The hard part of an air quality alert is not telling a family that the air is bad. It is telling the right family what can be changed in the next hour, in the room where a child is actually breathing. A citywide AQI alert may justify keeping windows closed, reducing outdoor activity, or using filtration, but it rarely knows whether dinner is being cooked without ventilation, whether incense is burning, whether a child with asthma is in the bedroom nearest the road, or whether the only available cooling option is an open window.
That gap matters because families do not necessarily know which ordinary indoor activities are changing their exposure. In one survey of 143 participants, only 3% were aware that indoor activities affect air quality, and only 6% recognized cooking without ventilation as a problem.[1] Those numbers do not prove that personalized alerts prevent exacerbations. They do suggest that generic air quality messaging is leaving a great deal of actionable risk unspoken.

For readers looking for the monitoring and epidemiology side of this problem, ClinicalMind’s related article on Health Risks of Wildfire Smoke and AI Air Quality Monitoring covers the broader evidence on wildfire smoke harms and AI-enabled detection. The narrower question here is what happens after a signal is detected: whether AI can turn sensor data into family-specific safety advice, and whether that advice has been shown to improve health.
What AI Adds Between an Alert and a Family Decision
The technical case for AI-powered safety tips is stronger than the clinical case. Machine learning systems can combine outdoor monitoring, indoor sensors, time patterns, pollutant histories, and household context to estimate near-term exposure more locally than public AQI reports. Several model classes have been reported in this space, including Random Forest, Decision Trees, LSTM networks, XGBoost, and Gradient Boosting. In reported applications, Random Forest reached 98.2% accuracy and Decision Trees reached 99.8% accuracy for pollutant prediction, while LSTM models were used for temporal forecasting.[2][3]
Those figures are useful, but they should not be asked to carry more than they measure. Prediction accuracy says the system can estimate pollutant levels or AQI states under the conditions tested. It does not say that a caregiver opened a window at the right time, that a child used a controller medication differently, that an asthma flare was prevented, or that emergency department use declined.
| Pipeline step | What current evidence supports | What remains unproven |
|---|---|---|
| Prediction | ML models can forecast pollutants or AQI at hyperlocal or indoor scales with high reported accuracy in selected studies. | Many systems are not validated against downstream clinical outcomes. |
| Explanation | SHAP and LIME can identify which measured features appear to drive a household’s pollution exposure. | Explanations may be technically correct without being clinically actionable. |
| Recommendation | Systems can translate drivers such as cooking, smoking, incense, AC use, VOC, NO₂, and PM₁₀ into targeted advice. | Advice may cross into individualized health guidance without regulatory authorization. |
| Behavior | A small pediatric asthma pilot showed children taking actions after app notifications. | Engagement durability and generalizability remain uncertain. |
| Health outcome | Risk stratification tools can identify children at higher respiratory risk before alerts occur. | No large-scale RCTs show fewer exacerbations, ED visits, or hospitalizations from AI-generated safety tips. |
The practical value begins when prediction becomes specific enough to support a different action. A family does not need an algorithm to say “air quality is poor” if the same statement already appears in a public alert. The more useful version is narrower: the kitchen particle level rose after cooking; the child’s bedroom is improving after filtration; the outdoor air is worse than the living room; opening a window now is likely to increase exposure; running AC may be the safer cooling option if filtration and recirculation are available.
From Pollutant Forecasts to Household-Specific Advice
A typical AI recommendation pipeline starts with measurement. Low-cost sensors may collect particulate matter, volatile organic compounds, nitrogen dioxide, temperature, humidity, or room-level trends. The model then estimates a current or near-term exposure state. If the system is designed only to forecast pollutant concentration, it can notify the family that risk is elevated. If it also uses explainable AI, it can begin to say why.
That distinction is important. SHAP and LIME are not magic layers of clinical wisdom; they are methods for attributing a model’s output to measured features. In indoor air quality research, these methods identified household activities and environmental signals such as cooking, smoking, incense burning, AC usage, VOC, NO₂, and PM₁₀ as influential contributors to exposure estimates.[1] The clinical promise is not the explanation itself. It is the possibility that the explanation makes the recommendation less generic.
