For a hospital or public health agency, the practical question around AI in flood prediction and emergency response is not whether a model can draw a cleaner inundation map. It is what changes before the water arrives: whether dialysis patients can be moved, whether an emergency department can staff for a surge, whether shelters know which neighborhoods will need transport, whether public health teams can watch for infectious disease earlier, and whether relief reaches damaged high-poverty areas before the easiest-to-see places absorb the first wave of help.
The current evidence supports part of that chain. AI-enabled flood systems can extend useful warning time, improve nowcasts in regions where traditional hydrologic infrastructure is thin, and help target post-disaster resources. The evidence does not yet show that these tools reduce flood-related mortality, injury, or disease incidence. That distinction matters. Forecast lead time is valuable, but it is not the same thing as a health outcome.

The strongest case is lead time
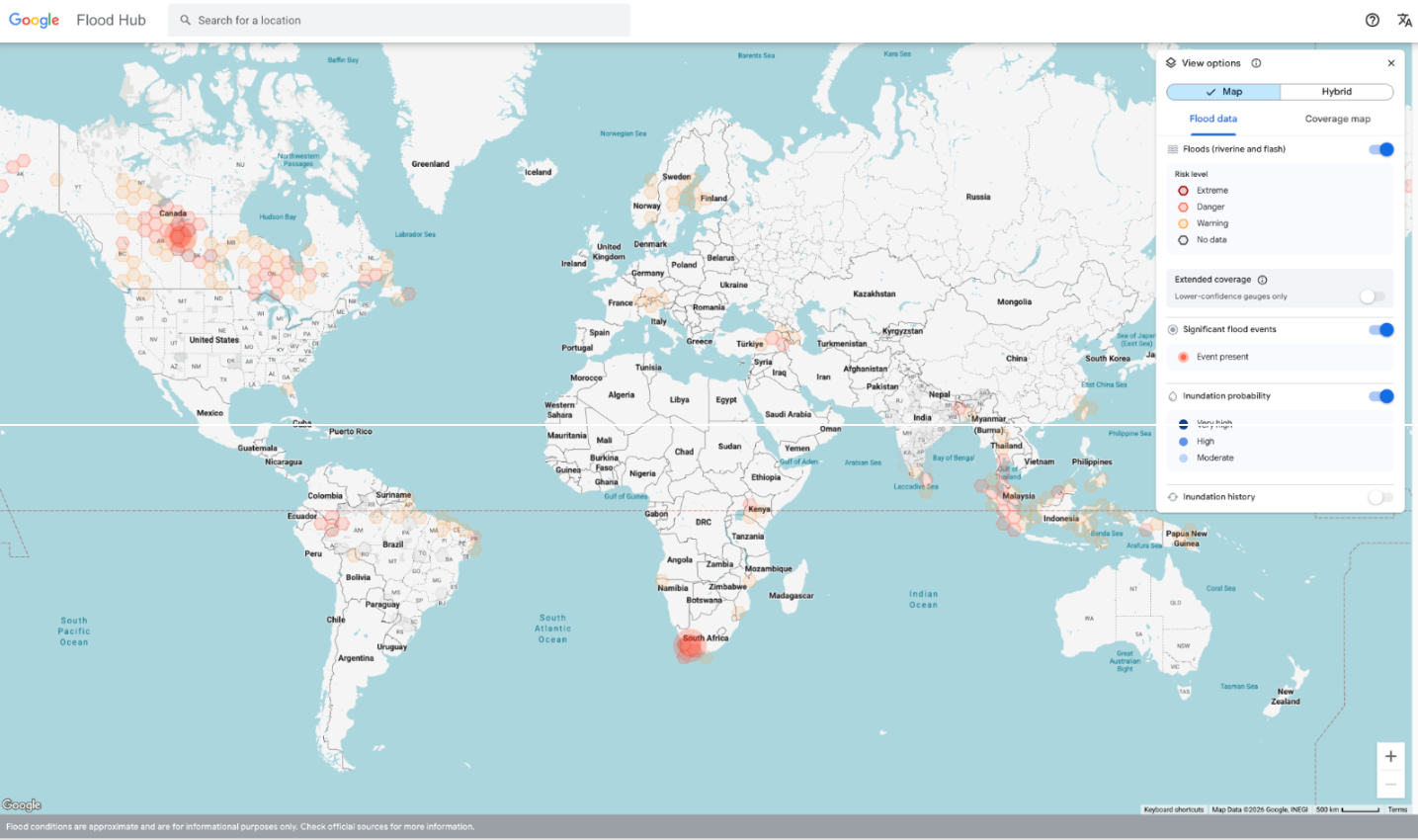
The most important peer-reviewed evidence comes from Google’s global flood forecasting work published in Nature in 2024. The study reported that machine learning extended reliable flood nowcasts from zero days to five days and achieved forecast accuracy in Africa and Asia comparable to what had previously been available in Europe through conventional systems.[1] Google’s operational Flood Hub also reports coverage in more than 150 countries, reaching about 2 billion people.[2]
Five days is not a magic interval, but it is operationally meaningful. A same-day alert may tell a hospital to brace. A five-day warning can let a system check generator fuel, discharge patients who can safely leave, adjust elective schedules, stage ambulances, confirm oxygen and medication supply, and coordinate with long-term care facilities that cannot move residents quickly. For public health departments, it can also create time to pre-position clean water messaging, identify shelter staffing needs, and prepare surveillance for diarrheal illness, wound infections, and respiratory complications after displacement.
That is why the Google evidence deserves attention even though it is not health-outcome evidence. Flood forecasting has always been part of health preparedness because hospitals and EMS agencies make time-dependent decisions. If an AI system buys several usable days in places with limited gauge infrastructure, the preparedness value is real enough to pilot. The unsupported leap would be claiming that the added days have already been shown to prevent deaths or disease at population scale.
