The controversy over AI-generated images in politics is no longer only a campaign-season communications problem. It has trained a public reflex that matters inside hospitals: when an image becomes inconvenient, confusing, or emotionally charged, someone can now ask whether it was made, altered, or mislabeled by AI. That question may be reasonable. It may also be opportunistic. Either way, it changes the room for the person who has to explain what the image means.
Political examples made the pattern visible first. PBS reported on White House-edited arrest photos and expert concerns that Trump’s use of AI images further erodes public trust; NPR documented AI images around hurricanes and disasters being used as propaganda during moments when the public was already trying to sort evidence from rumor.[1][2] For healthcare leaders, the important point is not the partisan content. It is the transferable habit: once people know images can be synthetic, real images become easier to challenge.
That habit has a name in misinformation research: the liar’s dividend. The phrase describes the advantage bad actors gain when authentic evidence can be dismissed as fake. In a clinical setting, the same mechanism does not need a conspiracy theory to become operationally expensive. It can appear as a patient doubting an image in a portal, a clinician questioning whether a teaching case is synthetic, a legal team asking for proof of origin, or a communications department deciding whether a label will clarify or make the public less confident.
The Label Can Become Part Of The Problem
A 2026 pre-registered experimental study by Harff in Computers in Human Behavior gives healthcare organizations a particularly awkward finding to absorb. In a German-speaking sample of 890 participants, average viewers struggled to identify AI-generated images without disclaimers. Labels helped with detection, but they also reduced message and source credibility, especially among people farther from the political center.[3]
That is not an argument against labeling. It is an argument against treating labeling as a magic solvent for distrust. A hospital that labels synthetic or AI-augmented medical images may be doing the ethically necessary thing and still paying a credibility tax. A label that says an image was AI-generated, AI-assisted, simulated, enhanced, or synthetic may answer one question while opening another: if this one needed a label, what else in the record might be less direct than it appears?

The study’s sample matters. It was German-speaking, not a U.S. patient population; its results should not be inflated into a universal behavioral law. But the operating problem is familiar enough to deserve attention. Healthcare transparency work often assumes that more disclosure produces more confidence. Harff’s finding complicates that assumption. In some image environments, disclosure can help people classify content while making them trust the communicator less.[3]
For medical imaging, that distinction is central. Detection and confidence are not the same outcome. A patient may correctly understand that a synthetic image was used for education or model development and still feel less certain about the surrounding institution. A clinician may appreciate that an AI label is honest and still wonder whether the image can be used for teaching, comparison, litigation support, or patient explanation. The label is not just metadata. It is a communication event.
Radiologists Were Fooled More Often Than Most Departments Would Expect
The clinical shock comes from a second 2026 study, reported by ScienceDaily from work published in Radiology. Tordjman and colleagues tested 17 radiologists from 12 institutions across 6 countries on GPT-4o-generated synthetic X-rays. When radiologists were unaware that synthetic images were present, they were fooled 59% of the time.[4]
