same meeting as model performance, staffing, and outreach design.
A cautious way to deploy
The reasonable near-term role for these systems is population-health decision support. A health system can use AQI-linked EHR tools to identify a priority panel before or during smoke events, assign risk tiers, trigger medication and symptom checks, route high-risk patients to clinical review, and connect socially vulnerable households with mitigation resources when those resources exist. That is already more clinically useful than asking every clinic to improvise from a public smoke map.
The deployment standard should be explicit: local validation before broad use, transparent thresholds, monitoring for missed high-risk patients, documentation of what action follows each risk tier, and outcomes tracking that separates model performance from intervention performance. If admissions fall after deployment, leaders still need to know whether the change came from better prediction, more timely outreach, lower smoke exposure, staffing differences, or secular variation across fire seasons.
Mortality estimates also need careful handling. One PNAS estimate attributed approximately 11,415 nonaccidental deaths per year to long-term smoke PM2.5 exposure, while more recent CBS News reporting cited around 24,100 deaths; those figures differ because of methodology and study period differences.[4][7] A clinical AI program does not need one perfect mortality number to justify pilot work, but it does need honesty about what each estimate measures.
The case for AI in wildfire smoke care is strongest when the technology is modest about its job. It can help turn a fast-moving environmental hazard into a prioritized patient list and a timed outreach workflow. It can help a nurse avoid calling alphabetically when the smoke plume has already chosen a geography. It can help a population-health manager reserve scarce intervention capacity for patients with both physiologic and social risk. What it cannot yet claim, based on the evidence summarized here, is proven multi-center reduction in admissions from wildfire-specific deployment.
That is enough to pilot carefully, and not enough to oversell. Health systems should treat AI wildfire smoke stratification as clinical-applications infrastructure under evaluation: useful for targeted outreach, deserving of operational investment, and accountable for validation, equity, and outcomes before it is promoted as a settled admission-prevention strategy.
References
- Wildfire smoke exposure and emergency department visits for respiratory conditions. PNAS, 2023.
- Wildfire Population Health Approach. UC Davis Health.
- Children exposed to wildfire smoke show reduced lung function persisting 2-4 years post-exposure. Yale School of Public Health.
- PNAS 2024 mortality study. PNAS, 2024.
- Circulation Research review. AHA journals.
- AI in respiratory care review.
- CBS News reporting on wildfire smoke mortality estimates. CBS News.
Comments
Join the discussion with an anonymous comment.