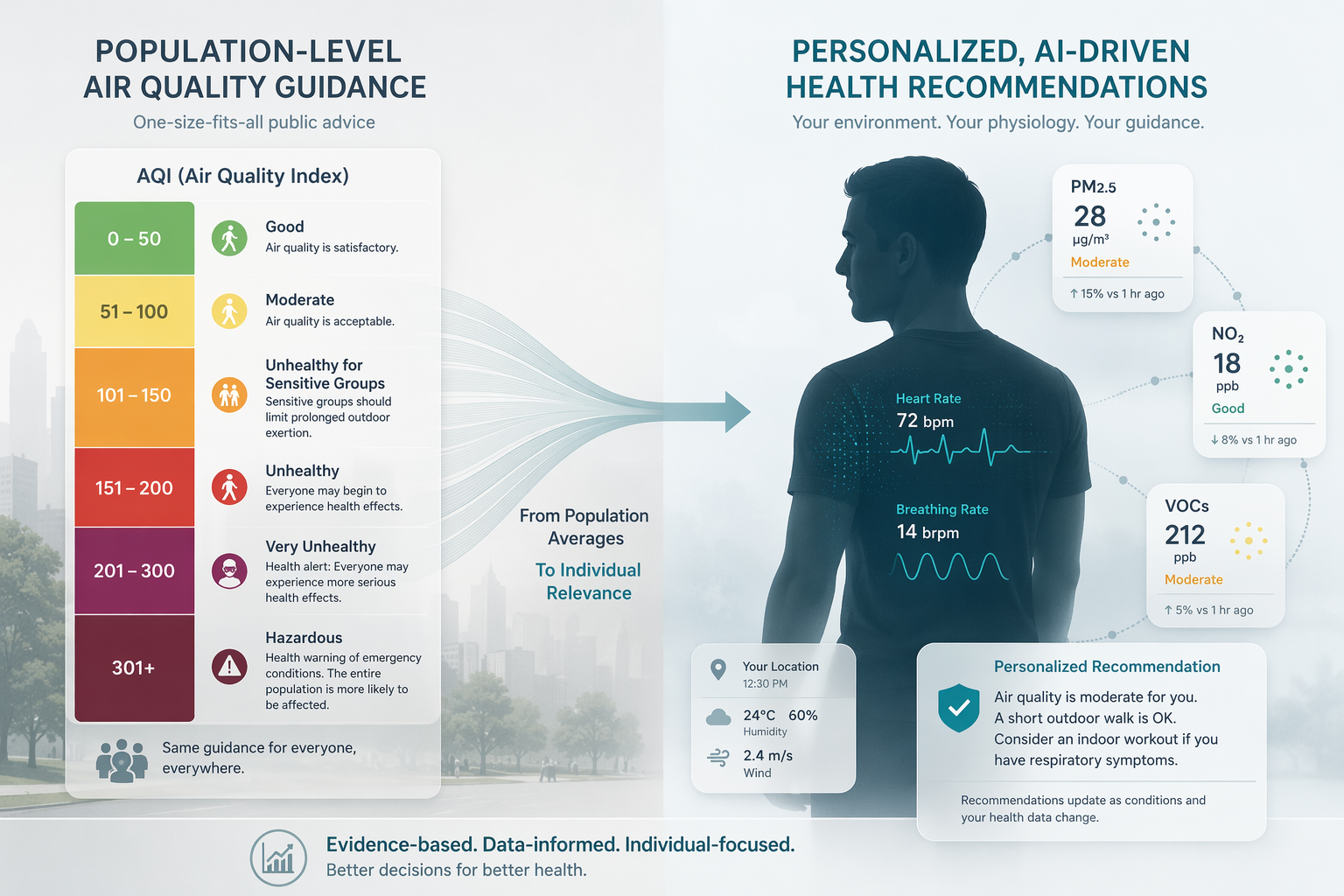
The uncomfortable question for real-time AQI health advice is not whether broad public warnings have value. They do. The harder question is what happens when a population-scale warning is used as if it were a clinical instrument. In one 2024 analysis of U.S. EPA Air Quality Index activity recommendations, more than 18 million general-population adults would need to follow activity restrictions to prevent one atherosclerotic cardiovascular disease event per day.[1] That estimate does not make AQI guidance meaningless. It shows how blunt the tool becomes when the person making the decision is not “the public,” but a patient deciding whether to walk outside, a parent weighing school activity, or a clinician being asked whether a generic alert applies to someone with asthma or COPD.