That number should not be read as a population-wide estimate for all radiologists in all settings. The sample was moderate, and individual performance varied widely, from 58% to 92% detection. Still, the finding lands hard because it punctures a comfortable assumption in imaging operations: that expert visual training alone can reliably absorb a new class of synthetic media risk.[4]
Warning helped, but it did not solve the problem. When radiologists were told synthetic images might be present, average detection rose to 75%. That leaves a meaningful gap between awareness and reliable identification. The study also found no correlation between years of experience and detection ability, which is the part department leaders should not wave away. Experience remains essential for diagnosis, protocoling, supervision, and clinical judgment. It simply should not be assumed to confer automatic immunity to synthetic-image artifacts.[4]
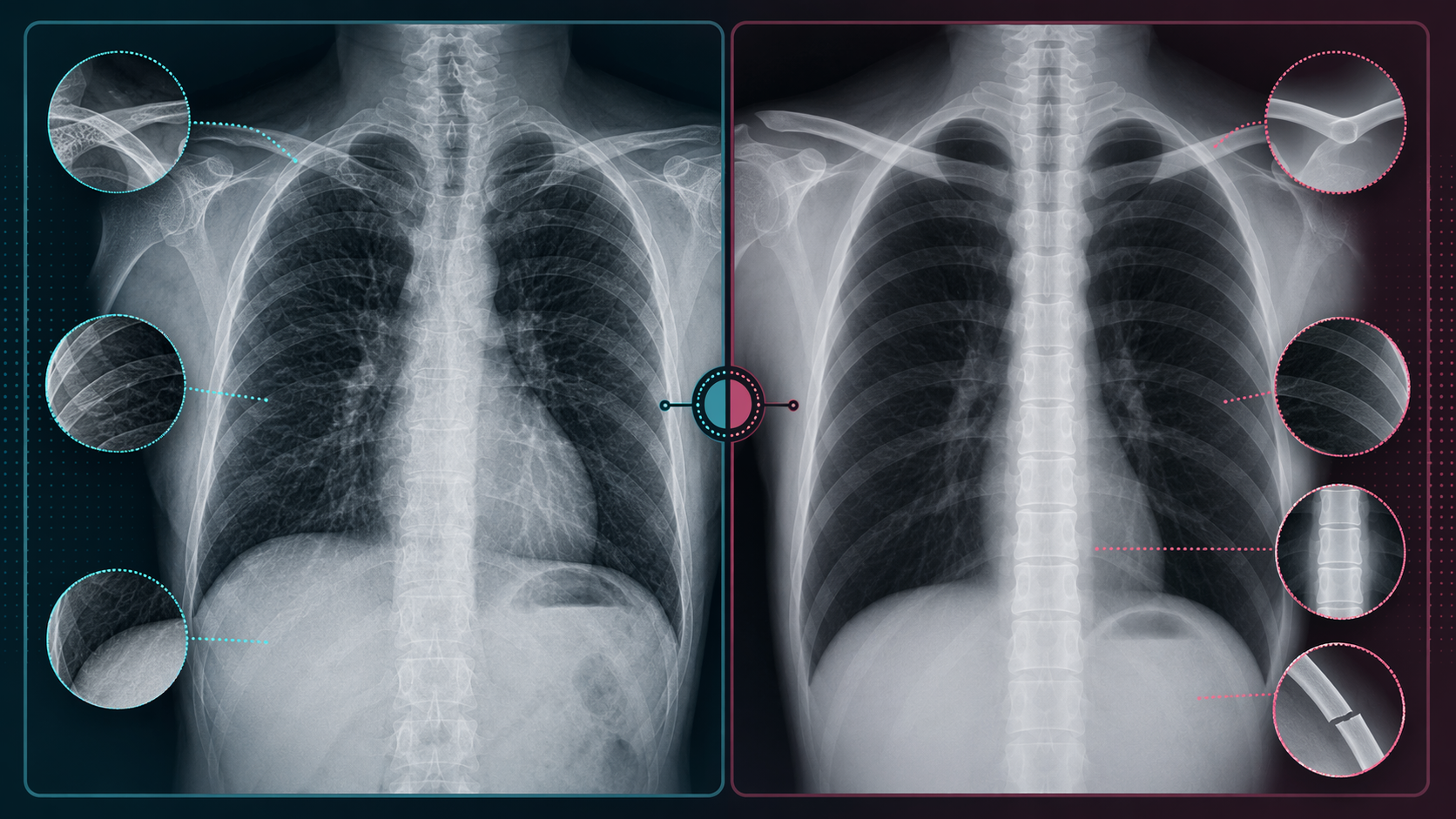
The visual clues are useful because they make the problem concrete without turning it into folklore. The synthetic X-rays in the study could show overly smooth bones, unnaturally straight spines, excessively symmetrical lungs, and unusually clean fractures.[4] These are not diagnostic rules for everyday use. They are examples of how a generative system may produce images that look coherent at the level of a quick read while failing at the level of anatomy’s ordinary messiness.
Tordjman and colleagues also warned that this may be “only the tip of the iceberg,” with 3D synthetic images such as CT and MRI as a logical next step.[4] That warning should be handled carefully. It is not evidence that synthetic CT or MRI deception is already common in clinical operations. It is evidence that the threat model should not stop at 2D radiographs, especially as image generation systems improve and as institutions begin using synthetic data for education, testing, augmentation, or research.
What Actually Transfers From Politics To Medicine
Political AI-image controversies and medical imaging do not carry the same stakes, workflows, or evidentiary standards. A campaign image circulates through social feeds; a radiology image moves through acquisition systems, PACS, reports, portals, consultations, quality review, and sometimes legal discovery. The transfer is not the content. The transfer is the trust dynamic.
| Trust Dynamic | Political Image Environment | Medical Imaging Implication |
|---|---|---|
| Detection uncertainty | Viewers struggle to tell generated and authentic images apart. | Patients and clinicians may not be able to rely on visual inspection alone. |
| Liar’s dividend | Real evidence can be dismissed as fake. | Authentic images may require stronger provenance support when contested. |
| Labeling penalty | Disclaimers can improve classification while reducing source credibility. | AI labels need explanation, not just placement in a portal or report. |
| Expert overconfidence | Public debate often assumes specialists can settle authenticity disputes. | Radiology experience did not correlate with synthetic X-ray detection in the reported study. |
The practical consequence is that healthcare organizations need to separate three questions that often get collapsed into one: Is the image clinically authentic? Has it been altered, generated, enhanced, or simulated? Can the institution explain that status in a way that preserves appropriate confidence? The answer to the third question will not automatically follow from the first two.
This is where patients differ from generic media consumers. A patient viewing an image in a portal is not usually trying to win an argument about misinformation. The patient may be trying to understand a diagnosis, prepare for a procedure, ask why a finding changed, or reconcile the image with symptoms. If an AI-related label appears without context, the patient may not know whether it refers to acquisition, reconstruction, triage, annotation, teaching material, report drafting, or a synthetic example used outside their own care. Ambiguity becomes part of the clinical experience.
