Predicting health impacts from the air quality index is not one problem. It is at least two. The first is a forecasting problem: given satellite, sensor, weather, and historical pollution data, can a model classify or predict an AQI category with useful accuracy? The second is a health translation problem: given an exposure estimate, what can be said about asthma exacerbations, cardiovascular events, premature mortality, or other population-level outcomes?
The distinction matters because the strongest AQI models are beginning to look operationally impressive. In one 2026 study, a hybrid CNN-LSTM model reached a 91.07% F1-score and 98.27% accuracy for AQI classification, while a bidirectional LSTM reached a 91.62% F1-score. But the same work reported only a 46–49% range when AQI category was mapped to disease risk probability, which is a different and more clinically consequential claim.[1]
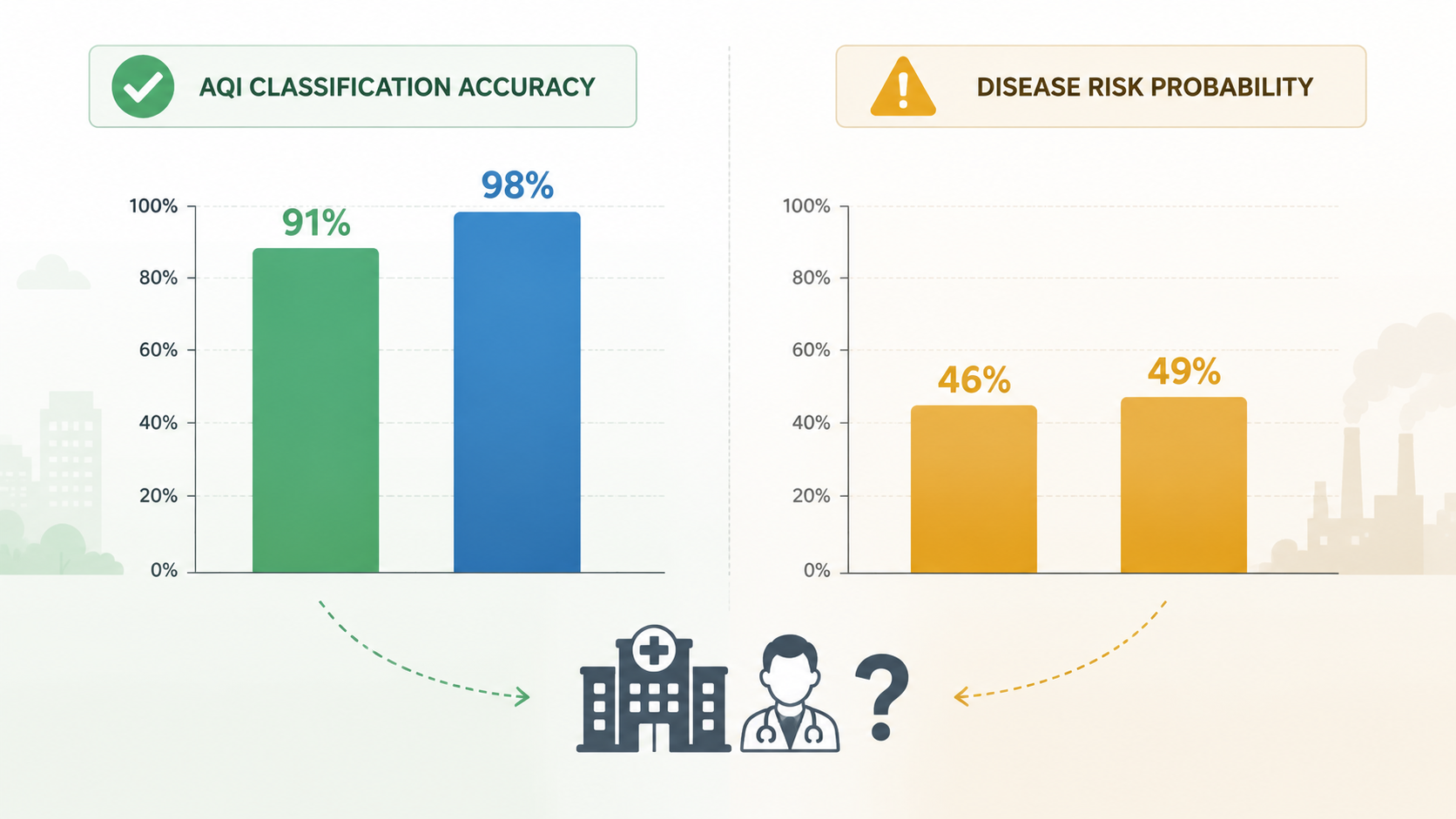
That gap is not a technical footnote. It is where a dashboard stops being a pollution forecast and starts implying something about bodies, clinics, hospitals, and deaths. A public health analyst can use a strong AQI forecast to prepare messaging or staff an alert system. The same analyst should not treat a disease-risk percentage as validated just because the upstream AQI classifier performed well.
