The clinical problem with wildfire smoke is that it can look deceptively simple from across a dashboard. A city turns orange, PM2.5 rises, an air-quality index changes color, and hospitals wait to see whether respiratory visits follow. But the impact of wildfire smoke on urban air quality and health is not just a cleaner version of the familiar pollution story. The same mass concentration of fine particles can carry different clinical implications depending on the source, chemistry, timing, neighborhood exposure, and who is still willing or able to come to the emergency department.

That distinction matters because wildfire smoke is becoming a recurring urban exposure, not a rare rural inconvenience that occasionally drifts into town. Emergency clinicians see the downstream version: wheezing patients who waited too long, older adults with cardiopulmonary disease whose baseline has shifted, families asking whether an inhaler is enough, and a waiting room that may be strangely calm precisely when risk is high. Public health teams see another version: monitors, modeled smoke plumes, syndromic feeds, delayed signals, and pressure to decide whether the absence of visits means absence of harm.
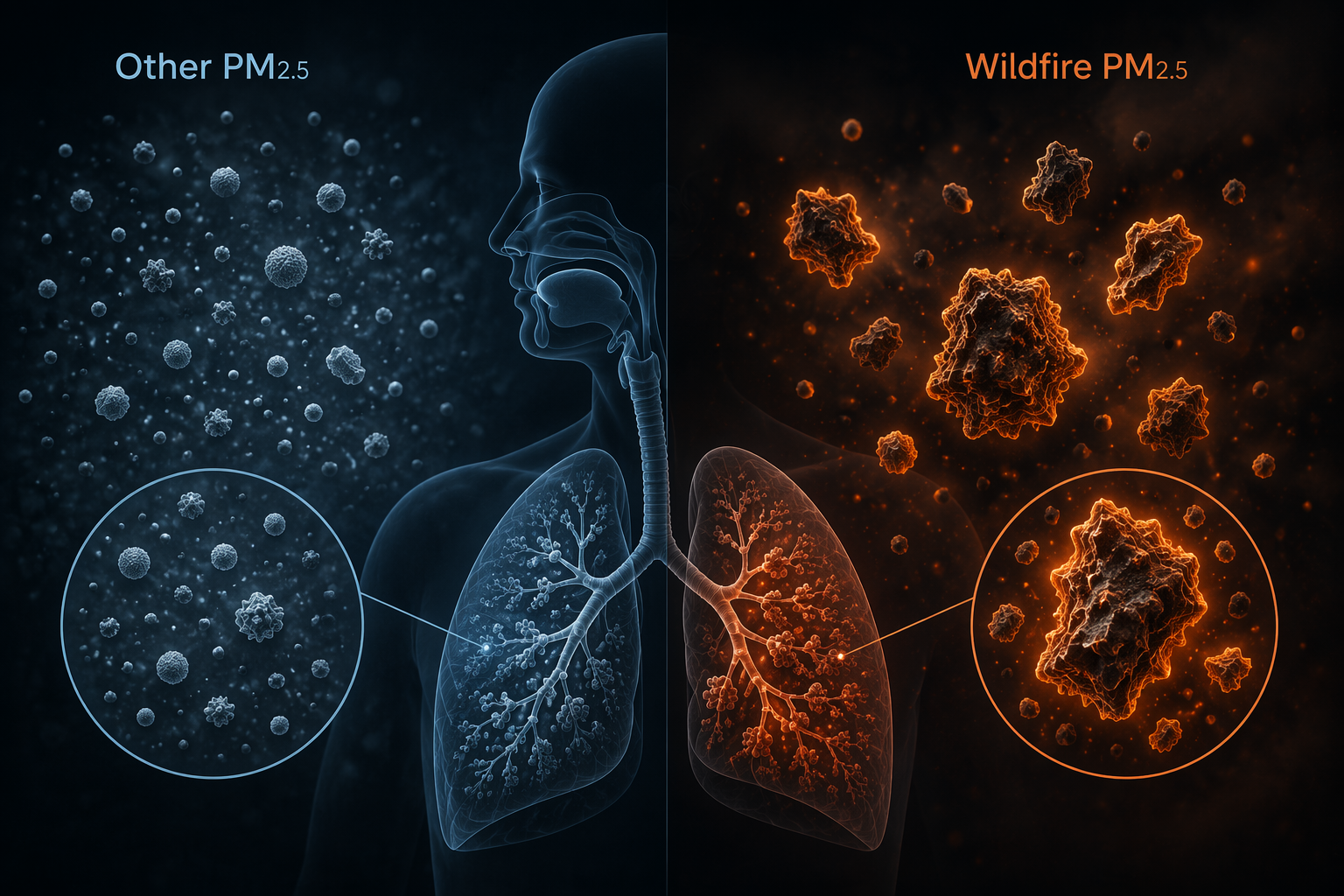
Wildfire PM2.5 Is Not Clinically Interchangeable With Other PM2.5
PM2.5 is useful because it gives clinicians and public health officials a shared unit for small airborne particles. It is also blunt. A microgram of wildfire-derived PM2.5 is not necessarily equivalent, biologically or clinically, to a microgram from traffic, industrial activity, or other combustion sources.