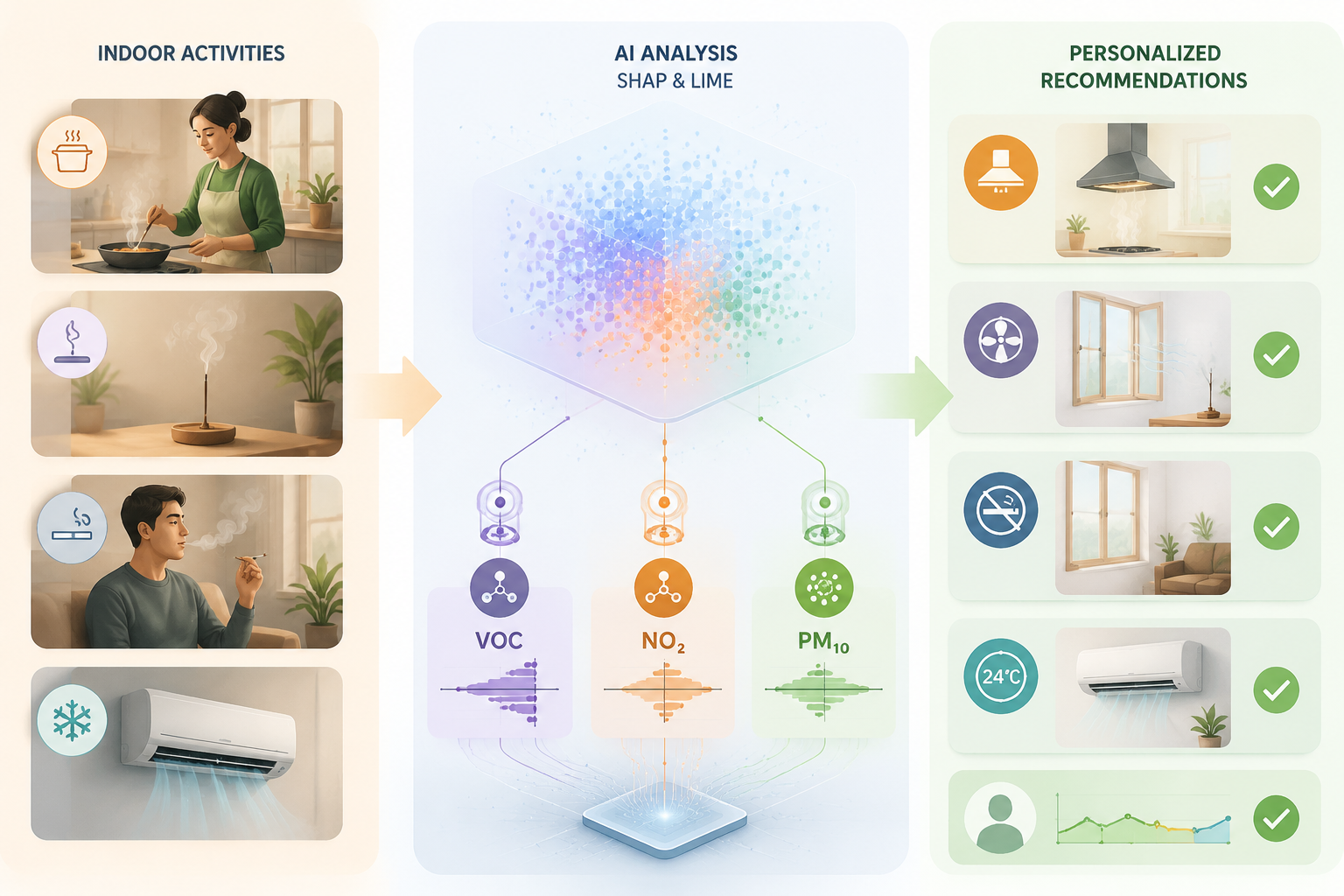
A generic alert might say, “Limit exposure.” A feature-aware system could say, “Particle levels rose after cooking; use the range hood if available, move the child with asthma away from the kitchen, and check whether bedroom levels fall before sleep.” Another household might receive different advice because incense, tobacco smoke, or outdoor infiltration is the dominant measured driver. These are plausible safety tips because they ask someone to change a concrete exposure pathway, not simply to feel warned.