That distinction matters because the AQI is designed to be legible at scale. Clinical decisions are usually less forgiving. A color band can warn a city, but it cannot know whether one person’s breathing rate reliably rises during pollution spikes, whether another person’s heart rate shifts only under certain pollutant mixtures, or whether a supposedly “moderate” day is physiologically uneventful for one patient and meaningful for another. AI enters this space as an attempt to narrow that gap: not to replace public guidance, but to ask whether real-time pollution data can be joined with individual physiological signals in a way that makes advice more targeted.
Where personalization begins to look technically plausible
The most complete example in the current evidence base is AI-Respire, a 2025 framework that combines high-resolution cohort data with transfer learning from personal smartwatch data.[2] Its appeal is not that it uses AI in the abstract. It is that the modeling target is clinically recognizable: changes in physiological response during air pollution exposure.
The workflow starts with environmental exposure and physiological data, then uses adversarial autoencoders trained on the INHALE cohort to model breathing-rate response. The model is then personalized through transfer learning using smartwatch data from an individual user. In the reported analysis, the framework achieved a mean squared error of approximately 0.003 for normalized breathing-rate prediction.[2] That number is technically encouraging, but it is not the endpoint that should matter most. The more important claim is that an individual’s wearable signals may help the model learn a person-specific response curve rather than applying the same restriction logic to everyone exposed to the same AQI reading.
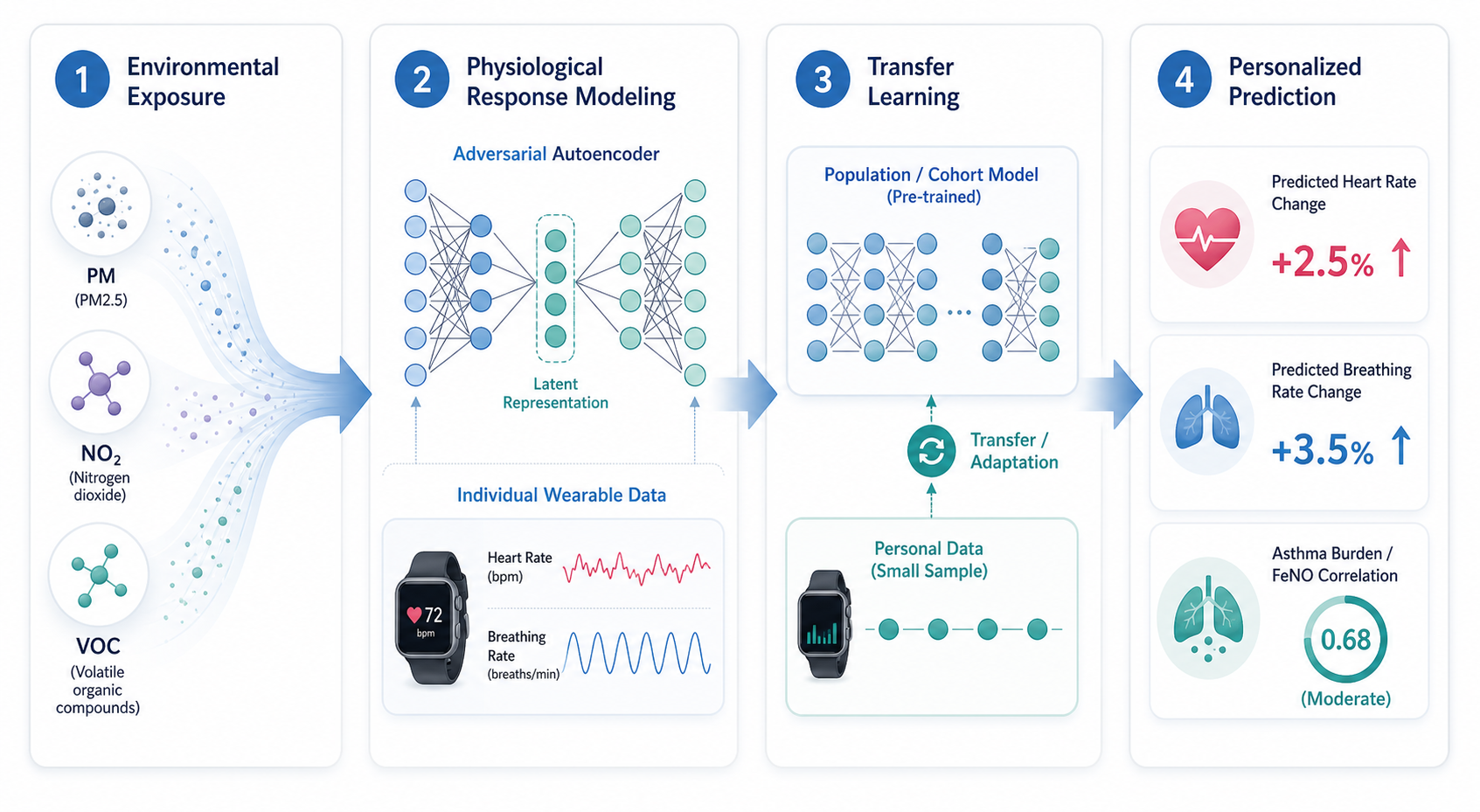
AI-Respire also tested simulated pollution spikes. A modeled 100% increase in pollution exposure was associated with predicted increases of 2.5% in heart rate and 3.5% in breathing rate, and those shifts were linked to asthma burden scores and elevated fractional exhaled nitric oxide in the U-BIOPRED cohort.[2] This is the kind of bridge personalized AQI advice would eventually need: exposure data on one side, measurable physiology on the other, and some relationship to disease-relevant biological signals rather than only a model output.
Still, the human base is very small. The personalization component used 10 healthy, non-asthmatic participants and one user’s 8-month smartwatch data.[2] That is enough to make the approach worth studying; it is not enough to treat it as clinically validated decision support. A model can learn a signal in a carefully bounded setting and still fail when moved into older adults, children, people with multimorbidity, different devices, different housing conditions, or a city with different pollutant patterns.
What the model would need to explain before advice becomes credible