Where the Health Claim Enters
The modern pipeline usually starts with exposure estimation. Satellite aerosol optical depth can help infer particulate pollution over wide areas. Ground monitors anchor those estimates to local measurements. Meteorological variables such as wind, humidity, and temperature help models account for dispersion and atmospheric chemistry. In some systems, electronic health records or other outcome data enter later, either for model development, validation, or downstream burden estimation.[2]
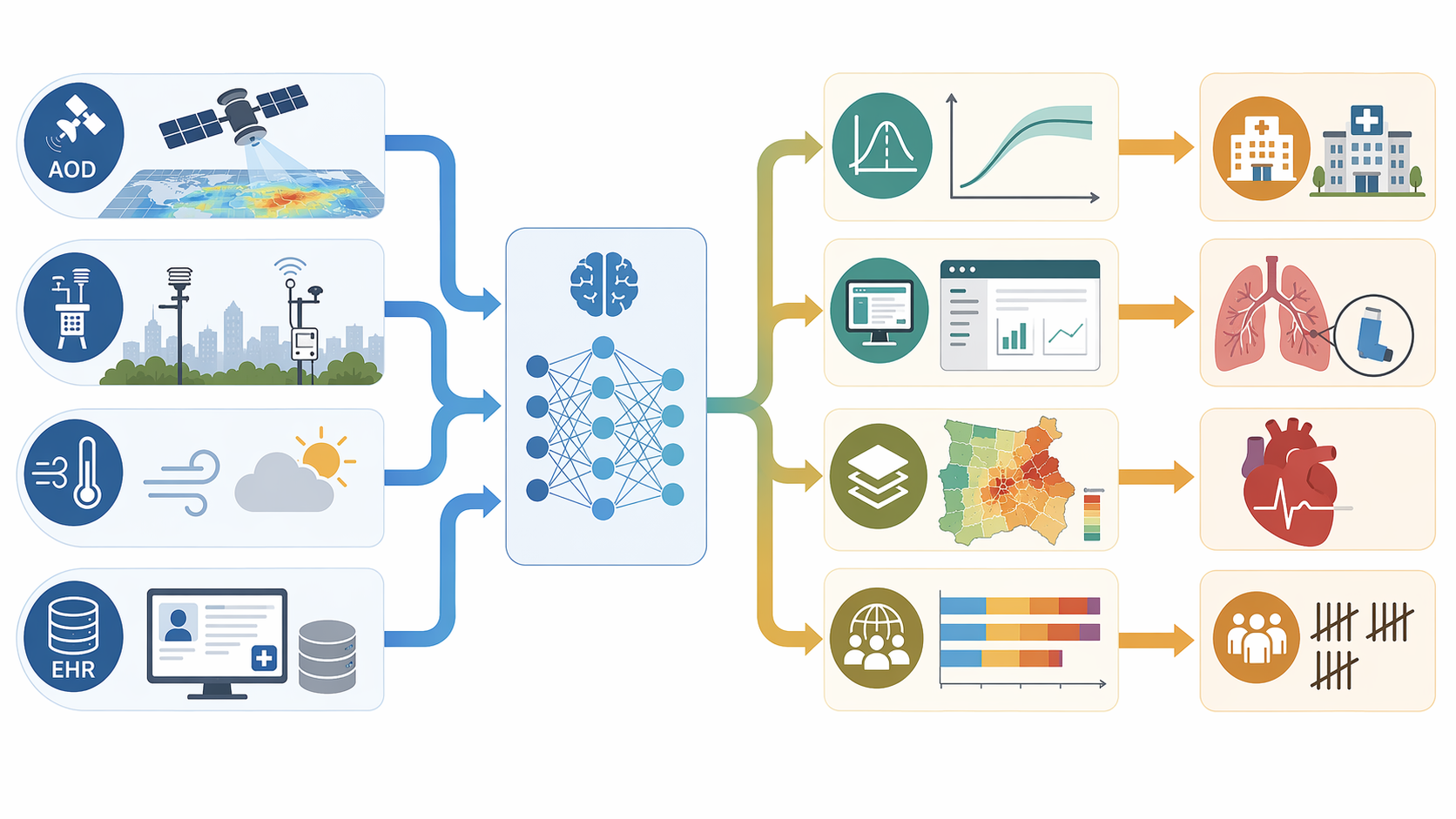
The AI layer can improve the exposure side of the pipeline. Models can fuse heterogeneous data sources, fill spatial gaps where monitors are sparse, forecast short-term pollution changes, and emulate more computationally expensive atmospheric models. A review of AI health-risk assessment methods describes this as a synthesis of satellite AOD, ground sensor data, electronic health records, and meteorology feeding concentration-response models derived from established epidemiological frameworks, including GEMM, IER, AirQ+, and GBD functions.[2]
The epidemiological layer is where exposure becomes burden. GEMM, the Global Exposure Mortality Model, links long-term fine particulate exposure to mortality outcomes. IER, or integrated exposure-response modeling, was developed to estimate risk across wide exposure ranges. AirQ+ and BenMAP-CE are health impact assessment tools that can estimate attributable cases under specified exposure and concentration-response assumptions. GBD-based functions draw on Global Burden of Disease methods to connect exposure distributions with disease burden estimates.