The geographic result is especially relevant. Flood health burdens are often severe in lower-resource settings, while hydrologic monitoring networks and historical data have been concentrated in wealthier regions. A system that performs more comparably across Africa, Asia, and Europe begins to address a practical weakness in traditional flood warning, not merely a technical benchmark. Still, coverage is not the same as trustworthiness in every watershed, and a global map should not be mistaken for local validation.
Prediction has to survive the handoff
A flood forecast becomes health preparedness only after someone acts on it. The warning has to reach an emergency operations center, a hospital incident command team, an EMS coordinator, a mayor’s office, or a public health nurse with authority to move resources. Then come the slower steps: deciding whether to evacuate, which roads can still carry patients, which clinics may close, which shelters can take medically fragile residents, and which neighborhoods will be undersupplied if the response relies only on visible damage reports.
This is where forecast accuracy can become a misleading comfort. A model can be directionally right and still fail to change health operations if alerts are not integrated into call trees, bed management, supply chain decisions, or public communications. A tool can also perform well on ordinary floods and then fail during an extreme event that sits outside its training experience. In disaster medicine, those are not marginal cases. They are the events that decide whether people trust the system the next time.
The research brief documents out-of-distribution failure as a limitation across major prediction models, including P2M, Errorcastnet, and a Penn State differentiable model. For health systems, that limitation should be treated as operational, not academic. A hospital does not need a post-event explanation that the rainfall pattern was unusual; it needs to know beforehand whether the model has been stress-tested against rare, severe, and compound events.
Resource targeting is closer to response than forecasting
The GiveDirectly and Google example after Hurricanes Helene and Milton shows a different role for AI: not predicting the flood, but helping route aid. As described in RAND’s 2025 commentary citing Associated Press reporting, an AI computer vision tool identified storm-damaged high-poverty areas from satellite imagery, and GiveDirectly delivered $1,000 in cash relief per household.[3]
This is a narrower but more concrete proof of concept. It does not establish improved health outcomes, and it should not be inflated into a general claim about disaster equity. But it does show a practical use case that emergency managers will recognize: after a major storm, official damage assessments lag, communications fail, and the first reports can overrepresent communities with better connectivity or louder political access. Satellite-based triage can make relief less blind if it is checked against local knowledge and if the targeting criteria are transparent enough to contest.
