The statute of limitations problem in a switched-at-birth medical malpractice claim does not begin with a lawyer’s calendar. It begins with a DNA result that arrives decades after the nursery has been remodeled, the staff has retired, and the paper chart may have been lawfully destroyed.
That is what makes the North Dakota lawsuit filed by two men switched as infants so difficult to fit inside ordinary malpractice timing rules. Kyle Bylin and Jeremy Morrison were born at the same hospital in 1988, raised by the wrong families, and learned of the switch through consumer DNA testing 38 years later. The hospital said its records from 1988 “no longer exist.”[1] In a standard claim file, missing records can be an evidentiary problem. In this setting, they are also part of the injury’s architecture: the very system that could have documented what happened is gone by the time the harmed people can reasonably know there is anything to investigate.

The legal question is not whether the switch matters. It plainly does. The harder question is whether a court can hear the case at all when ordinary medical malpractice deadlines often run in one to three years, while the injury may remain functionally invisible for 20, 40, or 60 years. Consumer DNA testing has not changed the underlying hospital event; it has changed the moment at which the event becomes knowable.
DNA discovery has turned old nursery errors into current claims
The North Dakota case is not an isolated curiosity. In New York City, a man alleged he discovered through DNA testing that he had been switched at Jamaica Hospital 64 years earlier.[2] In Oklahoma, two women learned through DNA testing that they had been switched 57 years before.[3] These cases have emerged in the same broad period in which consumer genetic databases have made biological relationships visible to people who previously had no reason, or no practical tool, to question the families and medical histories recorded at birth.
The frequency of switched-at-birth incidents remains uncertain. The available materials support the narrower statement that such incidents are described as rare, not a precise rate. For hospitals, however, rarity does not eliminate exposure when the alleged error is severe, the discovery is recent, and the documentation is incomplete or unavailable. A risk file can be statistically unusual and still be institutionally serious.
The Wyoming Supreme Court’s decision in Larsen v. Banner Health System remains the older doctrinal reference point. There, families alleged that two infants born in 1958 were switched and did not learn the truth until more than four decades later. The court held that emotional-distress claims could proceed in response to the certified question before it, recognizing the seriousness of the alleged injury.[4] But Larsen did not resolve the statute-of-limitations defense. That omission matters because recognition of an injury and timeliness of a lawsuit are separate gates.
Three timing questions courts should not collapse
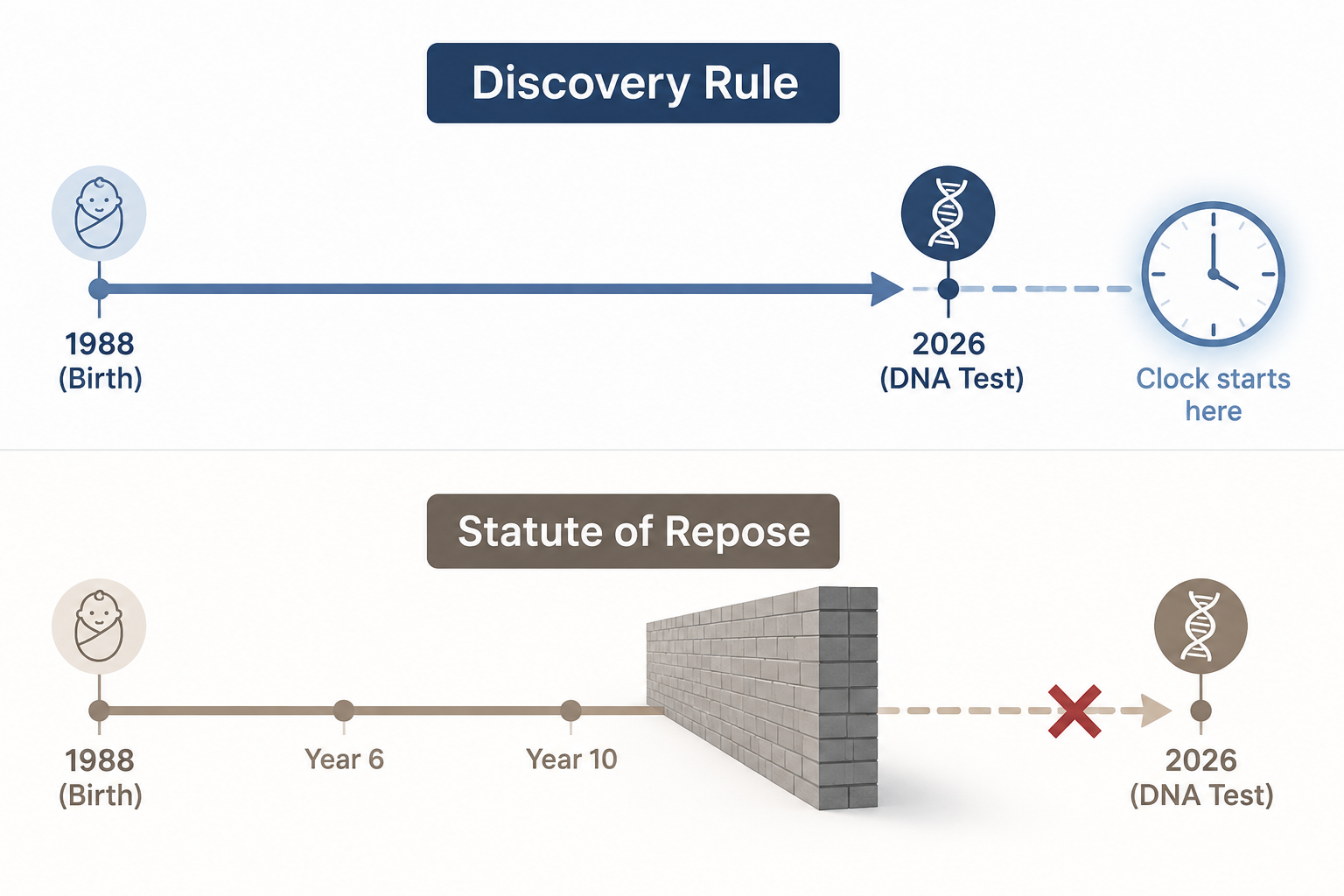
Switched-at-birth claims tend to blur three questions that ordinary malpractice cases can sometimes keep separate. The first is when the plaintiffs actually discovered the injury. The second is whether they reasonably should have discovered it earlier. The third is whether a statute of repose bars the case regardless of discovery.
| Question | Why it matters in DNA-discovered switch cases |
|---|---|
| Actual discovery | The DNA result may be the first credible notice that the birth record and biological lineage were wrong. |
| Constructive discovery | A defendant may argue that plaintiffs should have investigated earlier, but courts have not resolved when ordinary people should be expected to use consumer DNA testing. |
