The weak point in many healthcare AI business cases is not the model demo. It is the line where production compute becomes a recurring operating expense and gets treated as if it were a stable cloud subscription. That assumption may survive a pilot. It does not survive clinical inference running across notes, images, messages, records, and bedside workflows every hour of the year.
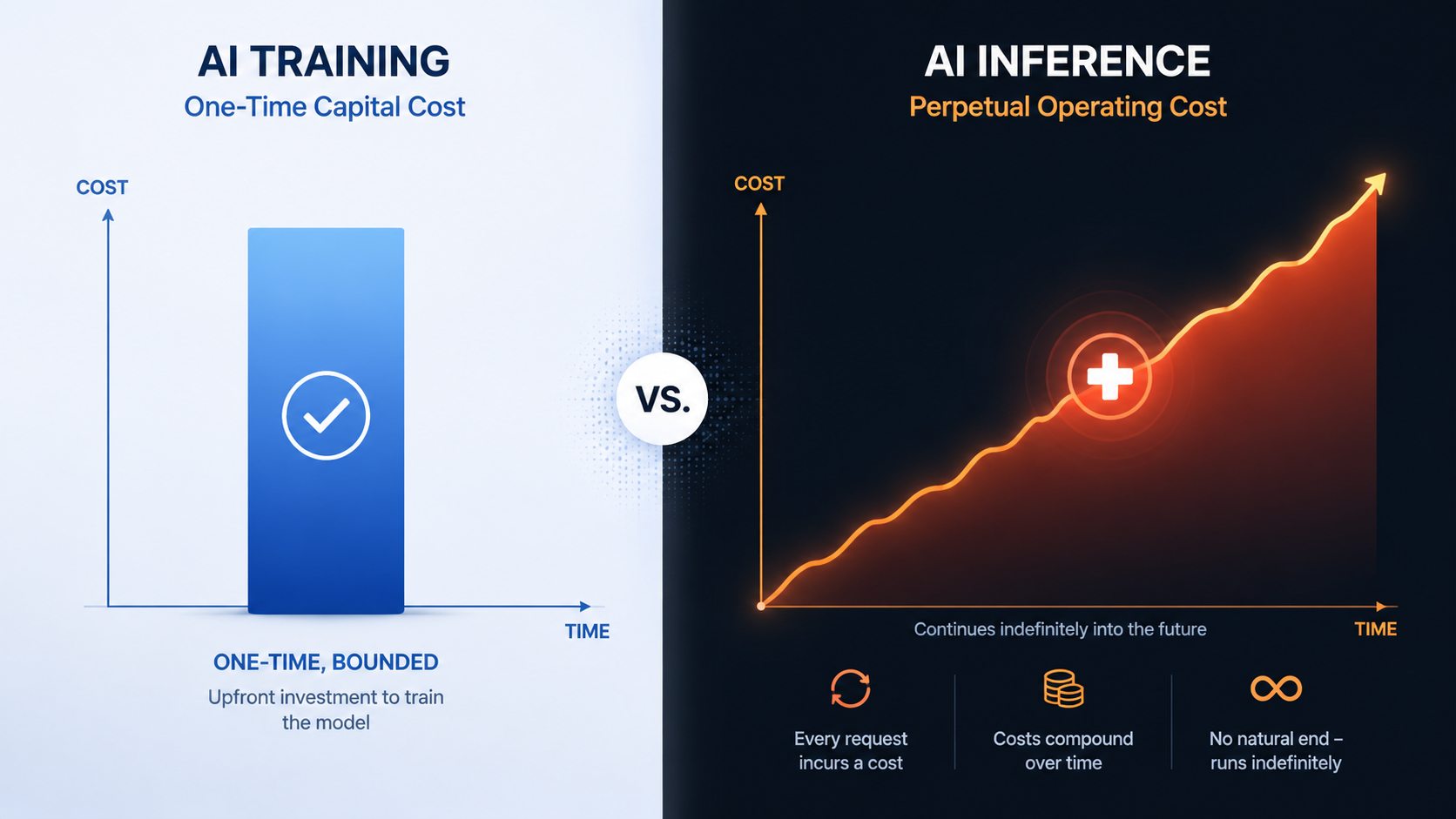
Training can be expensive, but it is at least bounded. A model is trained, tuned, evaluated, and either advanced or abandoned. Inference is different. Every time an ambient documentation tool drafts a note, an imaging model reviews a scan, a coding assistant reads a chart, or a triage tool scores a patient message, the system spends compute again. If the product works, usage expands. If usage expands, the electricity exposure expands with it.