These frameworks do not make the AI model medically validated by association. They provide the mathematical and epidemiological machinery for asking a health question after the exposure question has been answered. If the exposure estimate is biased, if the concentration-response function is imported from a population unlike the one being assessed, or if the outcome definition is weak, the final health estimate inherits those weaknesses.
Forecasting Accuracy Is Useful, but It Is Not Outcome Validation
AQI classification metrics answer a narrow question: did the model put a place and time into the correct pollution category? They do not answer whether the predicted category correctly estimated emergency department visits, asthma exacerbations, arrhythmia risk, or excess mortality in the exposed population.
That is why the Madan et al. contrast is so important. A 98.27% accuracy figure can make a system look nearly settled if the endpoint is AQI category. The reported 46–49% disease risk probability range makes the health translation look much less settled. The same model family can be strong for pollution classification and still coarse for health-risk estimation.[1]
This does not make forecasting irrelevant for health work. A reliable forecast can give a health department more time to issue advisories, prepare shelters or clean-air spaces, adjust outreach to high-exposure communities, or coordinate with clinicians who serve respiratory and cardiovascular patients. Preparedness can benefit before a model is ready for patient-level clinical decision support.
The sharper point is that preparedness and prediction are different claims. A system can be valuable for operational surveillance while still lacking validation as a disease-risk instrument. The same distinction shows up across other forms of AI public health surveillance, where early warning and case-level inference require different evidentiary standards.
What Model Fusion Adds
One reason AI has gained ground in air-quality work is that it can combine approaches that used to sit in separate boxes. Chemical transport models describe atmospheric processes, but they can be computationally demanding and sensitive to emissions inventories. Measurement networks provide observed data, but they are geographically uneven. Machine learning can learn patterns from both, especially when satellite and meteorological data are added.
Machine learning-measurement model fusion has been reported to achieve more than 90% forecasting accuracy, with performance described as 66% more accurate than chemical transport models alone and 12% more accurate than standalone machine learning.[3] Those figures support a practical conclusion: fusion approaches can make near-term AQI forecasting more usable for public health operations.
They do not settle the burden-estimation question. A better exposure forecast is a stronger input to a health impact model, but it remains an input. The health estimate still depends on the selected concentration-response function, the baseline disease rate, population age structure, vulnerability assumptions, exposure duration, and whether the model has been checked against actual outcomes.
The Older Epidemiology Still Carries the Weight
When an AI system estimates premature mortality from PM2.5, the mortality claim usually comes from an established exposure-response model rather than from the neural network itself. The AI may estimate or forecast concentrations. The burden framework converts those concentrations into attributable health outcomes.
The scale of those burden estimates can be large. The Global Exposure Mortality Model has been used to estimate 10.2 million premature deaths attributable to fossil-fuel PM2.5 in 2012.[2] That number is not an AI result by itself; it is an epidemiological estimate. AI becomes relevant when it helps produce more granular, more frequent, or less computationally expensive exposure fields that can be passed through similar burden-estimation machinery.
This is also where transparency becomes non-negotiable. A health-risk map should state which concentration-response function it used, which pollutant and averaging period drove the estimate, which baseline rates were assumed, and which population groups were included. Otherwise, a polished interface can hide the most consequential choices.
The Evidence Base Is Smaller Than the Dashboard Economy Suggests
The 2026 epidemiological review by Patil and Agrawal is useful because it sizes the field without pretending it is already mature. The review included 83 studies, but only 18 reported correlation coefficients suitable for meta-analysis. Its publication-bias test could not confirm bias, with Egger’s regression test reported as z = −0.9024 and p = 0.3668, but the authors noted that the analysis was underpowered because of the modest number of studies.[2]
That is not a minor methods complaint. If most studies cannot contribute comparable effect metrics, it becomes hard to determine whether model performance is stable across pollutants, populations, seasons, health outcomes, and monitoring environments. It also limits confidence in claims that AI-driven air-pollution health-risk estimation has generalized beyond its best-studied settings.