Provenance Standards Help, But They Are Not A Waiting Strategy
The political and journalism worlds are beginning to build provenance infrastructure. PBS reported in January 2026 on C2PA-related efforts to make content origins more detectable, while also noting that the infrastructure misinformation researchers want is at least a year away even in political contexts.[5] Healthcare should pay attention to that timeline. If provenance systems are still maturing for public media, hospitals should not expect a finished external standard to arrive neatly packaged for PACS, enterprise imaging, clinical AI, research datasets, and patient portals.
That does not make provenance optional. It means health systems need an interim posture. The most durable work is likely to sit in ordinary governance rather than in public warnings: chain-of-custody records for images, audit trails for AI-assisted changes, clear separation between clinical images and synthetic teaching or validation images, vendor documentation requirements, and retention rules that make later review possible.
Procurement committees should be asking vendors narrower questions than “Do you use AI?” The better questions are operational: when an image is generated, modified, reconstructed, denoised, annotated, compressed, or enhanced, what metadata is created; where is it stored; can downstream systems preserve it; can a radiologist see it; can a patient-facing system translate it; and can the organization prove it later? A provenance feature that disappears at the next integration point is not provenance in practice.
Labeling Policies Need To Anticipate The Credibility Tax
Hospitals already use many forms of labels: preliminary report, amended report, AI-assisted triage, research use only, educational case, simulated image, reconstructed series, non-diagnostic image, patient-supplied outside study. AI-generated and AI-assisted images need to fit into that communication ecosystem rather than appearing as a special warning badge that makes everything nearby look suspect.
- Use labels that state the image’s role: clinical source image, AI-assisted reconstruction, synthetic teaching image, simulated example, or research dataset image.
- Avoid labels that imply more certainty than the organization has, such as “verified real,” unless the verification method is defined.
- Attach explanation where the patient or clinician encounters the image, not in a policy document several clicks away.
- Keep clinical and non-clinical image libraries visibly separated in systems used for teaching, demos, quality review, and patient communication.
- Prepare plain-language scripts for portal support teams and clinicians before the first disputed image creates urgency.
The goal is not to make patients skeptical of every image. It is to make the status of each image understandable enough that skepticism does not become the only available response. A label that says “AI-generated” without explaining whether the image is part of the patient’s care, education, or research can be technically transparent and practically confusing at the same time.
Radiology Training Should Treat Synthetic Detection As A Workflow Risk
The Tordjman findings argue for training, but not the kind that quietly tells radiologists to be more vigilant and leaves the rest of the system unchanged. If warned radiologists still averaged 75% detection, awareness alone is incomplete protection.[4] Departments should treat synthetic-image exposure as a workflow risk that touches education, quality assurance, AI validation, image sharing, and incident response.
A useful training program would not ask radiologists to memorize a list of artifacts as if the next generation of models will preserve the same flaws. It would show examples, explain known synthetic giveaways, clarify when provenance review is required, and define escalation pathways. A resident, attending, technologist, or image librarian who suspects a synthetic or mislabeled image should know who reviews it, which system record matters, whether the image remains visible, and how patient-facing communication is handled.
Departments using synthetic images for teaching or model development need extra discipline. Synthetic material can be valuable, but value does not remove the need for boundary control. If a teaching image, test image, or vendor demo image can drift into a clinical workflow without persistent labeling and auditability, the governance failure has already happened before anyone asks whether a radiologist can spot the difference.
The Communications Plan Belongs Before The Incident
Trust failures in imaging rarely arrive as one clean scandal. They arrive as a portal message, a disputed screenshot, a family member asking whether an image was “made by AI,” a news story about synthetic scans, or a physician who wants reassurance before relying on an outside study. By the time communications teams are drafting a public statement, the organization is already explaining under pressure.
Healthcare organizations should prepare language that distinguishes authentic acquisition, AI-assisted processing, synthetic simulation, and uncertainty. They should also decide who is allowed to make those distinctions publicly. Radiologists should not be left to improvise institutional policy at the point of care, and communications teams should not be asked to explain imaging provenance without technical support from imaging informatics, compliance, and clinical leadership.
The strongest messages will be specific without being falsely absolute: what the institution knows about the image’s origin, what systems record that information, what role the image played in care, whether AI was used and how, and what review is available if a patient or clinician has a concern. That kind of answer does more than reassure. It gives confidence somewhere to stand.
The trust crisis has not swallowed medical imaging. That would overstate the evidence. But the mechanism is no longer hypothetical: political communication has shown how synthetic-image awareness creates room to dismiss real evidence, and radiology research has shown that specialists can be fooled by synthetic X-rays under experimental conditions. Preparedness is now a governance issue, not a distant reputational scenario.
References
- “Trump’s use of AI images further erodes public trust, experts say,” PBS NewsHour.
- “AI images hurricanes disasters propaganda,” NPR, October 18, 2024.
- “Harff (2026), Computers in Human Behavior,” Computers in Human Behavior, August 2026.
- “ScienceDaily coverage of the Radiology study,” ScienceDaily, March 2026.
- “PBS coverage of C2PA provenance standards,” PBS NewsHour, January 2026.
Comments
Join the discussion with an anonymous comment.