That matters more in 2026 because the power line is no longer a quiet facilities concern. U.S. industrial electricity rates have risen 36% since 2020, and public fights over who pays for AI-related power demand have moved from utility planning rooms into ratepayer politics.[1] The International Energy Agency projected in April 2025 that global data center electricity consumption could double to about 945 TWh by 2030, with AI workloads accounting for nearly half of the increase.[2]
Inference Is Where The Bill Keeps Coming Back
A hospital can approve a training project as a capital-like event: data preparation, model development, validation, and deployment. The hard accounting starts when the model becomes part of care delivery. Clinical inference has no natural off switch. Patient messages arrive after hours. Emergency imaging does not wait for a favorable power price. Documentation tools follow clinicians through full shifts. Revenue cycle models run over large backlogs. The better the workflow fit, the more often the model is called.
This is why data center power costs should be modeled at the unit level, not buried inside a generic cloud assumption. The relevant question is not only whether a health system can access GPUs. It is whether the organization can afford the inference pattern that clinical adoption creates.
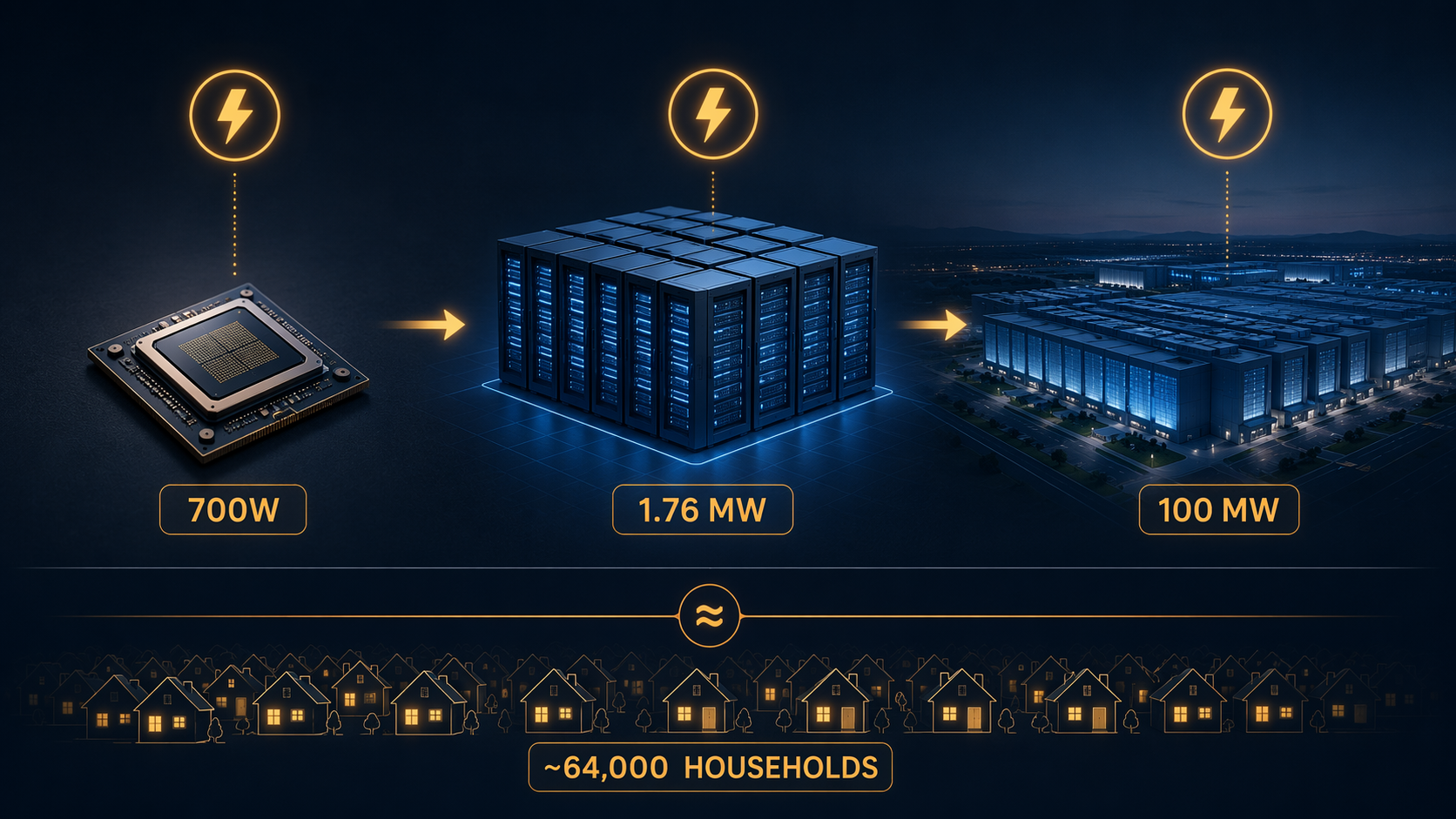
The power envelope makes the issue visible. A single NVIDIA H100 GPU draws 700W. A 1,000-GPU cluster can draw roughly 1.76 MW continuously. At hyperscale, a 100 MW data center may spend $41 million to more than $131 million annually on electricity alone, depending on local rates and utilization assumptions.[3][4] A facility at that size uses electricity on the order of 64,000 U.S. households.[3]
The household comparison is useful only because it restores scale to a discussion that often hides behind words like cloud, capacity, and managed service. It should not be mistaken for a healthcare-specific cost model. Hospitals are not necessarily building 100 MW AI campuses. Most are buying services from vendors, renting cloud capacity, expanding private data centers, or assembling hybrid infrastructure. But the electricity still exists somewhere in the cost base. If it is invisible on the hospital invoice, it is visible to the provider, the colocation operator, the cloud platform, the utility, or the ratepayer.
The Cloud Can Move The Line Item, Not Remove It
Cloud procurement has encouraged a convenient abstraction: the hospital pays for the application, the vendor pays for the infrastructure, and the data center becomes somebody else’s problem. That can be rational for early adoption. It is also how a recurring energy exposure gets converted into a flat-looking subscription fee until usage grows enough for the vendor to reprice, throttle, tier, or renegotiate.