Aguilera and colleagues examined respiratory hospitalizations in Southern California during Santa Ana wind-driven wildfire conditions and found that wildfire-specific PM2.5 was associated with substantially greater respiratory harm per unit than PM2.5 from other sources. In the study’s comparison, wildfire PM2.5 was estimated to be up to 10 times more harmful for respiratory health than non-wildfire PM2.5, including fossil-fuel-related particles.[1]
The Southern California setting is important. Fuel type, burn conditions, topography, and meteorology vary by region, and Santa Ana-driven events are not every wildfire exposure. The finding should not be flattened into a universal constant. Still, it is clinically clarifying. When a hospital treats wildfire PM2.5 as just another high-PM2.5 day, it may be under-reading the risk attached to the source of the particles.
Mechanistically, the concern is not mysterious: wildfire smoke is a changing mixture of fine particles and gases produced by burning vegetation and, in many urban-interface fires, structures and synthetic materials. But for a health-system response, the operational point is narrower. If wildfire PM2.5 carries disproportionate respiratory toxicity, then exposure classification, neighborhood-level alerts, and clinical suspicion need to be more precise than a single citywide air-quality reading.
The Burden Extends Beyond a Spike in Wheezing
Asthma and COPD exacerbations are the most visible clinical signal during smoke episodes, and they deserve that attention. They are also not the whole burden. Long-term exposure analyses connect wildfire smoke PM2.5 to mortality, and broader reviews describe associations across respiratory, cardiovascular, endocrine, mental health, and cognitive outcomes.[2][3]
Ma and colleagues estimated that long-term exposure to wildland fire smoke PM2.5 was associated with approximately 11,415 attributable nonaccidental deaths annually in the contiguous United States.[2] That number should not be used as a theatrical endpoint; it is more useful as a seriousness marker. It says the harm is not confined to the day a smoke plume is visible outside the hospital entrance, and not confined to patients who present with acute bronchospasm.
For clinicians, the cardiovascular signal is especially easy to under-recognize. A patient with chest pain, arrhythmia symptoms, decompensated heart failure, or worsening exertional tolerance may not mention smoke unless asked. The exposure may be treated as background weather rather than as a contributor to physiologic stress. For administrators, the implication is different: respiratory visit counts alone will miss part of the strain, including patients who arrive through cardiology, primary care, urgent care, pharmacy demand, telephone triage, and delayed follow-up.
The broader evidence base is still uneven by outcome. Reviews describe smoke-related concerns that extend into endocrine, mental health, and cognitive domains, but those areas should not be treated as equally mature for bedside decision-making.[3] They do, however, make one conclusion hard to avoid: a smoke episode is not only an air-quality event. It is a population-health stressor with acute, delayed, and chronic dimensions.
Emergency Department Counts Can Go Quiet for the Wrong Reason
Hospital utilization is tempting because it is concrete. A patient arrives, a chief complaint is recorded, a diagnosis code appears, and the signal feels real. The problem is that utilization measures both illness and behavior. During severe smoke, people may stay indoors, avoid travel, postpone care, lose access to transportation, fear exposure outside the home, or decide that an emergency department is not worth the trip unless symptoms become intolerable.