The strongest version of this approach would also respect constraints. A recommendation to close windows may be unsafe or unrealistic during heat if a family lacks air conditioning. A recommendation to use an air purifier may be irrelevant if the household cannot afford one or cannot place it in the child’s sleeping area. A useful AI system would need to know enough about housing, ventilation, cooling, and school schedules to avoid issuing advice that sounds precise but is not usable.
AirBuddy Shows the Most Concrete Behavioral Signal
AirBuddy is the case that most clearly moves beyond prediction into observed action. In the Rutgers study published in 2022, the mobile app connected indoor air quality sensors with AI-powered push notifications for children with asthma. The study enrolled seven children, ages 8 to 12, from a single urban pediatric hospital setting. When indoor air quality worsened, children reported taking protective actions such as turning on air conditioning or opening windows.[4]

That is a small but meaningful observation. A child changing a room-level behavior after a sensor-linked prompt is closer to the desired intervention than a model reporting high accuracy on a held-out dataset. It shows a behavioral pathway: detect a deterioration, notify the user, prompt an action, and potentially reduce exposure.
The same study also illustrates why feasibility should not be mistaken for proof of protection. The sample was n=7. The setting was one urban pediatric hospital. Engagement declined over eight weeks without gamification features.[4] The study was not designed to show fewer asthma exacerbations, fewer urgent visits, or better lung function. It supports the claim that AI-linked indoor air quality feedback can prompt some children with asthma to act. It does not support the claim that the app made school days safer or reduced emergency care.
The engagement finding deserves more attention than it usually gets. Air quality safety advice is not a one-time instruction like “take this antibiotic for ten days.” Families may need alerts during cooking, wildfire smoke, traffic peaks, sleep, school pickup, heat events, and respiratory viral season. If attention fades over weeks, the intervention may become least reliable precisely when families need it to be routine.
Risk Stratification Before the Alert
Personalization does not have to begin at the moment a sensor detects poor air. It can begin earlier, with identifying which children are more vulnerable when an alert occurs. Mayo Clinic researchers reported AI tools using machine learning and natural language processing trained on electronic health records from more than 22,000 children to identify high-risk asthma subtypes by age 3. Children in the high-risk subgroup had more than twice the pneumonia rates and nearly three times the influenza rates.[5]
That kind of tool is not an air quality recommendation system. Its role is upstream. It could help clinicians or health systems identify children who may need more anticipatory counseling before wildfire season, pollution alerts, or school-based exposure concerns. Used carefully, risk stratification could help decide whose family receives more intensive education, sensor support, or follow-up. Used carelessly, it could be oversold as if identifying risk were the same as reducing it.
Community Monitoring Is Not the Same as Family Personalization
The UNICEF and Arm deployment in Laos shows another useful boundary. In 2025, 148 AI-enabled real-time air quality sensors were installed in schools, using open-source machine learning models to analyze PM2.5 data, with public availability through AirGradient and OpenAQ.[6] That is a credible community-level feasibility example. It can improve visibility where monitoring infrastructure is limited.
It should not be treated as evidence that families received individualized recommendations or that children with asthma had better outcomes. A school sensor network can tell a community more about exposure. It cannot, by itself, know which child slept next to an open window, which household is cooking without ventilation, or which caregiver can realistically change the pickup route. Community monitoring is a necessary layer in many settings, but it is not the same intervention as AI-generated family safety guidance.
What Clinicians Would Need the System to Say
Clinical communication literature points toward a better design standard. Slavik and colleagues recommend using AQI visuals and stories, emphasizing near-term health benefits, and identifying barriers to clean indoor air when counseling families about air pollution and children’s health.[7] An AI system could automate parts of that work: translate readings into simple visuals, connect advice to near-term symptoms or activity choices, and ask about barriers before recommending an action.
The key word is “could.” A system that says “air quality is unhealthy” has done little more than repackage an alert. A system that says “PM levels in the child’s bedroom have stayed elevated since cooking; if available, run ventilation in the kitchen and keep the child in the room with the lowest reading for the next hour” has begun to behave like a decision aid. The recommendation is still environmental guidance, not asthma management, unless it tells the family to change medications, alter a written asthma action plan, or make individualized clinical decisions.