| Repose | A hard outer deadline may bar the claim even if discovery was impossible before the deadline expired. |
The first question is the most intuitive. If a DNA match reveals that a person’s recorded parents are not biological relatives, the date of that result gives plaintiffs a clear discovery date. The second question is less settled. Consumer DNA testing is widely known now, but that does not automatically mean a reasonable adult should test simply to verify a hospital birth record that no one had reason to doubt. The law has not yet supplied a stable answer to when availability of DNA testing becomes constructive knowledge.
The third question is the most important for plaintiffs and for institutional risk analysis. A claim can be newly discovered and still legally barred if a repose statute has already closed the courthouse door.
Why the discovery rule helps, but only partway
In medical malpractice law, a limitations period ordinarily requires a patient to sue within a specified time after the injury or after the injury is discovered. General medical malpractice limitation periods are commonly described as falling in the one-to-three-year range, depending on the state.[5] The discovery rule exists because some injuries are not reasonably apparent when the medical act occurs. A patient should not lose a claim before having a fair opportunity to know that a claim exists.
That principle has obvious force in a switched-at-birth case. The adults harmed by the switch are not overlooking a surgical scar, ignoring a lab result, or delaying after a known adverse event. They are living inside incorrect records. Their family history, genetic risk information, ancestry, and kinship assumptions may all point in the wrong direction. Before DNA testing supplies contradictory evidence, there may be no symptom that reasonably tells them to investigate the hospital nursery.
Foreign-object cases are a useful analogy, but an incomplete one. Many jurisdictions treat a surgical sponge or instrument left inside a patient as the type of hidden injury that may justify delayed accrual under a discovery rule.[6] A baby switch is also hidden, and the institution’s role may not be discoverable at the time it occurs. But the analogy begins to strain because the injury is not a concealed object inside one patient’s body. It is a lifelong relational and identity error distributed across multiple families, medical histories, and records.
The discovery rule can therefore answer one fairness problem: it can give legal significance to the moment the DNA result reveals the switch. It cannot, by itself, answer whether a legislature has imposed an absolute outer deadline.
The harder barrier is repose
A statute of limitations and a statute of repose are often discussed together, but they do different work. A limitations period usually runs from injury, discovery, or a legally defined accrual date. A repose period runs from the defendant’s act or omission and sets a final outside date after which a claim cannot be brought, even if the injury was not and could not reasonably have been discovered.
Secondary legal compilations describe medical malpractice repose periods in roughly 35 states, often with hard caps in the four-to-ten-year range.[7] Those compilations are useful for orientation, not a substitute for statutory verification. The exact rule depends on jurisdiction, amendments, exceptions, minors’ provisions, fraud or concealment language, and how courts interpret the statute. But the practical point is clear enough: a DNA-discovered switch can look timely under a discovery rule and still be barred under repose.