For health agencies, the analog is not hard to imagine. A similar workflow could help prioritize mobile clinics, bottled water distribution, pharmacy access, or outreach to medically vulnerable residents. The evidence does not yet prove those downstream benefits. It does, however, identify a plausible response function where AI may be useful before formal assessments are complete.
The infectious disease evidence is promising, but thin
The closest health-specific evidence comes from a 2025 retrospective cohort study by Safari and colleagues examining infectious disease after the 2022 Iranian floods. The study reported that disease prevalence increased from 39.5% before the floods to 47.3% after the floods, with an odds ratio of 1.38 and a relative risk of 1.20.[4]

The modeling results were moderate. A Random Forest model reached an AUC of 0.76, compared with 0.71 for Gradient Boosting and 0.69 for an artificial neural network.[4] The study also found a counterintuitive risk pattern: younger adults aged 18 to 40 were at higher risk than older groups.[4] That finding is worth attention because disaster health planning often defaults to older adults and people with chronic disease as the obvious high-risk groups. Those groups still matter, but post-flood exposure can follow cleanup work, mobility, household labor, and informal response roles as much as baseline frailty.
| Evidence area | What the evidence supports | What it does not yet prove |
|---|---|---|
| Google Flood Hub and Nature 2024 forecasting evidence | Longer reliable flood nowcasts and broader operational coverage | Reduced deaths, injuries, disease, or hospital surge |
| GiveDirectly/Google post-hurricane allocation example | AI-assisted identification of damaged high-poverty areas for cash relief | Generalizable disaster health benefit or equitable allocation across all settings |
| Safari et al. 2025 infectious disease study | Feasibility of post-flood infectious disease risk prediction with moderate model performance | Clinical-grade readiness or broad deployment across regions |
The caveats are substantial. The Safari study used only four predictor variables, was conducted in a single region, and reported AUC values that are useful for exploration but not strong enough to support broad operational dependence.[4] A model with an AUC of 0.76 may help public health teams decide where to look first. It should not decide, on its own, where care is withheld, where surveillance is relaxed, or which population is assumed to be safe.
This is the point at which health systems should be both interested and demanding. Post-flood infectious disease is exactly the kind of delayed hazard that can benefit from earlier risk stratification. But one retrospective, single-region study cannot carry the burden of operational practice change. The next evidence step is not another polished dashboard; it is prospective testing that measures whether AI-guided surveillance changes case detection, time to intervention, outbreak size, or avoidable utilization.
Operational systems are already moving
Some jurisdictions are already integrating AI into flood operations. The World Meteorological Organization described South Korea’s LSTM-based flood forecasting system operating at 223 locations with 10-minute intervals and integrated with SMS and cell broadcast alerts.[5] The same report noted that the system is being exported to Indonesia, Laos, and the Philippines through KOICA.[5]
That integration is important because an alerting channel is part of the intervention. A forecast that stays inside a technical platform is not an emergency response tool. A forecast connected to public warnings, local protocols, and accountable decision-makers has a chance to change behavior, even if the health benefit still needs to be measured.
Academic emergency management work is moving in the same direction. Texas A&M’s UrbanResilience.AI Lab reported field tests during hurricanes Beryl, Milton, and Helene for neighborhood-level evacuation monitoring, power outage tracking, and property damage assessment, and the lab anticipates standard AI tools in emergency management within 3 to 5 years.[6] USC’s Center for Artificial Intelligence in Society describes disaster planning work focused on road fortification optimization and infrastructure resilience modeling.[7]
These projects suggest that AI is becoming part of emergency management workflow, not just hydrologic modeling. That is useful context for health leaders because the hospital will not be the only actor using these tools. County emergency management, utilities, transportation agencies, and relief organizations may all be looking at AI-derived information during the same incident. If hospitals wait until the tools are mature before learning how local partners use them, they may enter the response late.