This is not a complaint about cloud computing. Cloud platforms absorb complexity that most hospital IT teams do not want to own. They also pool demand, negotiate power, manage cooling, and operate at a scale individual health systems cannot match. But none of that changes the underlying economics of serving inference continuously. If a model requires high-cost compute for every encounter, the cost will surface somewhere: in per-seat fees, per-use charges, enterprise minimums, model limitations, service-level tradeoffs, or vendor margin pressure.
McKinsey has described power availability as a central issue in expanding data center capacity for AI, not a secondary facilities detail.[5] U.S. baseline reporting from Lawrence Berkeley National Laboratory also places data center energy use inside a broader national electricity planning problem, rather than treating it as an isolated technology-sector expense.[6] Healthcare buyers do not need to become utility analysts, but they do need to stop assuming that energy volatility is irrelevant because the word cloud appears in the contract.
Healthcare Workloads Make The Exposure Less Optional
Some industries can batch AI work, delay it, or run it where power is cheap. Healthcare has less freedom. A radiology model used in acute care must meet the workflow where the image is read. A clinical assistant used during an encounter must respond before the clinician gives up and types the note manually. A patient-facing triage tool cannot be treated as an overnight analytics job if it is part of front-door access.
The compliance layer tightens the constraint. HIPAA, GDPR, data residency commitments, institutional risk tolerance, and vendor governance all shape where inference can run. Healthcare-specific reporting in 2026 describes organizations reassessing cloud dependence and moving some AI inference closer to controlled infrastructure because of GPU and memory cost pressure, compliance expectations, and performance requirements.[7] Iceotope has similarly framed clinical-grade AI infrastructure around sovereign compute, latency, and cooling needs rather than pure cloud expansion.[8]
Those sources are useful for direction, not for precision. They do not provide granular power-cost-per-inference figures for health systems. The better conclusion is narrower: healthcare’s regulatory and workflow demands can push some AI workloads toward private, sovereign, on-premises, or hybrid infrastructure, where power and cooling become harder to ignore as operating expenses. They do not prove that every hospital should repatriate AI workloads, or that local infrastructure is automatically cheaper.