Heft-Neal and colleagues put numbers on that distortion. In California, extreme wildfire smoke days were associated with a 30% to 110% increase in asthma and COPD emergency department visits, depending on the concentration range and subgroup examined. Yet total emergency department visits declined at the highest smoke concentrations.[4]
That combination is exactly the kind of pattern that can mislead a health system. Respiratory disease is worsening, but the total door count may fall. A manager looking only at aggregate ED volume could infer that demand is manageable. A syndromic analyst looking only at proportionate respiratory diagnoses could overestimate or underestimate burden depending on what is happening to the denominator. A clinician may see fewer low-acuity complaints and more concentrated respiratory acuity, which is not the same as less community harm.
| Signal | What it may appear to show | What it may actually mean during severe smoke |
|---|---|---|
| Total ED visits decrease | Overall acute care demand is lower | People may be avoiding care, postponing visits, or facing access barriers |
| Asthma and COPD visits increase | Smoke is affecting respiratory disease | The burden is visible in susceptible patients but may still be undercounted |
| Waiting room looks less crowded | The event is clinically mild | A quieter ED can coexist with higher risk among people who remain at home |
| Syndromic respiratory share rises | Respiratory disease is increasing | The numerator and denominator both need interpretation |
This is the point where a clean exposure-to-visit narrative breaks. Smoke exposure can increase clinical need while suppressing observed utilization. The consequence is not academic. Staffing, public messaging, outreach to high-risk patients, oxygen and bronchodilator supply planning, and follow-up capacity may all be calibrated to counts that are partly behavioral artifacts.
Why Urban Exposure Is Harder to See Than It Looks
Urban smoke exposure is patchy. Buildings, road corridors, wind shifts, indoor filtration, time spent outside, housing quality, and work conditions all change the dose that reaches a person’s lungs. A monitor several miles away can be directionally useful and still wrong for a neighborhood, clinic catchment area, school, shelter, or outdoor workforce.
That matters most for the groups a health system should be trying hardest not to miss: children with asthma, older adults, people with COPD or heart failure, pregnant patients, people without stable housing, outdoor workers, and residents in buildings without effective filtration. A regional PM2.5 average can make their exposure disappear into the mean.
This is also where artificial intelligence becomes relevant without needing to sound magical. The immediate value is not a bedside oracle. It is better exposure estimation, faster signal detection, and a more honest map of who may be affected before the ED count settles into a misleading pattern.
Where AI Enters the Response Chain
The strongest current use case for AI and machine learning is upstream of the bedside. Smoke response depends on knowing where exposure is occurring, whether clinical signals are rising above expected levels, and which patients may need earlier attention. Those are infrastructure problems before they are individual clinical decision-support problems.
| Response point | AI or ML role | Current practical value |
|---|---|---|
| Exposure prediction | Estimate daily smoke PM2.5 at finer spatial resolution | Helps identify neighborhoods and facilities that citywide monitors may miss |
| Syndromic surveillance | Detect unusual respiratory visit patterns in near real time | Supports public health alerts and situational awareness during smoke episodes |
| Clinical decision support | Integrate patient data, sensors, inhaler use, and lung-function tools | Promising, but wildfire-specific bedside guidance remains early |
Exposure prediction: making the invisible geography less invisible
Childs and colleagues developed a machine-learning model to estimate daily wildfire smoke PM2.5 exposure across the contiguous United States at a 10 by 10 kilometer resolution.[5] For urban health systems, that kind of resolution is not a cosmetic upgrade. It can shift attention from a citywide average to neighborhoods, clinics, school districts, and service areas where exposure may be materially different.
The model is most useful if its limits stay visible. Its predictive performance was weaker at smoke PM2.5 concentrations above 50 micrograms per cubic meter.[5] That is not a small footnote; those are the conditions when hospitals and public health agencies most need reliable estimates. A model that improves routine exposure assignment can still be less dependable during the extreme tail of the event.
Even with that limitation, high-resolution exposure modeling changes what can be asked. Instead of asking only whether the metropolitan area had bad smoke, analysts can ask which clinic panels, zip codes, or outreach lists overlapped with high estimated exposure. That can support earlier messages to patients with asthma or COPD, targeted pharmacy planning, and more realistic interpretation of utilization data after the event.
Syndromic surveillance: detecting respiratory strain while the event is still unfolding
Syndromic surveillance has a different job. It does not estimate exposure; it watches for clinical patterns that deviate from what would normally be expected. During the 2023 Canadian wildfire smoke episodes, CDC investigators using the National Syndromic Surveillance Program’s ESSENCE platform identified asthma-associated emergency department visits that were 17% above expected levels in affected areas.[6]
That example is modest in the best sense: it shows a practical public health use rather than a futuristic claim. Real-time or near-real-time detection can help health departments confirm that smoke is translating into respiratory morbidity, decide whether messaging is reaching the right populations, and alert healthcare partners before routine reports are complete.