Frameworks help, but they are not outcome evidence
RAND’s 2025 commentary offers a useful map of the disaster AI landscape, grouping tools into predictive analytics, generative AI and natural language processing, robotics, computer vision, speech recognition, recommendation systems, and fraud detection.[3] It also emphasizes pilot testing, bias monitoring, and ethical guardrails.[3]
That framework is helpful for procurement and planning conversations. It should not be read as a systematic review showing that each category improves disaster outcomes. For health systems, the categories matter only if they connect to a job that someone must do under pressure: predict inundation, send an alert, choose evacuation routes, identify inaccessible neighborhoods, match shelter capacity to medical needs, detect disease clusters, or audit relief distribution.
- Predictive analytics may support earlier flood warnings and surge planning.
- Computer vision may help identify damaged areas before manual assessments are complete.
- Recommendation systems may help prioritize resources, but only if allocation rules are explicit and reviewable.
- Generative AI and speech tools may support communication workflows, but they need tight controls during high-risk public messaging.
The uncomfortable procurement question is who bears responsibility when the model is wrong. If a system underestimates flooding in a low-income area because training data were sparse, the consequence is not a model-performance footnote. It may mean delayed evacuation support, delayed cleanup, delayed water distribution, or delayed clinical outreach. Bias monitoring is therefore not a compliance ornament; it is part of the safety case.
What health systems can reasonably do now
The evidence supports cautious piloting, not full dependence. Health systems should monitor AI flood tools and consider limited pilots for lead time, situational awareness, and targeted allocation. The safest pilots are those that add information to existing emergency management processes rather than replacing human review or established triggers.
A practical pilot should begin with the handoff. Before adopting an AI flood forecast, a hospital or health department should specify who receives the alert, what threshold changes operations, who confirms the forecast with emergency management, which actions are authorized, and how false alarms or missed events will be reviewed. If the tool flags a neighborhood for post-flood disease risk, the plan should state whether that leads to field surveillance, water testing, clinic outreach, mobile pharmacy deployment, or only closer monitoring.
- Prospective evaluation: Measure whether AI-informed actions change response time, evacuation support, case detection, service access, or other health-relevant endpoints.
- Extreme-event testing: Assess performance on rare, severe, compound, and out-of-distribution floods before relying on the tool during crisis operations.
- Bias monitoring: Compare alert accuracy and resource recommendations across neighborhoods, income levels, language groups, and infrastructure conditions.
- Human accountability: Define who can override the system, who documents decisions, and who reviews failures after the event.
- Local validation: Test whether global or regional models perform well in the specific watersheds, roads, facilities, and populations the health system serves.
The burden of proof should rise as the tool moves closer to patient-facing decisions. Using an AI forecast as one input for generator checks or staffing huddles is different from using it to prioritize evacuations, allocate scarce transport, or reduce surveillance in an area judged low risk. The more a recommendation affects who receives help, the more transparent, validated, and auditable it needs to be.
AI in flood prediction and emergency response is ready to be taken seriously by health systems. It is not ready to be treated as proven health protection. The best-supported use today is operational lead time, followed by situational awareness and targeted allocation. The missing evidence is still the evidence that matters most in healthcare: whether these systems measurably reduce harm when floods hit real communities.
References
- Global prediction of extreme floods in ungauged watersheds, Nature, 2024
- Google Flood Forecasting, Google Research
- How AI Is Changing Our Approach to Disasters, RAND, August 2025
- Predicting infectious disease outbreaks after floods using machine learning algorithms: A retrospective cohort study, Health Science Reports, 2025
- The future of flood forecasting: Technology-driven resilience, World Meteorological Organization, 2025
- How AI Tools Are Transforming Disaster Response & Preparedness, Texas A&M Today, October 1, 2025
- AI for Disaster Planning and Response, USC Center for Artificial Intelligence in Society
Comments
Join the discussion with an anonymous comment.