That distinction explains why the same factual revelation may have very different legal consequences from one state to another. A person who discovers a 38-year-old switch in a jurisdiction with a flexible discovery rule and no applicable repose bar may have a plausible timeliness argument. A person with the same DNA result in a jurisdiction with a strict repose statute may face dismissal before the court reaches causation, damages, or the credibility of the hospital’s historical records.
This is where administrative closure and lived reality separate. From a hospital’s record-management perspective, a decades-old chart may be beyond the required retention period. From the family’s perspective, the first meaningful notice may arrive only after that chart is gone. Neither fact cancels the other. Together, they produce the central institutional problem: the evidentiary system was designed around ordinary discoverability, while the injury was concealed by the ordinary documents themselves.
Larsen recognized the injury but left the timing fight for another day
Larsen is sometimes treated as if it settled switched-at-birth liability. It did not. The Wyoming Supreme Court addressed whether the plaintiffs could recover for emotional distress in the circumstances presented by the certified question. The court concluded that they could pursue those claims, rejecting the idea that the alleged harm was legally too remote or too intangible.[4]
For today’s DNA-discovered cases, Larsen is important but limited. It shows that a court can take the injury seriously. It does not tell hospitals, insurers, or plaintiffs what happens when a defendant raises a statute-of-limitations or statute-of-repose defense against a claim discovered only after modern DNA testing. The unresolved issue is not whether a family can suffer compensable harm from a switch. It is whether the law permits that harm to be litigated after the ordinary malpractice clock has expired many times over.
The newer North Dakota, New York, and Oklahoma disputes may bring that timing conflict closer to direct review, but their current posture matters. Ongoing lawsuits are not appellate answers. A complaint can allege a compelling injury and still be dismissed on timing grounds. A trial court can permit discovery without resolving the broader question for other jurisdictions. Until an appellate court squarely addresses a DNA-discovered switched-at-birth claim against a repose defense, the most important legal barrier remains unsettled.
Hospitals now face historical claims in a genomic visibility environment
For healthcare institutions, the lesson is not that every decades-old birth record must have been kept forever. Record-retention systems operate under legal, clinical, storage, and privacy constraints. A hospital cannot realistically insure against every factual uncertainty from a delivery unit that closed a generation ago.
But it is equally unsafe to treat expired retention periods as if they make the underlying event institutionally irrelevant. Consumer DNA testing has created a new discovery mechanism for old errors. A claim involving a missing 1988 record is not merely a stale-file problem; it may be a current notice event for people who could not have known earlier that the file mattered.
Risk teams reviewing these matters need a different first pass than the usual malpractice intake checklist. The core questions are procedural before they are emotional: when did the DNA result occur, what did it show, who received it, what hospital records still exist, what retention policy applied, whether any legal hold was triggered, which state’s limitation and repose rules govern, and whether any exception could plausibly apply.
- Identify the first documented DNA-based notice date, not merely the date of birth.
- Separate missing-record analysis from liability analysis; lawful destruction may affect proof without answering discoverability.
- Verify the governing state’s current statute of limitations and repose from primary legal sources.
- Treat similar family members and counterpart families as part of the same exposure map, because the injury is relational.
- Avoid assuming that a DNA test automatically revives a claim or that repose automatically resolves every institutional consequence.
Standard medical malpractice deadlines were built for injuries that usually surface near the period of care or can at least be investigated with contemporaneous medical records. Switched-at-birth claims discovered through consumer DNA testing do not fit that model cleanly. The discovery rule offers a partial route by recognizing that the injury may not become knowable until the DNA result. Statutes of repose remain the hard unresolved barrier, especially in jurisdictions that cut off claims a few years after the original act regardless of later discovery.
That leaves hospitals in an uncomfortable but practical position. A claim may be legally stale, factually underdocumented, emotionally severe, and newly discoverable all at once. Historical record policies, legal holds, insurer notice, and early claims triage now sit inside a genomic environment that can make a decades-old nursery event visible for the first time in 2026.
References
- Men switched at birth sue North Dakota hospital after DNA test discovery, AP News, July 2026.
- Man switched at birth 64 years ago sues Jamaica Hospital after DNA test, NBC New York, 2025.
- Two women switched at birth 57 years ago discovered the truth through DNA testing, Business Insider, 2022.
- Larsen v. Banner Health System, 2003 WY 167, 81 P.3d 196, Wyoming Supreme Court, 2003.
- Medical Malpractice Lawsuit Requirements, Justia.
- Discovery Rule in Medical Malpractice Cases, National Medical Malpractice Authority.
- Medical Malpractice Statute of Limitations by State, Sokolove Law; Medical Malpractice Statute of Limitations by State, Cerebral Palsy Guide, 2026; Medical Malpractice Statutes of Limitations by State, Levin & Perconti; Medical Malpractice Statute of Limitations by State, Tavrn, 2026.
Comments
Join the discussion with an anonymous comment.