The geography of the evidence base is another constraint. The review found that most studies focused on metropolitan areas in Asia and Europe, while Sub-Saharan Africa, Eastern Europe, and rural regions globally were severely underrepresented.[2] This matters both for exposure and for health translation. Sensor density, fuel sources, housing conditions, baseline disease rates, health-system access, and age structure can all change the meaning of the same pollutant concentration.
Underrepresentation is not just an academic limitation. It can become an algorithmic disparity when models trained or validated in data-rich cities are presented as if they travel cleanly to places with sparse monitors, different exposure mixtures, or weaker hospital reporting. That concern is adjacent to the broader problem of algorithmic bias in public health AI, but air pollution adds a physical layer: the model may be biased because the air, the sensors, and the clinical record are all unevenly observed.
Real-Time Maps Are Operational Examples, Not Clinical Proof
Real-time mapping is one of the field’s most visible advances. Rajesh et al. proposed a machine learning-driven framework for real-time air quality assessment and predictive environmental health risk mapping with 5-minute refresh cycles and Health Risk Index mapping.[4] For emergency preparedness, that cadence is attractive. It can help agencies see where conditions are changing and where alerts may need to be targeted.
But a frequently refreshed Health Risk Index is not the same as demonstrated prediction of hospital admissions. The Rajesh et al. framework has not been validated against actual hospital admission records.[4] That makes it an operationally interesting system, not proof that a 5-minute health-risk map can accurately predict near-term clinical burden.
The same caution applies to personalized response modeling. The AI-Respire framework used an adversarial autoencoder, LSTM, and transfer learning to predict individualized physiologic responses to pollution. It reported predicted vital sign shifts under simulated 100% pollution spikes—breathing rate increasing by 3.5% and heart rate by 2.5%—and cross-validated those predicted shifts against the independent U-BIOPRED clinical cohort.[5]
That cross-validation makes AI-Respire more clinically interesting than a map that never touches outcome data. It still does not make the framework longitudinally validated. Cross-sectional agreement with an independent cohort is useful evidence, but it does not show that the model can prospectively predict future exacerbations, admissions, or disease progression in exposed individuals.
Preparedness Can Move Faster Than Clinical Validation
The strongest near-term use case is not bedside decision support. It is preparedness. Johns Hopkins APL reported an AI system that produces 10-day AQI forecasts from 21 hours of input data, a design meant to improve air-quality forecasting for health-relevant planning.[6] A 10-day horizon can matter for staffing, public messaging, school or outdoor-event guidance, and coordination during smoke or pollution episodes.
That does not require pretending the system has solved clinical risk prediction. A health department can act on a credible forecast without telling clinicians that an individual patient’s near-term event probability has been validated. Population-level triage and clinical prediction sit on different evidentiary rungs.
This distinction is easy to lose during high-smoke or high-ozone episodes, when demand for actionable maps rises quickly. In those moments, the question is not whether AI is useful. It is which decision the model is being asked to support, and whether the validation matches that decision.
How to Read the Next Health-Risk Claim
A credible AQI health-impact model should separate its performance claims. AQI classification accuracy belongs in one box. Exposure estimation error belongs in another. Health burden estimation belongs in a third. If a paper or product reports only F1-score, accuracy, or forecasting error, it has not validated disease burden.
- External health validation: the model should be tested against hospital admissions, EHR outcomes, emergency visits, mortality records, or longitudinal cohort data when it makes outcome claims.
- Transparent concentration-response assumptions: the system should identify whether it uses GEMM, IER, AirQ+, BenMAP-CE, GBD-based functions, or another framework.
- Population specificity: baseline rates, age structure, comorbidity patterns, and local exposure conditions should be stated rather than implied.
- Geographic reporting: performance should be reported beyond data-rich metropolitan areas, especially where sensor density and health records are limited.
- Endpoint clarity: alerts, burden estimates, and individual clinical predictions should not be treated as interchangeable outputs.
The current evidence supports a calibrated position. AI-enabled AQI health risk estimation is more mature than simple AQI prediction when it is coupled to established epidemiological burden frameworks. It is operationally plausible for surveillance and preparedness. It is not yet a validated clinical risk prediction instrument.
References
- Hybrid deep learning model for air quality prediction and its impact on healthcare, Nature Scientific Reports, 2026.
- AI Assessment of Health Risk Based on Air Pollution: An Epidemiological Review, Environmental Sciences Europe, 2026.
- AI can help forecast air quality, but freak events like 2023's summer of wildfire smoke require traditional methods too, The Conversation, 2023.
- Machine learning-driven framework for realtime air quality assessment and predictive environmental health risk mapping, Nature Scientific Reports, 2025.
- An AI-driven framework for the prediction of personalised health response to air pollution, arXiv, 2025.
- Using Artificial Intelligence, Better Pollution Predictions Are in the Air, Johns Hopkins APL, 2024.
Comments
Join the discussion with an anonymous comment.