Personalization creates an interpretability problem. If a system tells one person to reduce exposure while giving another person a less restrictive message, the explanation cannot stop at “air quality is poor.” The user, clinician, or public health reviewer needs to know what is driving the recommendation: particulate matter, nitrogen dioxide, volatile organic compounds, an indoor source, a physiological response pattern, or a modeled vulnerability profile.
A 2025 explainable AI study of indoor air pollution shows why that matters. The study applied LIME and SHAP to indoor air quality classification and reported 99.8% classification accuracy on a controlled dataset of 10,559 instances from specific indoor sources.[3] The interpretability methods identified VOC, NO2, and PM10 as the most influential pollutants for personalized health impact.[3] In practice, that kind of attribution could separate a generic warning from a more targeted intervention concept: ventilation, source control, timing of activity, or further investigation of a specific pollutant driver.
The limitation is equally important. A controlled indoor dataset is not the same as a lived indoor environment, where cooking, cleaning, outdoor infiltration, sensor placement, ventilation behavior, building age, and device calibration can all change the signal. The study supports the feasibility of explainable classification; it does not prove that an explainable model will deliver better health outcomes when deployed in homes, clinics, schools, or workplaces.
Risk mapping moves the target from the individual body to the vulnerable population
Another strand of work keeps the real-time ambition but shifts the unit of personalization. A 2025 Scientific Reports framework used an ensemble of Random Forest, gradient boosting regression trees, XGBoost, and LSTM models, updated every 5 minutes, to generate a Health Risk Index.[4] Instead of centering on one person’s smartwatch-derived response, the index weights pollutant exceedance against population vulnerability, including elderly residents, children, and COPD prevalence.[4]
| Approach | Personalization target | What it adds | Main evidence gap |
|---|---|---|---|
| AI-Respire | Individual physiological response | Links pollution exposure with breathing rate, heart rate, transfer learning, and asthma-related signals | Very small human base and no pragmatic outcome trial |
| Indoor explainable AI | Pollutant-specific indoor risk attribution | Uses LIME and SHAP to identify drivers such as VOC, NO2, and PM10 | Controlled dataset may not reflect real-world indoor variability |
| Real-time risk mapping | Population vulnerability groups | Updates risk estimates frequently and incorporates vulnerable-group weighting | Pilot or synthetic validation rather than mature live deployment evidence |
This is a different answer to the same targeting problem. It does not claim to know how a particular patient’s respiratory rate will change after an exposure spike. It asks whether a neighborhood, facility, or region contains people more likely to bear the health consequences of pollutant exceedance. That can be useful for public health operations, but it should not be confused with individualized clinical advice.