The same utilization caveat still applies. Surveillance systems see care-seeking behavior as well as illness. If severe smoke suppresses some ED visits, then syndromic signals should be interpreted alongside exposure estimates, call center volume, pharmacy demand, outpatient contacts, school absenteeism where available, and qualitative reports from front-line services. AI can help detect a pattern, but it does not remove the need to ask why the pattern looks that way.
Clinical decision support: promising inputs, immature wildfire-specific guidance
The bedside AI story is less mature. Reviews of AI in respiratory care describe tools involving wearable sensors, smart inhalers, AI-supported spirometry, and other approaches that could eventually help identify worsening respiratory status earlier or personalize chronic respiratory management.[7] Those technologies are relevant to smoke response because wildfire exposure often worsens diseases that already require longitudinal monitoring.
But it would be premature to treat them as finished wildfire-specific clinical decision support. A smart inhaler signal may show rising rescue use; a wearable may capture changes in activity or physiology; spirometry tools may support remote assessment. None of that automatically tells a clinician how to triage a patient during a smoke event, when to escalate medication, or how to separate smoke-triggered deterioration from infection, heat stress, occupational exposure, or poor baseline control.
For now, the practical clinical use is more disciplined: use exposure and surveillance information to heighten suspicion, reach high-risk patients earlier, and interpret symptoms in context. The AI layer may improve the timing and targeting of those actions. It should not be asked to carry clinical judgment that has not yet been validated for wildfire-specific care.
What Health Systems Can Act On Now
The evidence is strong enough to justify treating wildfire smoke as a serious clinical and operational risk, even while important uncertainties remain. The uncertainties are not trivial: regional differences may limit direct transfer of toxicity estimates, same-day analyses may miss lagged effects, high-concentration exposure models may perform less well, and ED utilization can fall for reasons that conceal harm rather than reduce it.
A reasonable response does not require waiting for perfect models. It requires using current evidence in the places where it is most reliable. Wildfire-specific PM2.5 should be treated as clinically meaningful, not merely as another high-pollution day. Respiratory and cardiovascular services should expect effects beyond the most obvious asthma presentations. ED and urgent care counts should be read with caution during the highest smoke concentrations. Public health teams should combine exposure modeling with syndromic surveillance rather than relying on either one alone.
- Use smoke-specific exposure estimates where available instead of relying only on regional PM2.5 averages.
- Monitor asthma, COPD, cardiovascular complaints, pharmacy demand, call volume, and delayed presentations after visible smoke improves.
- Interpret falling total ED volume during severe smoke as ambiguous, not reassuring.
- Prioritize outreach to patients whose baseline disease or living conditions make avoidance advice hard to follow.
- Treat AI tools as support for exposure prediction and surveillance before treating them as bedside decision-makers.
That is the practical endpoint. Wildfire smoke is already a clinical and public health problem in urban settings, with evidence of disproportionate toxicity, respiratory and cardiovascular morbidity, mortality, and broader health consequences. AI is most credible today as an infrastructure layer that helps health systems see exposure and early clinical signals more clearly. The finished clinical answer still has to be built carefully, under the same conditions in which smoke care already happens: imperfect information, uneven access, and patients who may be harmed before they ever appear in the waiting room.
References
- Wildfire smoke impacts respiratory health more than fine particles from other sources: observational evidence from Southern California, Nature Communications, 2021.
- Long-term exposure to wildland fire smoke PM2.5 and mortality in the contiguous United States, PNAS, 2024.
- Wildfire Smoke and Health, Annual Review of Medicine, 2024.
- Associations between wildfire smoke exposure and emergency department visits in California, PNAS, 2023.
- Daily local-level estimates of ambient wildfire smoke PM2.5 for the contiguous US, Environmental Science & Technology, 2022.
- Notes from the Field: Asthma-Associated Emergency Department Visits During Wildfire Smoke Events — New York, June 2023, CDC MMWR, 2023.
- Artificial intelligence in respiratory care: Current evidence and future perspectives, Annals of Thoracic Medicine, 2024.
Comments
Join the discussion with an anonymous comment.