Data gravity adds another reason the decision is not simple. Imaging archives, genomics pipelines, longitudinal records, and operational data sets are expensive to move, slow to duplicate, and sensitive to govern. If the data already sits inside a hospital-controlled environment, shipping it outward for repeated inference may create latency, egress, security, and contracting concerns. If the model sits in the cloud, pulling the data toward it may be easier for deployment but more complicated for governance. Either way, inference location becomes a cost-design decision, not merely an architecture preference.
A Useful AI Tool Can Become A Bad Scaling Candidate
Healthcare procurement often asks whether an AI tool is accurate, safe, usable, and compliant. Those questions remain necessary. They are not sufficient. A tool can clear validation and still fail the operating model if each additional user, shift, patient, or record adds high-cost inference demand without a matching reduction elsewhere.
The distinction matters because AI value in hospitals is rarely captured at the same point where compute cost appears. An ambient documentation system may reduce clinician after-hours work, but the subscription may sit in an IT or departmental budget. An imaging model may improve worklist prioritization, but radiology leadership, enterprise IT, compliance, and the CFO may each see different pieces of the value chain. A coding tool may accelerate review, but the gain depends on staffing, denial rates, payer mix, and audit outcomes. The inference bill is more direct than the benefit calculation.
| Procurement Question | Why It Matters For Scaling |
|---|---|
| How often is inference called? | A model used once per admission behaves differently from a tool triggered across every note, message, image, or chart event. |
| What is the cost unit? | Per-token, per-study, per-encounter, per-user, and per-batch pricing create different exposure as adoption grows. |
| Where does inference run? | Cloud, colocation, on-premises, and sovereign infrastructure shift who sees the power bill and who controls latency. |
| What workload can be deferred? | Batchable analytics have more scheduling flexibility than point-of-care tools that must respond immediately. |
| What work actually disappears? | Electricity cost is easier to justify when the model removes measurable labor, rework, delay, or avoidable downstream expense. |
The uncomfortable category is the always-on model with modest per-use value and no clear displacement of work. These systems can look harmless during a pilot because utilization is low, champions are attentive, and vendor credits may soften the early bill. At enterprise scale, the same tool can become a compounding expense attached to routine clinical activity.
Grid Constraints Are Now Part Of AI Feasibility
Power cost is only one side of the constraint. Availability is the other. AI data center growth depends on substations, transmission, generation, interconnection queues, backup systems, cooling capacity, and local approval. Spheron describes grid connection timelines of 24 to 36 months in some AI infrastructure contexts, though those timelines vary significantly by region, utility, and project size.[3] For a hospital evaluating AI vendors, that variability matters because infrastructure scarcity eventually flows into pricing and service commitments.
The politics are also becoming less theoretical. CNBC has reported on ratepayer backlash over who pays for AI’s electricity demand.[1] Brookings has discussed AI energy growth in the context of grid safety margins and regulatory pressure.[9] EnerSys has pointed to Ireland’s Commission for Regulation of Utilities rules as an example of data center development being shaped by grid constraints and policy intervention.[10]
This does not mean a hospital AI roadmap should become an energy-policy document. It does mean local power conditions can influence which applications scale economically. A latency-sensitive model that must run near the point of care in a high-cost power region has a different path than an administrative summarization workload that can be batched through a cloud region with better economics. A vendor with reserved infrastructure in a constrained market has a different risk profile than one buying capacity opportunistically.
Efficiency Helps, But It Does Not Make Inference Free
There are real mitigation strategies. Model architecture, quantization, caching, batching, routing, accelerator choice, cooling design, workload placement, and power management can reduce electricity cost per useful output. These choices should be part of procurement and technical review. They should not be treated as a rescue plan that eliminates the need to model operating cost.