- Useful safety tips name the exposure source, the room or timing affected, and the specific action available to the family.
- Safer systems distinguish environmental actions from individualized medical advice.
- Equity-sensitive systems ask whether filtration, air conditioning, ventilation, or relocation is feasible before recommending it.
- Clinically credible systems track whether the recommendation was seen, whether behavior changed, and whether symptoms or utilization changed afterward.
The Outcome Evidence Gap
The evidence chain is currently uneven. Prediction and personalization feasibility are relatively well supported. Behavior change has a small pediatric asthma signal, most clearly in AirBuddy. Health outcomes are where the chain thins out. The reviewed evidence does not include large-scale randomized trials directly measuring whether AI-generated personalized safety tips during air quality alerts reduce asthma exacerbations, respiratory events, emergency department visits, or hospitalizations.
That absence matters because every step in the chain can fail quietly. A model can predict well but alert too often. An explanation can identify cooking as a driver but recommend ventilation when outdoor air is worse. A child can tap through a notification without changing location. A caregiver can intend to act but lack AC, filtration, transportation flexibility, or authority over a school environment. A pilot can show enthusiasm in week one and attrition by week eight.
There is also a regulatory boundary. None of the reviewed AI recommendation systems have FDA clearance, CE marking, or equivalent authorization for generating individualized health recommendations. That does not make environmental safety prompts inappropriate. It does mean clinicians, health systems, and vendors should avoid presenting these tools as proven medical interventions unless they have been evaluated and authorized for that use.
What Would Count as Stronger Evidence
The next evidentiary step is not another demonstration that a model can classify air quality accurately under favorable conditions. For family safety during alerts, the more important question is whether the system changes exposure-relevant behavior and whether that change is durable enough to matter clinically.
A stronger study would enroll enough families to compare AI-personalized recommendations with usual AQI messaging or nonpersonalized sensor feedback. It would define the population clearly, especially asthma severity, age, housing conditions, and baseline access to filtration or cooling. It would measure not only app engagement but also actual protective actions, indoor pollutant changes, symptom days, rescue medication use if appropriate to the protocol, urgent visits, emergency department visits, and hospitalizations. It would need enough follow-up to see whether families keep responding after the novelty of alerts fades.
External validation is just as important. A system developed in one housing stock, climate, sensor configuration, or pediatric asthma clinic may not perform the same way in rural homes, multifamily buildings, schools without mechanical ventilation, or regions where wildfire smoke and heat co-occur. If the model’s advice depends on AC use, window opening, or indoor pollutant sources, the study setting is not a minor detail; it is part of the intervention.
Where the Evidence Leaves Families and Clinicians
AI can already generate plausible, personalized, real-time safety tips for families during air quality alerts. The most defensible use is as an environmental decision aid: connect sensor readings to room-level and activity-level recommendations, make the reason for the advice visible, and help families act on risks they would otherwise miss. Pediatric asthma is the area where the rationale is strongest, because susceptibility is higher, the behavioral pathway is concrete, and early pilot evidence shows children can respond to prompts.
The boundary is equally clear. High prediction accuracy is not evidence of fewer asthma attacks. Explainability is not evidence of better health. A small feasibility study is not a clinical outcomes trial. As of Q3 2026, the evidence supports promise and careful deployment as decision support, not claims that AI-powered safety tips have been proven to reduce respiratory events, emergency department visits, or hospitalizations during air quality alerts.
References
- arXiv:2501.06222v1. arXiv. 2025.
- Rajesh et al. 2025. PubMed Central. 2025.
- Artificial intelligence in indoor air quality. PubMed Central.
- AirBuddy: A Mobile App for Children With Asthma to Monitor Indoor Air Quality. JMIR Formative Research. 2022.
- Mayo Clinic AI tools identify children at high risk of asthma-related infections. Mayo Clinic. 2025.
- UNICEF and Arm deploy AI-enabled air quality monitoring in schools in Lao PDR. UNICEF Innovation. 2025.
- Air pollution and children’s health: a clinician communication framework. BMJ Paediatrics Open. 2023.
Comments
Join the discussion with an anonymous comment.