The framework also used SHAP-based interpretability, which is a welcome design choice when risk scores may guide resource allocation or warnings.[4] But the evidentiary boundary remains narrow: most machine-learning AQI frameworks, including this type of ensemble approach, have been validated on synthetic pilot data rather than mature live sensor deployments. Frequent updating and model diversity make the system operationally interesting; they do not by themselves establish clinical benefit.
The validation gap is not a footnote
The evidence has moved beyond the idea that real-time AQI health advice must remain one-size-fits-all. It has not moved far enough to show that AI-personalized advice improves outcomes. That distinction is the center of the field as of Q3 2026.
Several limitations recur across the studies. The JAMA Network Open analysis that exposes the targeting problem modeled PM2.5-related exposure reduction and ASCVD events; it did not empirically measure behavior change or include the full complexity of combined pollutants such as ozone.[1] AI-Respire’s personalized component rests on 10 healthy participants and one smartwatch user, not a broad clinical population.[2] The indoor explainable AI study reports very high classification performance, but in a controlled dataset rather than the messier environments where advice would be acted on.[3] The real-time risk-mapping framework is promising as an operational model, but pilot or synthetic validation leaves real-world performance unresolved.[4]
The missing study is not hard to name. A clinically persuasive evidence base would need prospective deployment, real users, clear comparator guidance, measured adherence, and health-relevant outcomes. It would need to show that the advice changes behavior in a safer or more efficient way than standard AQI guidance, without creating unnecessary restriction, alert fatigue, inequitable access, or false reassurance. None of the cited work yet demonstrates that.
Privacy-preserving personalization is an architecture, not proof
Federated learning often appears in this conversation for good reason. A systematic review on integrated air pollution monitoring and health impact assessment describes federated learning as a way to support privacy-preserving personalization across distributed data sources.[5] Conceptually, that matters because the most useful models would likely need data from many people, places, devices, and exposure settings without casually centralizing sensitive physiological records.
But architecture should not be mistaken for validation. Federated learning could make multi-site, privacy-preserving AQI personalization more feasible. It does not answer whether a predicted breathing-rate change should alter advice, whether patients will follow that advice, or whether outcomes improve. Those questions still require clinical and public health evidence, not only better data plumbing.
A disciplined read of the evidence
AI can plausibly make real-time AQI health advice more personal. The strongest reason to think so is mechanistic: models can combine pollutant measurements with physiological data, learn person-specific response patterns, and identify which exposures are driving a risk estimate. That is a meaningful advance over applying the same activity restriction to millions of adults when only a very small number of events may be prevented on a given day.
The evidence does not yet justify treating these systems as clinically proven decision support. AI-Respire is the most instructive framework because it connects real-time exposure, wearable physiology, transfer learning, and asthma-related markers, but its personalization evidence is still early. Explainable indoor models and real-time risk maps add useful adjacent capabilities, especially attribution and vulnerability-weighted surveillance, but they do not close the outcome gap.
As of Q3 2026, the fairest conclusion is narrow: AI-personalized AQI advice is a credible research direction and a plausible way to reduce the mismatch between population alerts and individual risk. It remains an early research application, not validated clinical guidance.
References
- Public Health Relevance of US EPA Air Quality Index Activity Recommendations, JAMA Network Open, 2024.
- An AI-driven framework for the prediction of personalised health response to air pollution, arXiv, 2025.
- Can Explainable AI Assess Personalized Health Risks from Indoor Air Pollution?, arXiv, 2025.
- Machine learning-driven framework for realtime air quality assessment and predictive environmental health risk mapping, Scientific Reports, 2025.
- Towards Integrated Air Pollution Monitoring and Health Impact Assessment Using Federated Learning: A Systematic Review.
Comments
Join the discussion with an anonymous comment.