FP8 quantization is a good example. Spheron reports that FP8 on H100 hardware can deliver 30% to 40% more tokens per second at identical TDP compared with BF16, translating to a 23% to 29% reduction in electricity cost per token.[3] That is meaningful if the workload tolerates the numerical format and the full system is engineered to capture the gain. It is not a guarantee that the application’s total cost drops by the same percentage, because software overhead, memory, networking, idle capacity, vendor margin, and utilization patterns still matter.
GPU power-capping deserves similar treatment. MIT Sloan, citing MIT Lincoln Laboratory trials, reported that capping GPUs at 60% to 80% of thermal design power reduced energy consumption with negligible model quality loss.[11] That result supports a practical procurement question: will the vendor or infrastructure team tune for the lowest acceptable energy per useful inference, or simply run hardware at maximum performance because the power bill is abstracted away?
Efficiency gains are often presented as if they settle the issue. They do not. A 25% reduction in electricity cost per token can be overwhelmed if adoption triples, context windows expand, multimodal inputs become standard, or clinicians begin using the tool in more parts of the workflow. Better efficiency changes the slope. It does not remove the slope.
What A Serious Healthcare AI Business Case Should Show
The next generation of healthcare AI business cases should separate model development from production inference. They should also separate cloud subscription price from the cost drivers that shape that price. A flat annual software fee may be the commercial form of the contract, but it is not the economic behavior of the system underneath.
- Estimate inference frequency by workflow, not by licensed user count alone.
- Identify whether the model is called per token, per image, per encounter, per message, per record, or per batch.
- Ask vendors which parts of pricing are sensitive to GPU type, utilization, context length, latency tier, and region.
- Model local or contracted electricity exposure for on-premises, colocation, private cloud, and sovereign deployments.
- Require an efficiency plan that covers quantization, power management, model routing, caching, and workload scheduling where clinically acceptable.
- Tie scale-up approval to observed utilization and measurable work removed, not only to pilot satisfaction.
The finance question is not whether AI compute is expensive in the abstract. It is whether a specific clinical use case can carry its inference pattern at scale. A model that runs occasionally for high-value decisions may be easy to justify. A model that runs constantly for low-friction convenience may still be worth buying, but it deserves a much harder look at utilization, substitution, and marginal cost.
This is where CIOs, CFOs, informatics leaders, and infrastructure teams need to be in the same room before deployment, not after renewal. The CIO sees architecture and reliability. The CFO sees recurring commitments. Informatics sees whether the tool fits care delivery. Infrastructure sees latency, uptime, cooling, and capacity. If those perspectives meet only after enterprise adoption, the organization has already accepted the cost curve.
The Scaling Limit Is Operational
Healthcare AI will not be capped only by whether vendors can acquire GPUs or whether models continue to improve. The more durable constraint is operational: how much continuous inference a health system can afford, govern, power, cool, and justify against actual clinical or administrative work removed.
A roadmap that treats inference electricity as a hidden component of a flat cloud fee will underestimate that constraint. A roadmap that models it as an independent, compounding operating variable will make different choices: fewer vague enterprise deployments, more attention to workload shape, more pressure on vendors to disclose cost drivers, and a clearer distinction between impressive AI and AI that can run every day inside a hospital’s real operating budget.
References
- Who pays for AI's electricity?, CNBC, March 2026.
- Energy and AI, International Energy Agency, April 2025.
- Power-Bound, Not GPU-Bound, Spheron, 2026.
- Deconstructing the Data Center, Alpha Matica, 2026.
- AI power: Expanding data center capacity to meet growing demand, McKinsey, October 2024.
- 2024 United States Data Center Energy Usage Report, Lawrence Berkeley National Laboratory.
- Healthcare AI Leaders Are Rapidly Trying To Outmaneuver Skyrocketing Memory And GPU Costs, Forbes, June 2026.
- From Cloud AI to Clinical-Grade Infrastructure, Iceotope, April 2026.
- Global energy demands within the AI regulatory landscape, Brookings, April 2026.
- Data Centers in 2026: 5 Trends, EnerSys.
- AI has high data center energy costs — but there are solutions, MIT Sloan.
Comments
Join the discussion with an anonymous comment.